
Arthroscopy-assisted DG-lock suture fixation offers a minimally invasive, hardware-free method for managing patellar osteochondral fractures, providing stable fragment fixation, preserving cartilage integrity, and facilitating early rehabilitation with favourable clinical outcomes.
Dr. Ajit S Rathod, Department of Orthopaedics, Grant Government Medical College and Sir J.J. Group of Hospitals, Mumbai, Maharashtra, India. E-mail: ajit.rathod.5659@gmail.com
Abstract
Introduction: Patellar osteochondral fractures (OCFs) commonly occur following acute lateral patellar dislocation and have traditionally been managed using metallic or bioabsorbable implants, which may abrade cartilage or require later removal. This case demonstrates an alternative management in the form of an arthroscopic-assisted suture-based fixation of patellar OCFs using the DG-lock suturing.
Case Report: A 17-year-old male who presented to our facility with pain and deformity of the knee following a self-fall. On examination, tenderness was present over the medial aspect. On radiographic imaging, findings were suggestive of inferomedial patellar OCF. After meticulous planning, the patient underwent arthroscopy-assisted reduction and suture-based fixation using the DG-lock suturing technique. Arthroscopy allowed identification of the avulsed fragment, which was displaced and adherent to the lateral femoral condyle within a haematoma. After arthroscopic localisation and mobilisation, the fragment was fixed using multiple high-strength suture loops through transosseous patellar tunnels, providing broad compression without articular hardware. Early range of motion and full weight-bearing in a hinged brace were initiated post-operatively, resulting in radiographic union and return to activity by 10–12 weeks. Post-operative outcomes of DG-lock suturing demonstrated favourable results compared to conventional methods, such as the standard metallic and bioabsorbable implants used for OCF management.
Conclusion: Arthroscopy-assisted DG-lock suture fixation offers a minimally invasive, hardware-free method for managing patellar OCFs. It provides fragment-preserving compression, reduces soft-tissue trauma, and enables early rehabilitation, making it a viable and novel alternative to metallic implants.
Keywords: Patella, osteochondral fracture, arthroscopic-assisted fixation, DG-lock suturing, suture-based fixation.
Osteochondral fractures (OCFs) of the patella frequently accompany acute lateral patellar dislocations, particularly in adolescents and young athletes [1,2,3]. Early anatomical reduction and stable fixation are essential to restore joint congruity and prevent secondary chondral degeneration [1]. Patients usually present with an associated knee effusion secondary to hemarthrosis and medial retinacular tenderness [4].
Conventional fixation methods using metallic screws, pins, or bioabsorbable implants can violate fragile osteochondral fragments; cause articular cartilage abrasion, synovitis, or implant prominence; and may necessitate a secondary procedure for removal [1,5].
Arthroscopy-assisted fixation has recently gained prominence as it allows direct visualisation of the lesion, removal of intra-articular haematoma, and precise anatomical reduction with minimal soft-tissue disruption. When combined with modern suture-based fixation methods, such as the DG-lock suturing technique, this approach provides broad-surface compression without hardware placement in the joint. The arthroscopic-assisted DG-lock construct standardises a reproducible, minimally invasive, and fragment-preserving fixation for small- to mid-sized patellar OCFs, enabling early motion and reliable union while minimising complications associated with hardware [6].
A skeletally mature 17-year-old male presented after a 1st-time lateral patellar dislocation with haemarthrosis and medial retinacular tenderness; magnetic resonance imaging (MRI) revealed a 20 × 16 mm osteochondral fragment from the inferomedial patellar facet with a corresponding donor site and typical bone oedema pattern. Radiographs and computed tomography localised a loose body in the suprapatellar recess, and instability risk factors were documented without the need for tubercle transfer in this isolated case (Fig. 1).
