
Percutaneous radiofrequency ablation is a safe, day-care, minimally invasive option for appropriately selected benign bone tumors, providing rapid pain relief, early functional recovery, and high rates of radiological resolution with minimal morbidity.
Dr. Navdeep Singh Keer, Sports Injury Centre, VMMC and Safdarjung Hospital, New Delhi, India. E-mail: drnavdeepsinghkeer@gmail.com
Abstract
Introduction: Radiofrequency ablation (RFA) is a minimally invasive technique for the treatment of benign bone tumours, offering pain relief and lesion control with minimal morbidity. However, prospective Indian data on clinicoradiological outcomes remain sparse. This study aimed to evaluate pain reduction, functional recovery, and radiological healing following RFA in benign bone tumours.
Materials and Methods: This prospective study included 25 patients with symptomatic benign bone tumours who underwent percutaneous RFA under spinal anaesthesia between 2017 and 2020. RFA was performed under C-arm or computed tomography (CT) guidance. Pain was assessed using the visual analogue scale (VAS) and functional outcome through the Musculoskeletal Tumour Society (MSTS) score at baseline, 3 weeks, 6 weeks, and 6 months. Imaging follow-up with X-ray, CT, and magnetic resonance imaging (MRI) evaluated lesion size and marrow oedema. Statistical significance was set at P < 0.05.
Results: The mean pre-procedural VAS score was 7.44 ± 0.3, which reduced to 0.68 at 6 months (P < 0.05). MSTS scores improved from a baseline of 28.73–35 (maximum) by the 3rd week and remained stable thereafter. Radiologically, the mean lesion diameter decreased from 1.67 cm to 0.95 cm at 3 months (P = 0.005). Complete lesion resolution on CT was observed in 83.3% at 6 months and 95.8% at 9 months. MRI demonstrated resolution of marrow oedema in 96% of cases. Minor complications included two superficial burns and one recurrence requiring surgical curettage. There were no infections, fractures, or significant adverse events.
Conclusion: RFA is a safe and effective outpatient procedure for benign bone tumours, providing rapid and sustained pain relief, excellent functional outcomes, and high rates of radiological resolution. These results affirm RFA as a valuable alternative to surgical excision in appropriately selected cases. Larger studies are warranted to validate these findings and explore long-term outcomes.
Keywords: Radiofrequency ablation, bone neoplasms, treatment outcome, pain measurement, tomography, X-ray computed.
Benign bone tumours such as osteoid osteoma, osteoblastoma, and chondroblastoma cause disabling, often nocturnal pain out of proportion to their size. Traditional open curettage or en bloc resection removes the nidus but at the cost of surgical morbidity, iatrogenic fracture, long immobilisation and delayed return to work or sport [1]. Radiofrequency ablation (RFA) has reshaped this landscape: A percutaneous probe heats the nidus to >60°C, achieving cytotoxicity while sparing healthy cortex [2]. Success rates above 90% and durable pain relief are well documented in Western cohorts, yet most series focus on osteoid osteoma and rely on plain radiographs or computed tomography (CT) alone for follow-up [3,4,5,6]. The Indian experience is scant, and the link between cross-sectional imaging changes and functional recovery remains poorly defined. We therefore conducted a prospective study of CT- or C-arm-guided RFA for consecutive benign bone tumours at a high-volume tertiary centre in India. Pain (Visual Analogue Scale [VAS]) and function (Musculoskeletal Tumour Society [MSTS] score) were tracked alongside a tri-modal imaging protocol, radiographs, multidetector CT and magnetic resonance imaging (MRI) to capture nidus evolution and marrow oedema resolution. We hypothesised that RFA would provide rapid, sustained analgesia with minimal complications and that MRI findings would mirror functional gains. By pairing rigorous clinical metrics with detailed imaging across a broader tumour spectrum, this work fills a key gap in the orthopaedic oncology literature and offers data directly applicable to resource-constrained, high-load settings where minimally invasive solutions are paramount.
