
Percutaneous Achilles tenotomy using an 18-gauge needle is a safe, cost-effective, and minimally invasive technique that achieves excellent clinical correction and complete ultrasonographic tendon healing in children with idiopathic clubfoot.
Dr. Ankur Kumar, Department of Orthopedics, Nandkumar Singh Chouhan Government Medical College, Khandwa, Madhya Pradesh, India. E-mail: drankurkumar96@gmail.com
Abstract
Introduction: Percutaneous Achilles tenotomy is a critical step in the Ponseti method for correcting residual equinus deformity in idiopathic clubfoot. Needle tenotomy has emerged as a minimally invasive alternative to conventional scalpel-based tenotomy, offering potential advantages in safety, procedural cost, and ease of performance. Prospective combined clinical and ultrasonographic evidence evaluating this technique from Indian centres remains limited.
Objective: The aim of the study was to evaluate the clinical and ultrasonographic outcomes of percutaneous Achilles tenotomy using an 18-gauge needle in children with idiopathic clubfoot managed by the Ponseti method.
Materials and Methods: This prospective study included 45 children (76 ft) with idiopathic congenital talipes equinovarus. Serial Ponseti casting was performed until residual equinus was the only deformity remaining, after which percutaneous Achilles tenotomy was performed using an 18-gauge needle under general anaesthesia. Patients were evaluated preoperatively and at 3 weeks, 2 months, 6 months, and 1 year using the Pirani score, passive dorsiflexion angle at the ankle, and foot bimalleolar angle on podogram. Ultrasonography was performed at the 3-week follow-up to assess tendoachilles healing.
Results: The mean age at tenotomy was 7.3 ± 2.76 months, with male predominance (71.11%) and bilateral involvement in 68.89% of cases. On ultrasonography at 3 weeks, 14 of 76 ft (18.42%) showed a tendon defect, and 9 of 76 ft (11.84%) showed peri-tendinous collections; both abnormalities resolved by the 2-month follow-up. The mean Pirani score improved significantly from 2.11 ± 0.40 preoperatively to 0 at 1 year (t = 42.93, df = 66, P < 0.05). The mean passive dorsiflexion angle improved from 128.74° ± 12.04° to 76.21° ± 2.15° (mean difference 52.53° ± 11.57°; t = 36.90, df = 65, P < 0.05), and the mean foot bimalleolar angle improved from 70.09° ± 2.70° to 81.74° ± 1.58° (t = −48.96, df = 65, P < 0.05). Forty patients (88.90%) maintained correction without additional surgery; four patients (8.88%) required posteromedial soft-tissue release, and one patient (2.22%) required unilateral tendoachilles lengthening.
Conclusion: Percutaneous Achilles tenotomy using an 18-gauge needle is a safe, effective, and minimally invasive technique for correcting residual equinus in idiopathic clubfoot. The procedure yields favourable clinical correction, satisfactory ultrasonographic tendon healing, and a low rate of secondary surgical intervention.
Keywords: Clubfoot, congenital talipes equinovarus, ponseti method, needle tenotomy, achilles tenotomy, ultrasonography, pirani score.