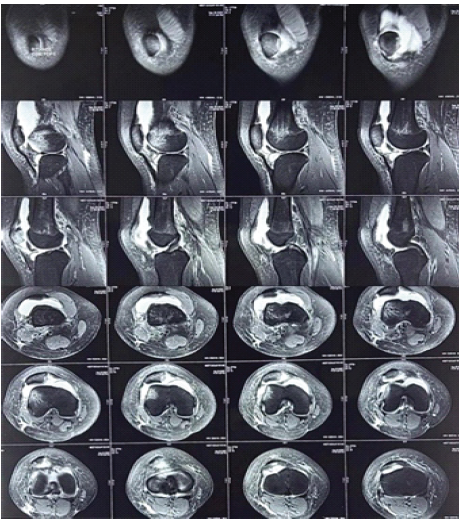
Figure 1: Pre-operative magnetic resonance imaging knee – axial and coronal views depicting 20 × 16 mm osteochondral fragment from the inferomedial patellar facet with a corresponding donor site and typical bone edema pattern.
Indications and planning:
Given fragment size, viability, and donor-bed freshness within 10 days, primary fixation was indicated to restore congruency; the planned technique was an arthroscopy-assisted open subvastus approach with fragment-preserving, transosseous suture fixation using a DG-lock multi-loop construct.
Surgical technique:
The patient was administered combined spinal anaesthesia. A pneumatic tourniquet was applied on the proximal thigh, and standard aseptic preparation of the limb was performed. Initial diagnostic arthroscopy was carried out mainly to retrieve the fragment and also helped to assess the fracture morphology, feasibility of fixation, and exact location of the chondral defect. The medial patellar donor defect was clearly identified intraoperatively (Fig. 2a), and transosseous tunnel planning was performed using one central and four peripheral drill tunnels framing the defect (Fig. 2b). The osteochondral fragment was found avulsed from the medial patellar margin and displaced laterally, adherent to the lateral femoral condyle within an organised haematoma. Owing to this displacement and adhesion, arthroscopic retrieval was technically difficult without extensive exposure (Fig. 2c). An arthroscopy-assisted DG-lock suture-bridge fixation was therefore planned. Through a minimally invasive subvastus approach, the fragment was carefully released from the lateral condyle and mobilised to its anatomical position without injuring the vastus medialis obliquus (VMO). The osteochondral fragment was then temporarily reduced and positioned within the donor defect before definitive fixation (Fig. 2d). Under arthroscopic guidance, the fragment was anatomically reduced to the donor site on the medial patella. Transosseous DG-lock multi-loop sutures were used to achieve uniform compression and stable fixation (Fig. 2f). The components of the transosseous DG-Lock multi-loop sutures consist of the following:
- A: The central pilot needle
- B: The lead sutures (4 in number)
- C: The fixation node
- D: The protection ring
- E: The peripheral fixation sutures (4 in number)
- F: The peripheral fixation needles (4 in number) (Fig. 2).
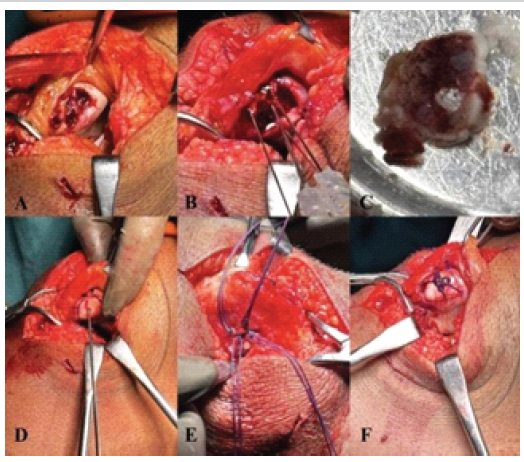
Figure 2: Intra-operative clinical images depicting. (a) Defect present over the medial aspect of the patella. (b) One 1.8-mm central and four 1.2-mm peripheral diagonally opposite tunnels were drilled to frame the defect. (c) Isolated osteochondral fracture fragment. (d) Fragment placed and fixed in the defect temporarily. (e) High-strength sutures were passed through tunnels in crossing and parallel configurations. (f) Knots were tied securely over the anterior periosteum, ensuring no contact with the articular cartilage.
