
All four fixation modalities yield satisfactory results, though modified tension band wiring (MTBW) shows superior functional outcomes and modified cerclage wiring (MCW) has the fewest complications.
Dr. Rajesh Kumar Gupta, Department of Orthopedics, Nandkumar Singh Chouhan Government Medical College, Khandwa, Madhya Pradesh, India. E-mail: guptarajk25@gmail.com
Abstract
Introduction: Comminuted patellar fractures constitute approximately 55% of all operatively managed patellar fractures and pose a persistent challenge for orthopedic surgeons. Comparative functional outcome data from India, particularly from central India, remain sparse.
Objectives: The objective of the study was to evaluate and compare the functional outcomes of tension band wiring (TBW), modified TBW (MTBW), cannulated screw TBW, and modified cerclage wiring (MCW) in the surgical management of comminuted patellar fractures.
Materials and Methods: This prospective observational study enrolled 63 cases of comminuted patellar fractures at Government Bundelkhand Medical College, Sagar, Madhya Pradesh, from August 2022 to April 2024. Of these, 46 underwent surgical management. Functional outcomes were assessed using the Böstman clinical grading score at 1, 3, 6, and 12 weeks post-operatively. Fisher’s exact test was applied for intergroup comparisons (significance threshold: P < 0.05).
Results: The mean patient age was 42.2 ± 15.4 years; 76.1% were male. Road traffic accidents were the predominant injury mechanism (69.6%). TBW was the most frequently performed procedure (43.5%). At 12 weeks, 39.1% achieved excellent and 47.9% achieved good Böstman scores. MTBW yielded the highest proportion of excellent results (56.3%). Complications occurred in 15.2% of cases, predominantly in the TBW group. No statistically significant differences were observed across modalities (P = 0.443).
Conclusion: All four modalities yielded satisfactory outcomes in comminuted patellar fractures. MTBW demonstrated numerically superior excellent outcomes; MCW showed the lowest complication rate. Fixation choice should be individualised to fracture morphology and surgeon expertise.
Keywords: Comminuted patellar fracture, tension band wiring, modified tension band wiring, modified cerclage wiring, Böstman score, and fixation modalities.
Patellar fractures constitute approximately 1% of all skeletal injuries and about 3.5% of lower extremity fractures, most often resulting from high-energy trauma [1]. When inadequately managed, they can cause extension lag, knee stiffness, patellofemoral arthritis, quadriceps weakness, and prolonged functional disability [1,2]. Among all patellar fractures treated surgically, approximately 55% are comminuted in nature [3]. The intra-articular position of these fractures makes precise anatomical reduction technically demanding, rendering them a persistent challenge for orthopaedic surgeons [4]. The primary goal of surgical intervention is to achieve accurate anatomical realignment of all fracture fragments, restore the integrity of the quadriceps extensor mechanism, and enable early postoperative mobilisation [5]. Failure to achieve satisfactory reduction is associated with delayed union or non-union, compromised knee function, extension lag, and post-traumatic patellofemoral osteoarthritis [4,6]. Extensive comminution also prolongs operative time, increasing exposure to anaesthesia and the risk of post-operative complications [7]. Numerous fixation techniques are available for comminuted patellar fractures, each with unique biomechanical properties and clinical implications. Conservative management is reserved for undisplaced fractures with an intact extensor mechanism [8]. Surgical options include tension band wiring (TBW), modified TBW (MTBW), cannulated screw TBW (CSTBW), cerclage wiring, modified cerclage wiring (MCW), basket plates, mesh plates, and nickel-titanium patellar concentrators [9,10]. Partial or total patellectomy should be reserved as a last resort, as it significantly disrupts the extensor mechanism and reduces quadriceps strength [11]. TBW and its modifications convert tensile quadriceps forces into compressive forces at the fracture site, promoting union [12]. MTBW has shown excellent results in transverse fractures, but its superiority in comminuted patterns remains debatable [13]. Conventional cerclage wiring offers inferior biomechanical stability compared to tension band constructs [14]. MCW, combining posterior circumferential cerclage (figure-of-0) with anterior tension band fixation (figure-of-8), has shown promising outcomes in recent studies [15]. Cannulated screw-based TBW reduces the risk of K-wire migration while maintaining the tension band mechanism [16]. The existing literature on comminuted patellar fracture management is predominantly from Western institutions, with limited data from India and none specifically from central India. This study aimed to prospectively evaluate and compare the functional outcomes and complication profiles of four commonly used fixation modalities for comminuted patellar fractures at a tertiary care government hospital in Madhya Pradesh.