Study design and participants:
This prospective observational study was conducted between 2017 and 2020 at a tertiary care hospital in Delhi after Ethics Committee approval (S.No.: IEC/VMMC/SJH/Thesis/October/2017-153; dated October 30, 2017). Consecutive patients with symptomatic, histologically or radiologically confirmed benign bone tumours, osteoid osteoma, osteoblastoma or intraosseous chondroblastoma were screened. Inclusion criteria were (i) pain refractory to non-steroidal anti-inflammatory drugs for ≥3 months, (ii) lesion diameter ≤20 mm, and (iii) a safe percutaneous access corridor. Exclusion criteria comprised suspected malignancy, sub-articular location <5 mm from articular cartilage, pregnancy, coagulopathy, or active infection.
Sample size rationale:
Published series report a mean VAS reduction of roughly six points after RFA. Assuming the need to detect a clinically relevant two-point change with 80% power and α = 0.05, an a priori power calculation indicated 24 participants; allowing for minimal attrition, the recruitment target was set at 25. All enrolled patients completed the planned follow-up.
RFA technique and follow-up schedule:
Procedures were performed under spinal anaesthesia with conscious sedation. Using either multidetector CT or biplanar fluoroscopy, a 13-gauge coaxial bone cannula was advanced into the nidus (as illustrated in Fig. 1).
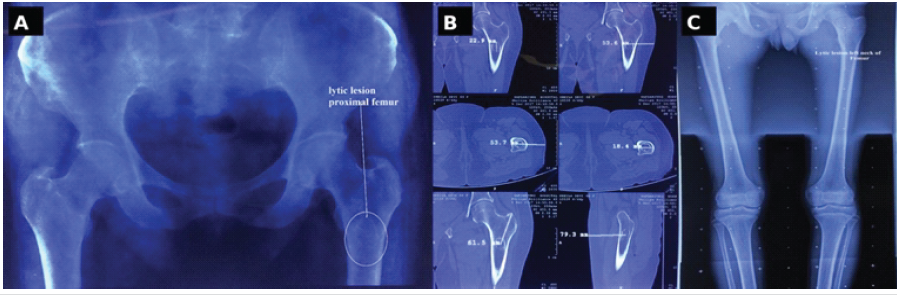
Figure 1: Multimodality assessment of proximal-femoral lesion. (a) Pelvic radiograph reveals a well-circumscribed lytic focus in the left proximal femur. (b) Axial and coronal computed tomography images with electronic callipers quantify nidus diameter and cortical thickness. (c) Long-leg scanogram confirms the solitary nature of the lesion and highlights skeletal alignment.
A 17-g internally cooled monopolar RFA electrode (7-mm active tip) delivered impedance-controlled energy, maintaining 90°C for 6 min. Track cauterisation was performed during electrode withdrawal, and patients were discharged the same day with a 48-h course of oral non-steroidal anti-inflammatory drugs. Clinical review and radiography were obtained at 3 weeks, 6 weeks, 3 months, 6 months and 9 months. Thin-slice CT and fat-suppressed MRI were performed at 3 and 6 months to document lesion evolution and marrow changes.
Outcome measures:
The primary outcome was pain relief, defined as ≥90% reduction in VAS score from baseline at 6 months. The secondary outcomes were functional recovery, defined as an MSTS score increase by ≥6 points; radiological success, defined as no enhancing nidus on CT and complete resolution of bone-marrow oedema on MRI; and procedure-related complications, classified as minor or major per the Society of Interventional Radiology criteria.
Statistical analysis:
Continuous variables are presented as mean ± standard deviation; categorical variables as counts and percentages. VAS and MSTS trajectories were compared with repeated-measures analysis of variance (ANOVA), and categorical data with χ2 or Fisher’s exact test. Two-sided P < 0.05 was considered statistically significant. Analyses were performed using Statistical Package for the Social Sciences (version 25).
Demographic characteristics:
The cohort comprised 25 patients (mean age 26 ± 7 years). Age-group distribution was 12% ≤12 years, 12% 12–18 years and 76% >18 years. Males predominated (15/25; 60%) over females (10/25; 40%). Lesions were most often in the femur (52%), followed by tibia (32%), fibula (8%), talus (4%) and calcaneum (4%) (Table 1).