One 1.8-mm central and four 1.2-mm peripheral diagonally opposite tunnels were drilled to frame the defect, through which high-strength sutures were passed in crossing and parallel configurations. High-strength sutures were passed through the transosseous tunnels in crossing and parallel configurations (Fig. 2e). Knots were then tied securely over the anterior periosteum, ensuring no contact with the articular cartilage (Fig. 2f). Final arthroscopic inspection confirmed congruent articular reduction and stable fixation through a full range of motion. Immediate postoperative radiographs confirmed satisfactory reduction and fixation of the osteochondral fragment (Fig. 3).
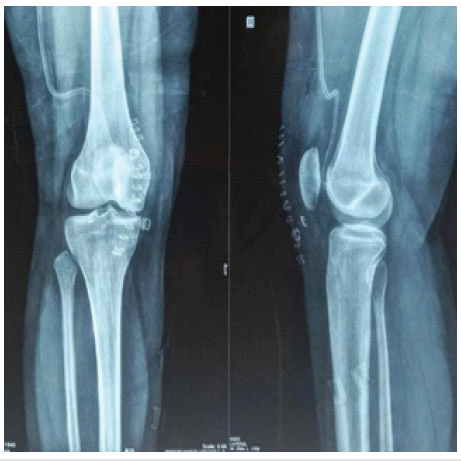
Figure 3: Immediate post-operative X-ray knee anteroposterior and lateral view.
Advantages:
- Arthroscopy allowed accurate localization of the displaced fragment and avoided unnecessary extensile exposure of the extensor mechanism
- The minimally invasive subvastus approach preserved the VMO and facilitated early recovery
- Reduced post-operative pain, reduced blood loss, and shorter operative time
- Early rehabilitation enabled by secure, hardware-free fixation.
Post-operative protocol:
A hinged brace locked at 0–30° was used for 2 weeks with immediate partial weight-bearing; the range was advanced to 90° by 6 weeks, and the brace was discontinued thereafter, consistent with suture-fixation pathways that allow early motion due to secure compression without implant prominence [7,8]. Strengthening began by 4–6 weeks, with a progressive return to running by 10–12 weeks if imaging and the exam confirmed stability (Fig. 4).

Figure 4: Post-operative 3-month follow-up clinical images depicting near complete flexion and extension, and the ability to sit in a cross-legged position comfortably.
Outcomes:
Radiographs at 3 months and MRI at 10–12 weeks demonstrated union and articular congruity without synovitis or implant-related abrasion; clinically, pain resolved, no re-dislocation occurred, and functional recovery allowed sport-specific drills by 3 months, mirroring outcomes reported for crossing sutures and fragment-preserving constructs (Fig. 5). No anterior patellar bursitis or effusion was observed, though this is a recognised consideration after transosseous suture fixation in series using absorbable strands.
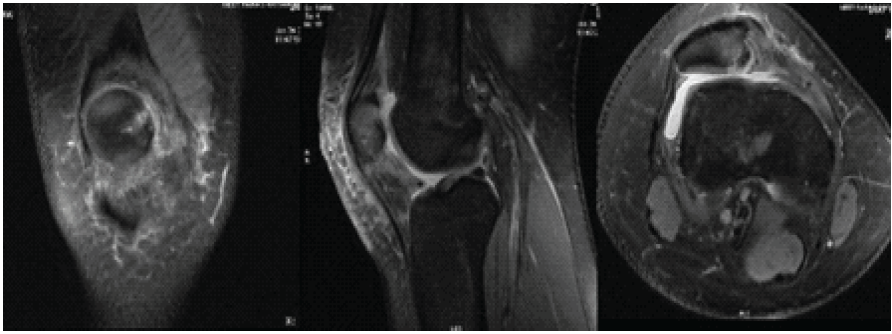
Figure 5: Three months later, post-operative magnetic resonance imaging films of the right knee depicting bony union and reduced edema.