Study design and setting:
This was a prospective observational study conducted in the Department of Orthopaedics, Government Bundelkhand Medical College and Hospital, Sagar, Madhya Pradesh, India, between August 2022 and April 2024.
Patient selection:
Inclusion criteria: Skeletally mature adults with comminuted patellar fractures where articular surface restoration was feasible; Grade 1 or 2 open wounds per the Gustilo-Anderson classification; and patients providing written and verbal informed consent. Exclusion criteria: Associated periarticular tibial or femoral condyle fractures; skeletally immature patients; old malunion or non-union of the patella; haematological disorders or muscular dystrophy; comminution precluding articular congruity restoration; fractures older than 2 weeks; irreparable extensor mechanism; and patients unwilling to consent.
Sample size:
A total of 68 cases of comminuted patellar fractures were treated during the study period. Five cases were excluded – two for associated tibial fractures, two for old patellar malunion, and one lost to follow-up – yielding a final cohort of 63 cases. Of these, 46 underwent surgical management, and 17 were managed conservatively. Non-probability convenience sampling was employed.
Surgical procedures:
All operative patients were treated under anaesthesia in the supine position through a longitudinal midline incision under tourniquet control. Fracture fragments were anatomically reduced and stabilised using reduction clamps. Articular congruity was confirmed by digital palpation through the retinacular defect and intraoperative fluoroscopy. Stability was verified by intraoperatively cycling the knee through full flexion-extension. Four surgical modalities were employed:
- TBW: Two parallel 2-mm K-wires drilled longitudinally through the patella, with an 18-gauge stainless steel wire passed in a figure-of-8 configuration over the anterior patellar surface, deep to the K-wire protrusions. K-wire ends were bent acutely and buried in soft tissue.
- MTBW: Similar K-wire placement with the addition of a supplementary SS wire loop passed through the superolateral border, medial fragment border, and back transversely, creating additional circumferential stabilisation with K-wire ends concealed deep within the bone.
- CSTBW: Two parallel 4-mm cannulated cancellous screws inserted over guide wires; 18-gauge SS wire threaded through the cannulated screws and crossed over the anterior patella in a figure-of-8 configuration, tightened with the knee in full extension.
- MCW: Double 18-gauge braided SS wire fixation in two planes: a circumferential wire at the periphery of the posterior articular surface (figure-of-0) and a second wire crossing the anterior patellar surface in a figure-of-8 tension band configuration.
All patients were encouraged to begin quadriceps exercises from post-operative day 1 and were permitted weight-bearing as tolerated from day 2. Knee flexion to 90° was targeted by 2 weeks postoperatively. A torn retinaculum was repaired in all cases.
Outcome assessment:
Patients were reviewed at 1, 3, 6, and 12 weeks postoperatively with clinical examination and radiographs. Functional outcomes were assessed using the Böstman clinical grading scale [17], which evaluates eight domains: range of motion (6 points), pain (6 points), working condition (4 points), quadriceps atrophy (4 points), assistive device use (4 points), joint effusion (2 points), giving way (2 points), and stair climbing (2 points); total score = 30 points. Scores of 28–30 were rated “excellent”, 20–27 as “good”, and <20 as “poor/unsatisfactory”.
Statistical analysis:
Data were entered in MS Excel and analysed using the Statistical Package for the Social Sciences version 26.0 (IBM Corp., Armonk, NY, USA). Proportions and percentages were calculated for categorical variables and mean ± standard deviation for continuous variables. Fisher’s exact test was applied for intergroup comparisons. A P < 0.05 was considered statistically significant.
Ethical considerations:
Ethical approval was obtained from the Institutional Ethics Committee of Government Bundelkhand Medical College, Sagar, Madhya Pradesh (No. IEC BMC/2022/86, dated 16/08/2022). Written and verbal informed consent was obtained from all participants. Participant confidentiality was maintained throughout the study.