Idiopathic congenital talipes equinovarus (CTEV), commonly known as clubfoot, is one of the most prevalent congenital musculoskeletal deformities, occurring in approximately 1 in 1,000 live births worldwide [1]. The deformity is characterised by four cardinal components – cavus (high-arched foot), adduction (medial deviation of the forefoot), varus (hindfoot inversion), and equinus (plantarflexion) – and when left untreated, results in significant functional disability and gait impairment [1,2]. The Ponseti method of serial manipulation and casting has become the globally accepted standard of care for idiopathic clubfoot, achieving correction through gentle, biomechanically sound manipulation that exploits the plasticity of neonatal connective tissue and cartilaginous tarsal bones while minimising the need for extensive soft-tissue surgery [2]. Despite successful correction of cavus, adduction, and varus by serial casting, residual equinus persists in approximately 80–90% of cases and requires Achilles tenotomy to achieve a plantigrade foot [2,3]. Ponseti originally performed tenotomy using an ophthalmic scalpel; subsequent surgeons adopted the No. 15 blade with satisfactory results [2]. However, percutaneous scalpel tenotomy carries a risk of haemorrhagic and neurovascular complications arising from posterior tibial vessel variations [4,5]. In response, several alternative techniques have been described: Mini-open tenotomy under direct visualisation [6], botulinum toxin injection to the triceps surae [7], keratome-based tenotomy [8], and percutaneous needle tenotomy [3]. The concept of large-gauge needle tenotomy was introduced by Minkowitz et al. in 2004, who used a precision-glide needle as a safe, cost-effective, office-based alternative to blade tenotomy [3]. The needle technique employs the bevelled tip in a controlled sawing motion to divide tendon fibres with minimal collateral soft-tissue trauma. A subsequent systematic review by Dhingra et al. demonstrated a pooled success rate of 95% across 1,026 ft with a complication rate of 0.04% [9]. Despite this evidence, prospective studies combining serial clinical assessment with ultrasonographic documentation of tendon healing remain relatively scarce, particularly from resource-limited settings [10,11]. Although percutaneous Achilles tenotomy using a surgical blade is conventionally performed as an outpatient procedure with satisfactory outcomes, concerns regarding bleeding, inadvertent neurovascular injury, and soft-tissue trauma still persist, particularly in infants with small anatomical dimensions and vascular variations. The use of an 18-gauge needle has been proposed as a minimally invasive and potentially safer alternative because the bevelled needle tip permits controlled division of tendon fibres with minimal collateral tissue injury, reduced bleeding risk, and lower procedural cost without requiring specialised surgical instruments or operating-room setup. Furthermore, prospective data correlating clinical outcomes with serial ultrasonographic assessment of tendon healing remain limited. The present study was therefore undertaken to prospectively evaluate the clinical effectiveness, procedural safety, and ultrasonographic healing outcomes of percutaneous Achilles tenotomy using an 18-gauge needle in idiopathic clubfoot managed by the Ponseti method.
Study design and setting:
This prospective single-arm interventional study was conducted at the Department of Orthopaedics, N.S.C.B. Medical College and Hospital, Jabalpur, Madhya Pradesh, India, from July 15, 2021, to June 30, 2024. Institutional ethics committee approval was obtained before initiation, and written informed consent was taken from the parent or guardian of each participant.
Sample size:
The sample size was calculated using the formula n = z²s² / d², where z = 1.96 (95% confidence level [CI], α = 0.05), s = standard deviation (SD) of total Pirani score (0.85) [12], and d = 5% relative error (mean = 5.12), yielding a minimum required sample of 45 children.
Eligibility criteria:
Inclusion criteria:
Children aged up to 5 years with unilateral or bilateral idiopathic clubfoot who had undergone serial Ponseti casting until residual equinus remained as the only deformity.
Exclusion criteria:
Children with neurogenic clubfoot, myelomeningocele, distal arthrogryposis, or acquired clubfoot.
Pre-operative assessment:
All children presenting to the CTEV clinic underwent clinical assessment and Pirani scoring [13]. Serial Ponseti casting was performed at weekly intervals [2]. When residual equinus was the only remaining deformity, pre-anaesthetic fitness was obtained, and the child was admitted for tenotomy. Preoperatively, the angle of passive dorsiflexion at the ankle was measured and video-recorded, and the foot bimalleolar angle was measured from a podogram.
Surgical technique:
All procedures were performed under general anaesthesia with the child supine, knee flexed to 90°, and the foot held in forced plantarflexion. The tendoachilles was palpated and marked. An 18-gauge needle (Dispo-van) was inserted from the medial to the lateral aspect of the tendon [3,14]. Using the bevelled tip in a controlled swinging (sawing) motion, the tendon was divided until a characteristic snap was felt, and passive dorsiflexion improved to the desired angle. A Plaster of Paris cast in overcorrection was applied for 3 weeks following tenotomy [2].