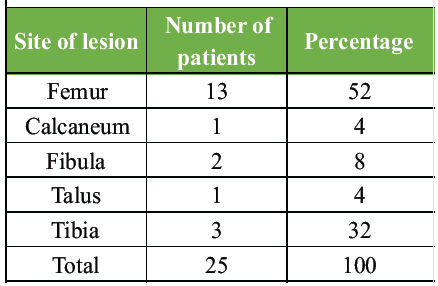
Table 1: Distribution of patients based on site of lesion
Intraoperative histology showed osteoid osteoma in 17 cases (68%), giant-cell tumour in 1 (4%), chondroblastoma in 1 (4%), fibrous dysplasia in 1 (4%), haemangioma in 1 (4%) and one inconclusive specimen (4%) (Table 2, Figs. 2 and 3).
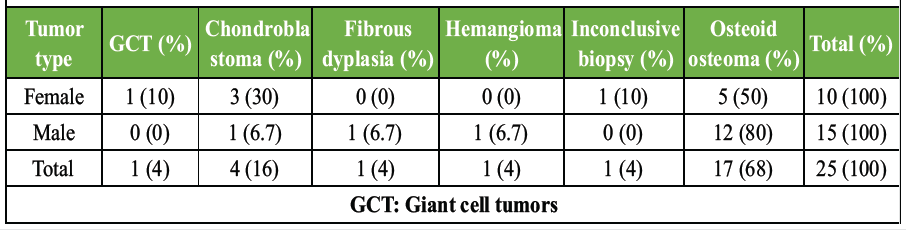
Table 2: Distribution of patients based on intra-operative biopsy findings
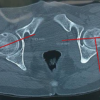
Figure 2: Image-guided radio-frequency ablation technique. (a) Fluoroscopic anteroposterior projection showing a coaxial bone cannula advanced into the nidus under real-time guidance. (b) Axial computed tomography (CT) slice depicting centrally placed 17-G internally cooled electrode with the ablation halo beginning to develop. (C) Three-dimensional CT reconstruction illustrates the final probe trajectory traversing the femoral neck into the nidus, ensuring an adequate safety margin.
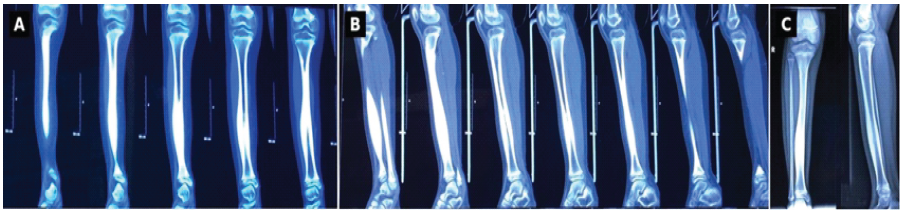
Figure 3: Composite pre-operative imaging of tibial nidus. (a) Coronal thin-slice computed tomography (CT) reformats demonstrate a cortical lucency with surrounding sclerosis in the mid-shaft tibia. (b) Sequential oblique-sagittal CT cuts outline the full craniocaudal extent of the nidus and adjacent reaction. (c) Orthogonal anteroposterior and lateral radiographs corroborate the cortical defect and sclerotic margin.
Pain and functional outcomes:
The baseline mean VAS pain score was 7.44. This fell to 6.76 at 3 weeks, 6.67 at 6 weeks and 0.68 by 6 months, a highly significant improvement (paired t-test P < 0.05). Mean MSTS functional score rose from 28.73 pre-procedure to the maximum 35 by week 3 and remained at 35 through week 6 (P < 0.05) (Table 3).