Demographic and clinical characteristics:
A total of 63 participants were enrolled (46 surgical, 17 conservative). The mean age was 42.2 ± 15.4 years. Among surgical patients, 50.0% were in the 21–40-year age group and 41.3% in the 41–60-year group. Males constituted 76.1% of the surgical cohort. Farmers (30.4%), daily labourers (19.6%), and self-employed individuals (17.4%) were the predominant occupational groups. A history of substance use (predominantly tobacco) was present in 52.2% of patients, and comorbidities – primarily hypertension – were found in 23.9%. Right-sided fractures predominated (65.2%). Road traffic accidents (RTA) accounted for 69.6% of injuries, followed by falls (19.6%) and assault (10.9%). These characteristics are summarised in Table 1.
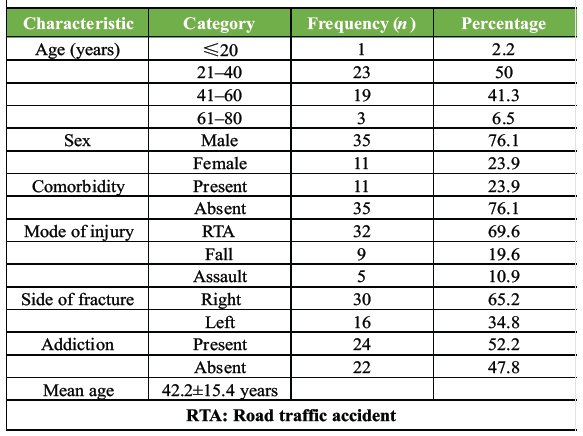
Table 1: Demographic and clinical profile of surgical patients (n = 46)
Management modalities:
Of the 63 total patients, 46 (73.0%) underwent surgical management and 17 (27.0%) were managed conservatively. Among surgical cases, TBW was the most frequently performed procedure (43.5%), followed by MTBW (34.8%), CSTBW (10.9%), and MCW (10.9%). One additional cerclage wiring case was excluded due to loss to follow-up. The average fracture-to-surgery interval was 4.3 ± 1.2 days; the majority were operated within 4 days. Distribution of surgical modalities is presented in Table 2.
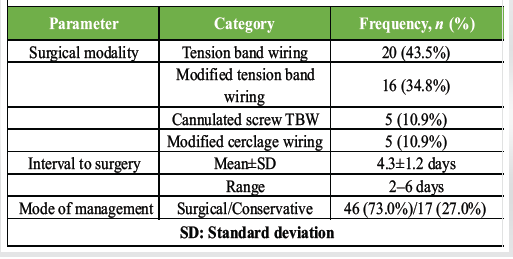
Table 2: Distribution of surgical modalities and management profile (n=46)
Functional outcomes by Böstman score:
At 1 week, 60.9% of patients had unsatisfactory outcomes across all groups (Figures 1 and 2); good outcomes were noted in 43.8% (MTBW), 40.0% (CSTBW), 40.0% (MCW), and 35.0% (TBW) patients, respectively (P = 0.962).
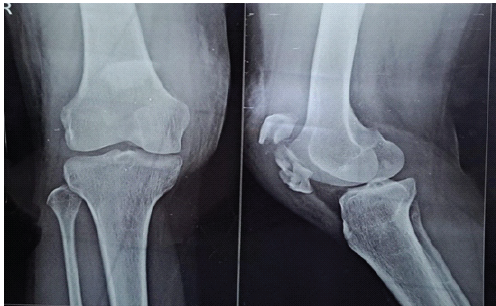
Figure 1: Pre-operative X-ray.
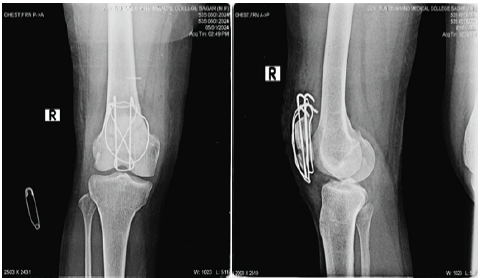
Figure 2: Immediate post-operative X-ray.
By week 3, 45.7% of all patients achieved good outcomes. MTBW demonstrated the highest good outcome rate (50%) at this stage (P = 0.968). At 6 weeks (Figure 3), 19.6% of patients achieved excellent outcomes and 43.5% achieved good outcomes.
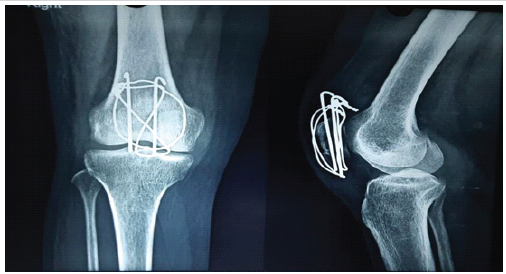
Figure 3: 6 week follow-up.