Rationale for arthroscopic-assisted suture-based fixation:
Arthroscopic-assisted fixation provides direct visualisation of the articular surface, precise identification of displaced fragments, and minimally invasive management of haemarthrosis and intra-articular debris. Combining arthroscopy with a suture-based DG-lock construct avoids violating delicate osteochondral fragments while eliminating articular hardware, thereby reducing the risks of cartilage abrasion, implant prominence, and the need for hardware removal associated with metallic or bioabsorbable devices. Crossing-suture techniques via small transosseous tunnels provide stable compression for small- to medium-sized fragments, while the DG-lock configuration distributes load evenly with central nodes or loops that minimise cut-through in thin osteochondral tissue.
Comparison with implants:
While metallic screws or bioabsorbable pins can achieve point fixation, meta-analyses suggest variable outcomes and complication profiles since they require larger bone purchase and carry risks of cartilage wear, synovitis, or implant reaction [9]. Bioabsorbable fixation techniques, although eliminating the need for implant removal, have been associated with inflammatory reactions and variable healing outcomes in some series [10]. In contrast, arthroscopic-assisted suture-bridge fixation enables broad, uniform compression without violating the articular surface and ensures fragment preservation. The concept of suture fixation for patellar osteochondral fractures was originally described by Pritsch et al., who demonstrated successful fragment stabilisation without metallic implants [11]. For patellar lesions, tying sutures over the anterior cortex through ≤2 mm tunnels achieves secure fixation with low risk of iatrogenic fracture, and the arthroscopic view allows accurate assessment of reduction and congruity throughout the range of motion. This approach also integrates effectively with concurrent instability or soft-tissue procedures when indicated.
Technique pearls for arthroscopic-assisted DG-lock construct:
Fixation should ideally be performed within 2 weeks of injury to preserve fragment viability. Initial arthroscopy aids in identifying and freeing fragments trapped within the haematoma or the lateral compartment. After reduction, small perpendicular transosseous tunnels are drilled framing the donor crater. At least four loops – arranged in diagonal and parallel orientation – are used for uniform compression. Gradual tensioning without sliding avoids cartilage abrasion, and knots are tied over the periosteum for secure fixation. Arthroscopy confirms anatomical reduction, ensuring smooth articular contour before closure. For thin or irregular fragments, multiple suture loops enhance load distribution and prevent cut-through [6].
Limitations and indications:
Arthroscopic-assisted DG-lock suture fixation is best suited for acute, viable osteochondral fragments of small to moderate size. Chronic, ischaemic, or osteochondritis dissecans-type lesions may require alternative methods, though hybrid techniques using knotless suture anchors or partial open approaches can extend its applicability [12]. Surgeons should be aware of potential anterior bursal irritation from transosseous tunnels and follow a cautious rehabilitation protocol to protect the repair during early healing.
Arthroscopy-assisted DG-lock suture fixation represents an effective and minimally invasive technique for managing patellar OCFs. It provides stable, fragment-preserving fixation without the need for intra-articular hardware, thereby reducing implant-related complications. This technique allows early mobilisation, promotes reliable healing, and may serve as a valuable alternative to conventional fixation methods in appropriately selected cases.
Arthroscopy-assisted DG-lock suture fixation is a reliable, hardware-free option for patellar osteochondral fractures that enables anatomical reduction, stable fixation, and early rehabilitation while minimizing implant-related complications.