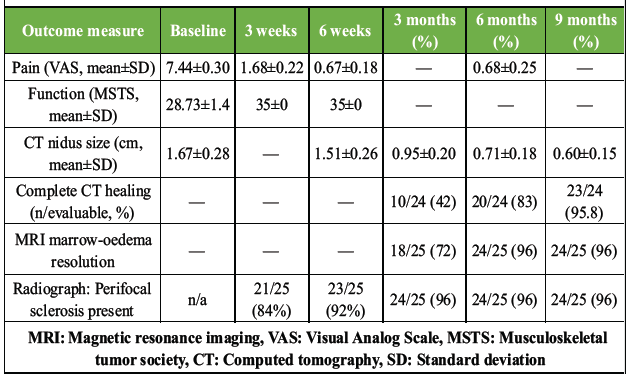
Table 3: Outcome measures
Tumour size and radiological healing:
On CT, the nidus diameter fell from 1.67 cm pre-RFA to 1.51 cm at 6 weeks and 0.95 cm at 3 months (repeated-measures ANOVA P = 0.005) (Fig. 4).
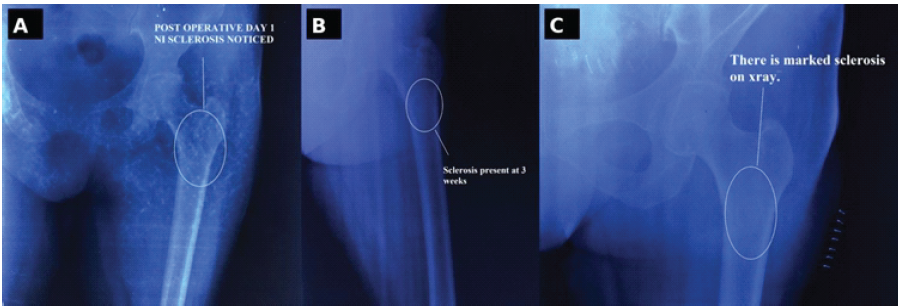
Figure 4: Serial radiographic evidence of post-ablation healing. (a) Day-1 postoperative radiograph shows early perifocal sclerosis around the ablated nidus. (b) At 3 weeks, the sclerotic rim has thickened and cortico-medullary continuity has begun to re-establish. (c) By 3 months, marked sclerosis and cortical remodelling denote mature bone healing with no residual lucency.
Complete CT disappearance of the lesion was documented in 20/24 evaluable patients (83.3%) at 6 months and 23/24 (95.8%) by 9 months. MRI demonstrated resolution of peri-lesional bone-marrow oedema in 24/25 cases (96%), with a single residual lesion managed subsequently. Serial radiographs showed progressive perifocal sclerosis at every visit (absent in 4% at ≥3 months) (Table 3). The best clinicoradiological response was observed in patients with osteoid osteoma, particularly those located in the femur and tibia, with marked pain relief, early functional recovery, and progressive radiological resolution following RFA. In contrast, the only case with persistent marrow oedema/recurrence was seen in a talar lesion, suggesting that small bones with relatively limited vascularity may show delayed or less predictable radiological recovery.
Complications:
Three minor adverse events were recorded (overall 12%): One pain recurrence (4%) was successfully treated with curettage, and two superficial thermal burns (8%) that healed with local care; no deep infections or fractures occurred.