Post-operative management and follow-up:
At the 3-week follow-up, the cast was removed, and the Pirani score, passive dorsiflexion angle, and foot bimalleolar angle were reassessed. Ultrasonography of the tendoachilles was performed using an ALPINION E-CUBE-7 machine with a high-frequency linear probe (7.5–10 MHz) to evaluate tendon healing, tendon defect, and peri-tendinous collections [10,11]. Patients with inadequate correction at 3 weeks received an additional 1-week overcorrection cast before brace application. All other patients were fitted with Steenbeck’s foot abduction brace. Parents were instructed in brace wear (23 h/day until the child began walking, followed by night-time wear until 4–5 years of age) and home physiotherapy exercises, including dorsiflexion stretching and external rotation [2]. Subsequent follow-up visits were scheduled at 2 months, 6 months, and 1 year.
Outcome measures:
Primary clinical outcome measures were the Pirani score (range 0–6; 0 = complete correction) [13], passive dorsiflexion angle at the ankle (in degrees; smaller angle indicates greater dorsiflexion), and foot bimalleolar angle on podogram (normal ≥75°). The primary ultrasonographic outcome was assessment of tendoachilles continuity, tendon defect, and peri-tendinous collections at 3 weeks. Secondary outcomes were the need for additional casting at first follow-up, relapse rate, and requirement for further surgery (posteromedial soft-tissue release [PMSTR] or tendoachilles lengthening).
Statistical analysis:
Data were entered into Microsoft Excel and analysed using IBM Statistical Package for the Social Sciences version 23.0. Continuous variables were reported as mean ± SD and categorical variables as frequencies and percentages. The paired t-test was used to compare pre-operative and final follow-up values of continuous outcomes. A P < 0.05 was considered statistically significant.
A total of 45 children with idiopathic clubfoot involving 76 ft were enrolled and followed for a minimum of 1 year. All patients completed the full follow-up schedule.
Demographic and baseline characteristics:
The mean age at tenotomy was 7.3 ± 2.76 months. The majority underwent tenotomy in the 6–11 month age group (28 children, 62.22%), followed by the ≤5 months group (15 children, 33.33%) and the ≥12 months group (2 children, 4.44%). Male predominance was noted (32 males, 71.11%; 13 females, 28.89%). Bilateral involvement was present in 31 children (68.89%), right-sided in 8 (17.78%), and left-sided in 6 (13.33%). Thirty-three children (73.34%) were born by normal vaginal delivery and 12 (26.66%) by caesarean section (Table 1).
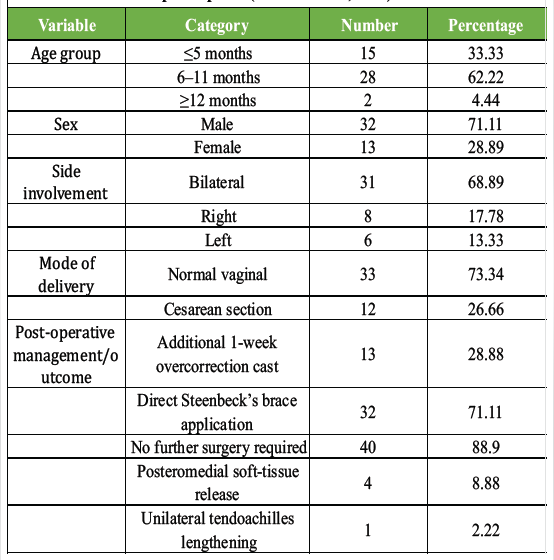
Table 1: Baseline characteristics and post-operative outcomes of study participants (n=45 children, 76 ft)
Ultrasonographic findings at 3 weeks:
All 76 ft were evaluated by ultrasonography at 3 weeks [10,11]. Fifty-three feet (69.74%) showed a normal study. Fourteen feet (18.42%) demonstrated a defect in the tendoachilles, and 9 ft (11.84%) showed peri-tendinous collections. All abnormalities had fully resolved by the 2-month follow-up, consistent with expected early tendon healing and remodelling after tenotomy [15,16]. These findings are presented in Table 2.