MTBW led in excellent outcomes (25%), followed equally by CSTBW and MCW (20% each) (P = 0.849). At the final 12-week follow-up (Figure 4), 39.1% achieved excellent and 47.9% achieved good outcomes; only 13.0% remained unsatisfactory.
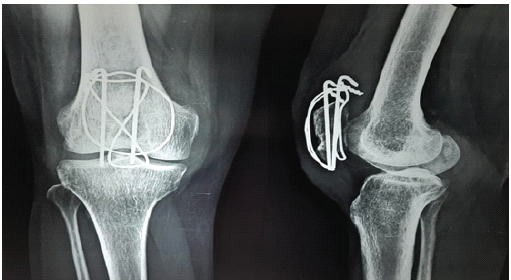
Figure 4: 12-week follow-up.
MTBW demonstrated the highest rate of excellent outcomes (56.3%), followed by MCW (40%) and CSTBW (40%); TBW achieved 25% excellent outcomes (P = 0.443). All intergroup differences were not statistically significant. Complete outcome data across all time points are presented in Table 3.
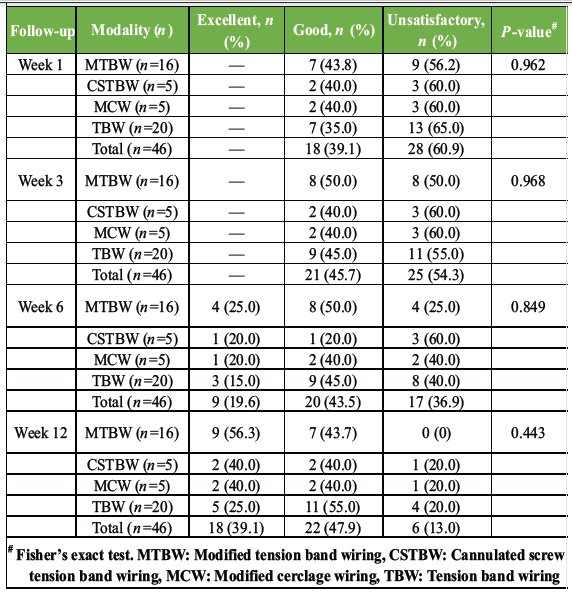
Table 3: Functional outcomes by Böstman score at serial follow-up across fixation modalities (n=46)
Complications:
Complications were observed in 7 of 46 surgical patients (15.2%). Five complications (71.4% of total) arose in the TBW group: Two cases of surgical site infection, two cases of K-wire migration, and one combined case of infection and wire migration. One infection each was recorded in the MTBW and CSTBW groups. No complications were observed in the MCW group. Complication data are presented in Table 4.
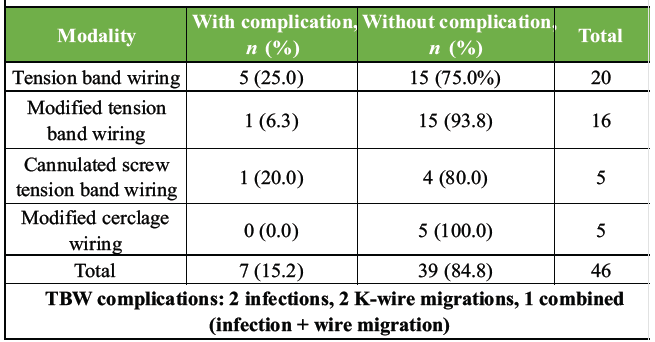
Table 4: Post-operative complications by fixation modality (n = 46)
This prospective study evaluated functional outcomes following four fixation modalities for comminuted patellar fractures at a tertiary care government hospital in central India. At the 12-week follow-up, 87% of surgically managed patients achieved either excellent (39.1%) or good (47.9%) outcomes per the Böstman scoring system, indicating that all four modalities yield satisfactory results when appropriately applied.