References
- 1. Ng WM, Al-Fayyadh MZ, Kho J, Seow Hui T, Mohamed Ali MR. Crossing suture technique for the osteochondral fractures repair of patella. Arthrosc Tech 2017;6:e1035-9. [Google Scholar] [PubMed]
- 2. Milgram JW, Rogers LF, Miller JW. Osteochondral fractures: Mechanisms of injury and fate of fragments. AJR Am J Roentgenol 1978;130:651-8. [Google Scholar] [PubMed]
- 3. Lee BJ, Christino MA, Daniels AH, Hulstyn MJ, Eberson CP. Adolescent patellar osteochondral fracture following patellar dislocation. Knee Surg Sports Traumatol Arthrosc 2013;21:1856-61. [Google Scholar] [PubMed]
- 4. Kramer DE, Pace JL. Acute traumatic and sports-related osteochondral injury of the pediatric knee. Orthop Clin North Am 2012;43:227-36. [Google Scholar] [PubMed]
- 5. Enea D, Busilacchi A, Cecconi S, Gigante A. Late-diagnosed large osteochondral fracture of the lateral femoral condyle in an adolescent: A case report. J Pediatr Orthop B 2013;22:344-9. [Google Scholar] [PubMed]
- 6. Goyal D. Suture-based technique for patellar osteochondral fractures fixation using an all-absorbable implant. Arthrosc Tech 2025;14:103896. [Google Scholar] [PubMed]
- 7. Vogel LA, Fitzsimmons KP, Lee Pace J. Osteochondral fracture fixation with fragment preserving suture technique. Arthrosc Tech 2020;9:e761-7. [Google Scholar] [PubMed]
- 8. Li ZX, Song HH, Wang Q, Guo DM. Clinical outcomes after absorbable suture fixation of patellar osteochondral fracture following patellar dislocation. Ann Transl Med 2019;7:173. [Google Scholar] [PubMed]
- 9. Kuhle J, Angele P, Balcarek P, Eichinger M, Feucht M, Haasper C, et al. Treatment of osteochondral fractures of the knee: A meta-analysis of available scientific evidence. Int Orthop 2013;37:2385-94. [Google Scholar] [PubMed]
- 10. Millington KL, Shah JP, Dahm DL, Levy BA. Bioabsorbable fixation of unstable osteochondritis dissecans lesions. Am J Sports Med 2010;38:2065-70. [Google Scholar] [PubMed]
- 11. Pritsch M, Velkes S, Levy O, Greental A. Suture fixation of osteochondral fractures of the patella. J Bone Joint Surg Br 1995;77:154-5. [Google Scholar] [PubMed]
- 12. Ishibashi Y, Kimura Y, Sasaki S, Sasaki E, Takahashi A. Internal fixation of osteochondritis dissecans using pushlock suture anchors. Arthrosc Tech 2021;10:e705-9. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Single-Stage Treatment of a Patellar Osteochondral Defect in an Adolescent Using Autologous Minced Cartilage – Platelet-Rich Plasma Scaffold Technique: A Case Report and Technical Considerations
March 1, 2026 Single-Stage Treatment of a Patellar Osteochondral Defect in an Adolescent Using Autologous Minced Cartilage – Platelet-Rich Plasma Scaffold Technique: A Case Report and Technical Considerations January 1, 2026 Aneurysmal Bone Cyst-cloaked Codman’s Tumor in the Patella: Case Report of an Easily Misdiagnosed Entity
January 1, 2026 Aneurysmal Bone Cyst-cloaked Codman’s Tumor in the Patella: Case Report of an Easily Misdiagnosed Entity October 1, 2025 Osteochondral Fragment from the Lateral Femoral Condyle in an Adult after Patellar Dislocation: A Surgical Challenge
October 1, 2025 Osteochondral Fragment from the Lateral Femoral Condyle in an Adult after Patellar Dislocation: A Surgical Challenge July 1, 2025 Management of Large Osteochondral Fracture of the Patella in an Adolescent: A Rare Case Report
July 1, 2025 Management of Large Osteochondral Fracture of the Patella in an Adolescent: A Rare Case Report