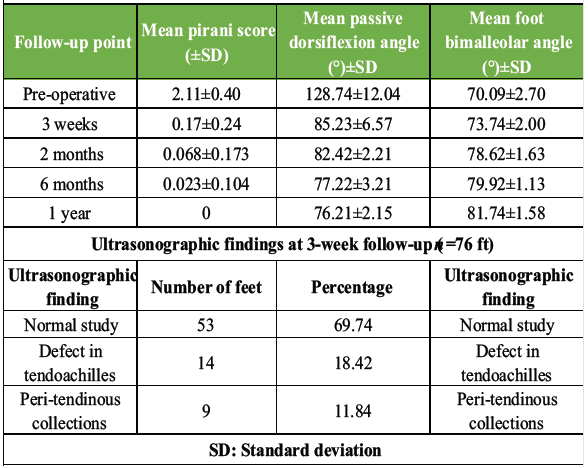
Table 2: Clinical and ultrasonographic outcomes following percutaneous achilles tenotomy
Pirani score:
The mean Pirani score was 2.11 ± 0.40 preoperatively and decreased progressively: 0.17 ± 0.24 at 3 weeks, 0.068 ± 0.173 at 2 months, 0.023 ± 0.104 at 6 months, and 0.00 at 1 year. The paired t-test demonstrated a statistically significant difference between pre-operative and 1-year values (t = 42.93, df = 66, P < 0.05, 95% CI). These results are presented in Table 1.
Passive dorsiflexion angle at the ankle:
The mean passive dorsiflexion angle was 128.74° ± 12.04° preoperatively, reflecting significant equinus deformity. Progressive improvement was observed post-tenotomy: 85.23° ± 6.57° at 3 weeks, 82.42° ± 2.21° at 2 months, 77.22° ± 3.21° at 6 months, and 76.21° ± 2.15° at 1 year. The mean improvement from pre-operative to 1 year was 52.53° ± 11.57° (t = 36.90, df = 65, P < 0.05). A smaller angle in this convention indicates greater ankle dorsiflexion (better correction). Results are presented in Table 1.
Foot bimalleolar angle:
The mean foot bimalleolar angle was 70.09° ± 2.70° preoperatively, below the normal threshold of 75°. Progressive improvement was documented: 73.74° ± 2.00° at 3 weeks, 78.62° ± 1.63° at 2 months, 79.92° ± 1.13° at 6 months, and 81.74° ± 1.58° at 1 year. The mean difference between pre-operative and 1-year values was −11.65° ± 1.93° (t = −48.96, df = 65, P < 0.05). Results are presented in Table 1.
Post-operative casting, bracing, and surgical outcomes:
At the 3-week follow-up, 13 patients (28.88%) required an additional 1-week overcorrection cast before brace application, while 32 patients (71.11%) were directly fitted with Steenbeck’s brace. During follow-up, five patients developed relapse: four (8.88%) required PMSTR, and one (2.22%) required unilateral tendoachilles lengthening. Forty patients (88.90%) maintained correction without any further surgical intervention [9,17,18,19]. The children requiring PMSTR were predominantly from the older age group (≥11 months). Outcomes are presented in Table 1.