Demographic profile and injury characteristics:
The predominant age group was 21–40 years (50.0%), with a mean age of 42.2 years, consistent with the peak incidence of patellar fractures reported in the third to fifth decades [18]. Males constituted 76.1% of the surgical cohort. This male predominance is well-documented: Soomro et al. reported 71.4% male prevalence in comminuted patellar fracture cohorts, while Shrestha et al. reported 87.5% [19]. The higher incidence in males reflects greater participation in high-risk outdoor occupational activities – farming (30.4%) and daily labour (19.6%) were the two largest occupational groups – and greater exposure to motorised traffic in this region. RTAs accounted for 69.6% of injuries, consistent with Shrestha et al., who reported RTAs in 80% of comminuted patellar fractures [19]. The high proportion of RTA-related injuries reflects the increasing volume of motorcycle traffic in central India. Falls from height were the second most common mechanism (19.6%), consistent with the findings of Jun et al. and Turgut et al. [20,21]. High-energy mechanisms such as RTA are associated with comminuted fracture patterns due to the magnitude of transmitted force and soft tissue disruption.
Outcomes of fixation modalities:
At 12 weeks, MTBW demonstrated the highest rate of excellent outcomes (56.3%), followed by MCW (40%) and CSTBW (40%). The superior results with MTBW are attributable to its biomechanical design, which converts quadriceps tensile forces into compressive forces at the fracture interface while providing additional circumferential stabilisation through supplementary wire loops [13]. Cho et al. reported a mean Böstman score of 28.6 points with miniplate-augmented TBW in comminuted fractures, supporting the advantage of augmented tension band constructs [22]. The MCW group, though small (n = 5), showed no complications and achieved 40% excellent outcomes at 12 weeks. The modified cerclage technique addresses the primary limitation of conventional cerclage – inadequate biomechanical stability – by integrating a posterior circumferential cerclage with an anterior tension band [15]. Sun et al. reported a mean Böstman score of 28.7 using MCW, with 84.2% achieving excellent results at a mean follow-up of 16 months [15]. Sun et al. similarly reported a mean Böstman score of 28.13 ± 1.73 with zero non-union or implant failure [23]. CSTBW achieved 40% excellent and 40% good outcomes. Cannulated screws provide greater compressive force at the fracture site, eliminate K-wire migration risk, and maintain the tension band mechanism [16]. Hoshino et al. demonstrated lower complication rates with CSTBW compared to K-wire-based TBW in transverse fractures, and our data suggest a similar trend in comminuted patterns [24]. Despite these numerical differences, no intergroup comparison reached statistical significance (P = 0.443–0.968), likely due to small subgroup sizes and limited follow-up duration.
Complications:
Overall complications were observed in 15.2% of patients; the TBW group contributed 71.4% of all complications, including K-wire migration and infection. K-wire migration is a well-recognised complication of TBW, with hardware removal rates reported as high as 36.8% in some series [24]. Bending K-wire ends acutely and burying them deep in soft tissue reduces this risk but does not eliminate it. The absence of complications in the MCW group supports growing evidence for modified cerclage as a safe and reliable fixation alternative [15,23].
Strengths and limitations:
This study has several strengths, including its prospective observational design, inclusion of multiple commonly used fixation modalities, standardised post-operative rehabilitation protocol, and use of a validated functional assessment tool in a real-world tertiary government hospital setting from an under-represented geographic region of central India. Nevertheless, several limitations must be acknowledged. First, the overall surgical sample size was relatively small (n = 46), which limited the statistical power of intergroup comparisons. The CSTBW and MCW subgroups were particularly small (n = 5 each), thereby reducing the reliability and interpretability of subgroup analyses. Second, the study employed a non-randomised observational design in which fixation modality selection was determined by fracture morphology, implant availability, and surgeon preference. This may have introduced selection bias and confounding. Third, as this was a single-centre study conducted at a tertiary government institution, the findings may not be fully generalisable to private-sector hospitals or other healthcare settings with different patient demographics, surgical expertise, or implant resources. In addition, non-probability convenience sampling was used, increasing the possibility of sampling bias. The follow-up duration was limited to 12 weeks, which was sufficient for early functional evaluation but inadequate for assessment of long-term outcomes such as post-traumatic patellofemoral arthritis, implant failure, symptomatic hardware irritation, functional endurance, reoperation