The mean VAS score in our series fell from 7.44 pre-procedure to 0.68 at 6 months, mirroring the ≥90% pain-free rates reported by Rosenthal et al. (95%) and Rimondi et al. (92%) after percutaneous RFA of osteoid osteoma [7,8]. Our functional results were equally robust: MSTS scores reached the ceiling value of 35 by week 3 and remained stable, confirming that ablative control of the nidus translates rapidly into regained load-bearing and range of motion. Vanderschueren et al. documented a comparable 4–5-week return-to-sport window [9]. We attribute our brisk functional rebound to immediate post-ablative weight-bearing, rigorous physiotherapy and the relatively small cortical fenestration created by the 13-gauge cannula, which preserves structural integrity. Serial CT showed an 83.3% complete nidus disappearance at 6 months and 95.8% at 9 months, slightly faster than the 12-month median reported by Rimondi et al. [8]. Several factors may explain this: (i) Meticulous impedance-controlled delivery ensured a homogeneous 90°C isotherm; (ii) the use of a 7-mm active tip provided a wider ablation margin, reducing residual viable tissue; and (iii) a younger cohort (mean 26 years) may heal cortical defects more rapidly. MRI demonstrated marrow-ooedema resolution in 96% of cases, paralleling Gebauer et al., who showed that bone marrow ooedema vanishes within 6 months in >90% of successful ablations. The lone persistent oedema in our study occurred in a talar lesion, an area with poor vascularity and limited thermal dissipation, highlighting anatomical nuances that can delay radiological remission. Our overall complication rate was 12%, all minor (two superficial burns, one recurrence) and within the 6–15% envelope seen across large European registries [8,9]. We suspect the slight uptick stems from early adoption of the technique when thermal-protection sleeves were not yet routine; after their introduction, no further skin injury occurred. The solitary recurrence (4%) aligns with published 3–10% redo rates, emphasising the importance of exact probe centring, particularly in eccentrically calcified nidi, when working under fluoroscopy rather than CT [10,11,12,13,14]. By prospectively pairing tri-modal imaging with validated clinical metrics across a broader histologic spectrum, including osteoblastoma and chondroblastoma, our study extends the evidence base beyond osteoid osteoma, particularly for resource-constrained high-volume centres. The tight concordance between MRI oedema resolution and functional recovery supports a shorter, more cost-effective CT-plus-MRI follow-up algorithm at 3 and 6 months, reserving additional imaging for symptomatic cases.
Limitations:
The single-centre design and modest sample size limit generalisability; nevertheless, complete follow-up mitigates attrition bias. Future multicenter trials with longer surveillance should clarify durability beyond the first postoperative year and refine predictors of rare failures.
In this prospective Indian cohort, percutaneous radiofrequency ablation produced swift, durable pain relief, full functional recovery within 3 weeks, and near-complete radiological healing of benign bone tumours by 9 months, all with only minor, self-limited complications. By pairing VAS and MSTS scores with a tri-modal follow-up protocol (radiographs, CT, MRI) across a spectrum that extended beyond osteoid osteoma, our study not only corroborates Western data but also accelerates expected healing timelines. These findings validate RFA as a first-line, day-care option in resource-constrained, high-volume settings and demonstrate that MRI marrow-oedema resolution closely tracks clinical recovery, insights that can streamline cost-effective surveillance. Thus, the work fills a critical geographic and methodological gap, strengthening the global evidence base for minimally invasive management of benign bone tumours.
Percutaneous RFA should be considered a safe and effective minimally invasive treatment option for appropriately selected benign bone tumors, particularly osteoid osteoma, as it provides rapid pain relief, early functional recovery, minimal morbidity, and favorable radiological healing. Careful patient selection, accurate probe placement, and structured follow-up with clinical assessment and cross-sectional imaging are essential to optimize outcomes and identify rare cases of residual or recurrent disease.