The present study demonstrates that percutaneous Achilles tenotomy using an 18-gauge needle is a safe, effective, and minimally invasive technique for correcting residual equinus deformity in idiopathic clubfoot managed by the Ponseti method. The significant improvements in all three primary clinical outcome parameters – Pirani score, passive dorsiflexion angle, and foot bimalleolar angle – across serial follow-up support both immediate procedural efficacy and sustained maintenance of correction over 1 year. Clubfoot has a multifactorial aetiology involving genetic, environmental, and mechanical factors [1]. Residual equinus after serial casting reflects the inherent tightness of the Achilles tendon, which, unlike the joint capsule and ligaments, does not predictably respond to stretching alone [2,3]. Tenotomy resolves this tightness by creating a controlled discontinuity that heals with a regenerated, functionally competent tendon over 3–6 weeks [15,16]. The mean Pirani score decreased from 2.11 ± 0.40 preoperatively to 0 at 1 year, reflecting complete clinical correction across the cohort. These findings are consistent with prior needle tenotomy studies. Sharma et al. reported a mean pre-tenotomy Pirani score of 1.73, which decreased to 0.14 at 1 year follow-up [17]. Barkham et al. similarly reported a reduction from a mean pre-operative score of 1.5–0.5 at 1 year [18]. Dhingra et al., in a systematic review of eight studies encompassing 1,026 ft, reported a mean final Pirani score of 0 with a pooled success rate of 95% [9]. The serial and progressive decline in Pirani score at each interval further supports the sustained biological and mechanical effect of tenotomy in resolving residual hindfoot tightness. The passive dorsiflexion angle showed clinically and statistically significant improvement from pre-operative to 1 year (mean improvement 52.53° ± 11.57°), confirming successful release of equinus and maintenance of correction. Multiple comparable studies have confirmed that needle tenotomy consistently achieves post-procedure ankle dorsiflexion >15° [9,17,18]. Richetta et al., using the 18-gauge needle specifically, reported complete tendon division in all 36 tenotomies without any bleeding, pseudoaneurysm, or nerve injury, further supporting the safety of this specific gauge [19]. Rehman et al. demonstrated that tenotomy achieved satisfactory correction in a substantial proportion of feet requiring the procedure [14]. The foot bimalleolar angle improved progressively from 70.09° ± 2.70° preoperatively to 81.74° ± 1.58° at 1 year, surpassing the normal threshold of 75° as early as 2 months. Podogram-based measurement of the foot bimalleolar angle provides a clinically meaningful complement to the Pirani score and dorsiflexion measurements, documenting structural correction of foot alignment in addition to soft-tissue release – a finding that was maintained through the full follow-up period. Ultrasonographic assessment was an important strength of the present study. Although 18.42% of feet showed a tendon defect and 11.84% demonstrated peri-tendinous collections at 3 weeks, all abnormalities resolved by the 2-month follow-up, confirming satisfactory early tendon healing. Lebel et al. demonstrated that tendon continuity was achieved within 3–4 weeks after Ponseti-type tenotomy and that the healed tendon was comparable to the contralateral normal tendon at 2 years [16]. Saini et al., using magnetic resonance imaging, found complete resolution of intra-tendinous signal changes by 6 months with maintained passive dorsiflexion of at least 15° in all feet [15]. The absence of any major neurovascular complication in the present series is consistent with the established safety profile of needle tenotomy across published studies [9,19]. The reintervention rate of 11.1% compares favourably with published literature. Dhingra et al. reported only three recurrences in 16 prospective feet, attributable to poor brace compliance [9]. Barkham et al. reported a similarly low rate of further intervention in their prospective series [18]. The observation that children requiring PMSTR were predominantly from the older age group (≥11 months) is consistent with the principle that greater tissue rigidity in older infants may compromise long-term correction, underscoring the importance of early treatment initiation and strict adherence to the bracing protocol [1,2]. The practical advantages of 18-gauge needle tenotomy deserve emphasis in a tertiary teaching hospital context. The technique uses widely available, low-cost consumables, requires no specialised instruments, and is technically reproducible by surgeons at all levels of training. The absence of blade-related haemorrhagic or pseudoaneurysmal complications in the present series reinforces the safety data reported by Richetta et al. [19] and by the systematic review of Dhingra et al. [9]. While the mini-open technique provides direct tendon visualisation [6], it adds procedural complexity; by contrast, needle tenotomy achieves equivalent outcomes with a simpler, less morbid approach that is particularly suited to resource-limited and high-volume orthopaedic settings. The study has limitations. It was conducted at a single centre without a contemporaneous control arm, limiting direct comparison with blade tenotomy in the same population. The follow-up period of 1 year does not capture late relapse or long-term functional outcomes beyond early childhood. Ultrasonographic imaging beyond 2 months was not included in the study protocol. Future multicenter randomised controlled trials with longer follow-up and standardised functional scoring would further consolidate the evidence base for this technique.
Percutaneous Achilles tenotomy using an 18-gauge needle is a safe, effective, and minimally invasive technique for the correction of residual equinus in idiopathic clubfoot managed by the Ponseti method. The procedure provides satisfactory clinical correction with reliable tendon healing demonstrated on serial ultrasonographic evaluation. Owing to its technical simplicity, minimal soft-tissue trauma, cost-effectiveness, and reproducibility, the technique represents a practical alternative to conventional blade tenotomy, particularly in resource-limited and high-volume orthopaedic settings.
Percutaneous Achilles tenotomy using an 18-gauge needle is a safe, effective, and cost-efficient alternative to traditional scalpel-based methods for correcting residual equinus in idiopathic clubfoot. Clinical outcomes demonstrate significant improvements in Pirani scores and ankle dorsiflexion, with ultrasonographic evidence confirming that initial tendon defects and peri-tendinous collections typically resolve completely within 2 months. The technique’s low reintervention rate and minimal risk of neurovascular complications make it an ideal choice for high-volume or resource-limited orthopaedic settings. Furthermore, because secondary surgical interventions were primarily required in older infants, the study reinforces the importance of early intervention and strict adherence to post-procedure bracing protocols.
References
- 1. Dobbs MB, Gurnett CA. Update on clubfoot: etiology and treatment. Clin Orthop Relat Res 2009;467:1146-53. [Google Scholar] [PubMed]
- 2. Ponseti IV. Congenital Clubfoot: Fundamentals of Treatment. Oxford: Oxford University Press; 1996. [Google Scholar] [PubMed]
- 3. Minkowitz B, Finkelstein BI, Bleicher M. Percutaneous tendo-Achilles lengthening with a large-gauge needle: a modification of the Ponseti technique for correction of idiopathic clubfoot. J Foot Ankle Surg. 2004 Jul-Aug;43(4):263-5. doi: 10.1053/j.jfas.2004.05.012. [Google Scholar] [PubMed] [CrossRef]
- 4. Dobbs MB, Gordon JE, Walton T, Schoenecker PL. Bleeding complications following percutaneous tendoachilles tenotomy in the treatment of clubfoot deformity. J Pediatr Orthop 2004;24:353-7. [Google Scholar] [PubMed]
- 5. Burghardt RD, Herzenberg JE, Ranade A. Pseudoaneurysm following percutaneous tendoachilles tenotomy in a case of congenital clubfoot. J Foot Ankle Surg 2008;47:463-7. [Google Scholar] [PubMed]
- 6. MacNeille R, Hennrikus W, Stapinski B, Leonard G. A mini-open technique for Achilles tenotomy in infants with clubfoot. J Child Orthop. 2016 Feb;10(1):19-23. doi: 10.1007/s11832-016-0710-3. Epub 2016 Jan 29. PMID: 26825454; PMCID: PMC4763148. [Google Scholar] [PubMed] [CrossRef]
- 7. Alvarez CM, De Vera MA, Beauchamp RD, Ward V, Black AH. The use of botulinum toxin type A in the treatment of idiopathic clubfoot: Preliminary results and a comparison with a standard regimen of casting. J Pediatr Orthop 2005;25:149-56. [Google Scholar] [PubMed]
- 8. Goyal S, Sangwan SS, Gogna P, Singla R, Kundu ZS. Use of keratome 1-0 for percutaneous tendo Achilles tenotomy for correction of equinus deformity in club foot. J Clin Orthop Trauma 2014;5:115-6. [Google Scholar] [PubMed]
- 9. Dhingra M, Cazorla Bak Y, Edokpayi F, Chong HH, Shyamsundar S. A systematic review and single center experience with percutaneous needle tenotomy in congenital talipes equinovarus (CTEV). Cureus 2022;14:e32812. [Google Scholar] [PubMed]