References
- 1. Yang WT, Chen WM, Wang NH, Chen TH. Surgical treatment for osteoid osteoma-experience in both conventional open excision and CT-guided mini-incision surgery. J Chin Med Assoc 2007;70:545-50. [Google Scholar] [PubMed]
- 2. Barei DP, Moreau G, Scarborough MT, Neel MD. Percutaneous radiofrequency ablation of osteoid osteoma. Clin Orthop Relat Res 2000;373:115-24. [Google Scholar] [PubMed]
- 3. Rehnitz C, Sprengel SD, Lehner B, Ludwig K, Omlor G, Merle C, et al. CT-guided radiofrequency ablation of osteoid osteoma and osteoblastoma: Clinical success and long-term follow-up in 77 patients. Eur J Radiol 2012;81:3426-34. [Google Scholar] [PubMed]
- 4. Palussière J, Pellerin-Guignard A, Descat E, Cornélis F, Dixmérias F. Radiofrequency ablation of bone tumours. Diagn Interv Imaging 2012;93:680-4. [Google Scholar] [PubMed]
- 5. Chahal A, Rajalakshmi P, Khan SA, Rastogi S, Srivastava DN, Gamanagatti S. CT-guided percutaneous radiofrequency ablation of osteoid osteoma: Our experience in 87 patients. Indian J Radiol Imaging 2017;27:207-15. [Google Scholar] [PubMed]
- 6. Kulkarni SS, Shetty NS, Polnaya AM, Janu A, Kumar S, Puri A, et al. CT-guided radiofrequency ablation in osteoid osteoma: Result from a tertiary cancer centre in India. Indian J Radiol Imaging 2017;27:318-23. [Google Scholar] [PubMed]
- 7. Rosenthal DI, Hornicek FJ, Wolfe MW, Jennings LC, Gebhardt MC, Mankin HJ. Percutaneous radiofrequency coagulation of osteoid osteoma compared with operative treatment. J Bone Joint Surg Am 2003;85:773-80. [Google Scholar] [PubMed]
- 8. Rimondi E, Mavrogenis AF, Rossi G, Ciminari R, Malaguti C, Tranfaglia C, et al. Radiofrequency ablation for non-spinal osteoid osteomas in 557 patients. Eur Radiol 2012;22:181-8. [Google Scholar] [PubMed]
- 9. Vanderschueren G, Lateur G, Van Linthoudt D. Percutaneous radiofrequency ablation of osteoid osteoma: Long-term clinical outcome and factors influencing success. Skeletal Radiol 2012;41:593-99. [Google Scholar] [PubMed]
- 10. Gebauer B, Collettini F, Bruger C, Schaser KD, Melcher I, Tunn PU, et al. Radiofrequency ablation of osteoid osteomas: MRI follow-up of the inflammatory response after successful therapy. Acta Radiol 2013;54:569-74. [Google Scholar] [PubMed]
- 11. Bhakhar A, Sharma A, Kaganur R, Pragadeeshwaran J, Paul N, Kumar Dhukia R, et al. Outcomes of osteoid osteoma treated by percutaneous CT-guided radiofrequency ablation. Cureus 2023;15:e42675. [Google Scholar] [PubMed]
- 12. Vogl TJ, Bialek M, Eichler K, Hammerstingl R, Bielfeldt J, Zangos S, et al. Short- and long-term outcomes after radiofrequency ablation of osteoid osteomas. J Pers Med 2024;14:401. [Google Scholar] [PubMed]
- 13. Nagaraju N, Varma A, Taksande A, Reddy H, Javvaji CK, Suryadevara M, et al. Radiofrequency ablation (RFA) for osteoid osteoma in an 11-year-old male child with sickle cell trait: A case report. Cureus 2024;16:e63626. [Google Scholar] [PubMed]
- 14. Karluka I, Mazıcan M, Andic C, Bolgen C, Beyaz S, Turgut N, et al. Radiofrequency vs. Microwave ablation in osteoid osteoma: Comparative outcomes and prognostic factors. J Clin Med 2025;14:7814. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2025 Incidence and Functional Impact of Malrotation after Intramedullary Nailing of Femoral Shaft Fractures: A Prospective Computed Tomography-based Observational Study
November 1, 2025 Incidence and Functional Impact of Malrotation after Intramedullary Nailing of Femoral Shaft Fractures: A Prospective Computed Tomography-based Observational Study March 1, 2026 Assessment of Lumbar Foraminal Stenosis: Diagnostic Value and Clinical Correlation: A Systematic Review
March 1, 2026 Assessment of Lumbar Foraminal Stenosis: Diagnostic Value and Clinical Correlation: A Systematic Review June 1, 2026 Efficacy and Safety of Microwave Ablation for Osteoid Osteoma: A Retrospective Analysis of 35 Cases
June 1, 2026 Efficacy and Safety of Microwave Ablation for Osteoid Osteoma: A Retrospective Analysis of 35 Cases May 1, 2026 Reawakening of a Giant Cell Bone Tumor after 40 Years of Silence: A Rare Case Report
May 1, 2026 Reawakening of a Giant Cell Bone Tumor after 40 Years of Silence: A Rare Case Report