- 10. Niki H, Nakajima H, Hirano T, Okada H, Beppu M. Ultrasonographic observation of the healing process in the gap after a Ponseti-type Achilles tenotomy for idiopathic congenital clubfoot at two-year follow-up. J Orthop Sci 2013;18:70-5. [Google Scholar] [PubMed]
- 11. Patil N, Menon J, Nema S. Clinical and sonographic evaluation of percutaneous Achilles tendon tenotomy in idiopathic clubfoot: A prospective study. J Res Pract Musculoskelet Syst. 2023;7(4):125-140. doi:10.22540/JRPMS-07-125. [Google Scholar] [PubMed] [CrossRef]
- 12. Goyal A, Agarwal S, Gupta M, Kapoor R, Mittal M, Mishra AK. Evaluating the effectiveness of the ponseti technique in treating idiopathic clubfoot: Long-term outcomes from an Indian tertiary care centre. Cureus 2026;18:e100658. [Google Scholar] [PubMed]
- 13. Pirani S, Outerbridge HK, Moran M, Sawatzky B. A reliable method of clinically evaluating a virgin clubfoot evaluation. J Pediatr Orthop 2000;20:709-16. [Google Scholar] [PubMed]
- 14. Rehman NU, Saliq A, Mahmud W. Frequency and outcome of Achilles tenotomy in patients with clubfoot following Ponseti casting. J Clin Orthop Trauma 2021;19:231-7. [Google Scholar] [PubMed]
- 15. Saini R, Dhillon MS, Tripathy SK, Goyal T, Sudesh P, Gill SS, et al. Regeneration of the Achilles tendon after percutaneous tenotomy in infants: A clinical and MRI study. J Pediatr Orthop B 2010;19:344-7. [Google Scholar] [PubMed]
- 16. Lebel E, Karasik M, Bernstein-Weyel M, Mishukov Y, Peyser A. Achilles tenotomy as an office procedure: Safety and efficacy as part of the Ponseti serial casting protocol for clubfoot. J Pediatr Orthop 2012;32:412-5. [Google Scholar] [PubMed]
- 17. Sharma R, Kumar A, Sinha S, Jameel J, Khan R, Kumar S. Effectiveness of needle tenotomy for correction of equinus in clubfoot. Cureus 2022;14:e32080. [Google Scholar] [PubMed]
- 18. Barkham B, McNally T, Russell A, Bridgens A, Gelfer Y. Percutaneous Achilles tenotomy under local anaesthetic in the clubfoot clinic was safe during the COVID-19 pandemic, for both children and parents. Int Orthop 2021;45:2271-6. [Google Scholar] [PubMed]
- 19. Richetta S, Andreacchio A, Monforte S. Percutaneous Achilles tenotomy using a 18 gauge needle in the treatment of clubfoot with Ponseti method. Pediatr Med Chir. 2022;44(s1):295-297. doi: 10.4081/pmc.2022.295. [Google Scholar] [PubMed] [CrossRef]



Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Bilateral Clubfoot in Nail-Patella Syndrome: A Rare Syndromic Case Successfully Treated with the Ponseti Method
March 1, 2026 Bilateral Clubfoot in Nail-Patella Syndrome: A Rare Syndromic Case Successfully Treated with the Ponseti Method November 1, 2025 Easy Cast Removal in Idiopathic Congenital Talipes Equinovarus: A Study on Modified Ponseti Technique using an Interposed Polythene Sheet
November 1, 2025 Easy Cast Removal in Idiopathic Congenital Talipes Equinovarus: A Study on Modified Ponseti Technique using an Interposed Polythene Sheet July 1, 2025 An Observational Study on Pre-natal Diagnosis of Congenital Talipes Equinovarus
July 1, 2025 An Observational Study on Pre-natal Diagnosis of Congenital Talipes Equinovarus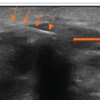 August 1, 2026 Thoracolumbar Fascial Defect in Persistent Low Back Pain After Lumbar Surgery: Ultrasound Findings and Response to Fascial Plane Injection
August 1, 2026 Thoracolumbar Fascial Defect in Persistent Low Back Pain After Lumbar Surgery: Ultrasound Findings and Response to Fascial Plane Injection