rates, or delayed complications. Serial radiological progression of fracture union was not quantitatively assessed using standardised union criteria, limiting objective evaluation of healing dynamics. Advanced imaging, such as computed tomography (CT), was not routinely utilised for fracture classification or comminution assessment. Consequently, detailed fracture morphology and severity stratification could not be standardised across groups, which may have influenced both fixation selection and postoperative outcomes. Furthermore, surgeon-related performance bias cannot be excluded, as different levels of familiarity and technical expertise with individual fixation methods may have affected operative execution and clinical results. Outcome assessors were not blinded to treatment allocation, thereby introducing potential assessment bias. Functional evaluation relied exclusively on the Böstman clinical grading scale, without incorporation of additional validated patient-reported outcome measures such as the Lysholm Knee Score, Kujala Anterior Knee Pain Scale, or Knee Injury and Osteoarthritis Outcome Score. Moreover, the observed numerical superiority of MTBW was not supported by biomechanical testing or laboratory correlation. Although post-operative complications such as infection and K-wire migration were documented, several clinically relevant complications – including anterior knee pain, implant prominence, secondary hardware removal, extensor lag quantification, and patient satisfaction – were not comprehensively analysed. Economic evaluation and cost-effectiveness analysis were also beyond the scope of the present study, despite their importance in resource-constrained healthcare environments where implant affordability influences surgical decision-making. Finally, although 17 patients underwent conservative management during the study period, their outcomes were not included in the comparative analysis with surgically managed cohorts. Inclusion of conservative treatment outcomes could have provided additional insight into treatment-selection thresholds and indications for operative intervention. Future multicenter randomised controlled studies with larger cohorts, CT-based fracture stratification, longer follow-up, blinded assessment, and comprehensive functional and radiological evaluation are warranted to establish stronger evidence regarding optimal fixation strategies for comminuted patellar fractures.
All four fixation modalities – TBW, MTBW, CSTBW, and MCW – produced satisfactory functional outcomes in comminuted patellar fractures at 12 weeks as measured by the Böstman scoring system. MTBW demonstrated numerically superior excellent outcomes (56.3%), while MCW showed the lowest complication rate. The TBW group was associated with the highest complication burden, primarily K-wire migration and infection. The selection of fixation modality should be individualised to fracture pattern, fragment morphology, degree of comminution, and surgeon proficiency. Larger randomised studies with extended follow-up are warranted to confirm these findings and guide evidence-based surgical decision-making in comminuted patellar fracture management.
Surgical management of comminuted patellar fractures using TBW, MTBW, CSTBW, or MCW generally yields satisfactory functional outcomes, with approximately 87% of patients achieving good to excellent Böstman scores. MTBW appears to offer the highest rate of excellent functional recovery, likely due to its superior biomechanical stabilization of fragmented bone. In contrast, MCW presents as a safer alternative with the lowest complication profile, specifically avoiding the K-wire migration frequently observed with traditional TBW. Ultimately, the selection of a fixation modality should be tailored to the specific fracture morphology and the surgeon’s technical proficiency to ensure optimal reduction and minimize hardware-related issues.
References
- 1. Luo TD, Marino DV, Pilson H. Patella fractures. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/nbk513330 [Last accessed on 25 Jan 2026]. [Google Scholar] [PubMed]
- 2. Carpenter JE, Kasman R, Matthews LS. Fractures of the patella. J Bone Joint Surg Am 1993;75:1550-61. [Google Scholar] [PubMed]
- 3. Gwinner C, Märdian S, Schwabe P, Schaser KD, Krapohl BD, Jung TM. Current concepts review: Fractures of the patella. GMS Interdiscip Plast Reconstr Surg DGPW 2016;5:Doc01. [Google Scholar] [PubMed]
- 4. Sharafatvaziri A, Shayan-Moghadam R, Tahmaseb MN, Tahami M, Vosoughi F. Comminuted patellar fracture: A summary of the latest updates. J Orthop Spine Trauma 2020;5(4):99-102. http://dx.doi.org/10.18502/jost.v5i4.4379 [Google Scholar] [PubMed] [CrossRef]
- 5. Bui CN, Learned JR, Scolaro JA. Treatment of patellar fractures and injuries to the extensor mechanism of the knee: A critical analysis review. JBJS Rev 2018;6:e1. [Google Scholar] [PubMed]
- 6. Benjamin J, Bried J, Dohm M, McMurtry M. Biomechanical evaluation of various forms of fixation of transverse patellar fractures. J Orthop Trauma 1987;1:219-22. [Google Scholar] [PubMed]
- 7. Hoshino CM, Tran W, Tiberi JV, Black MH, Li BH, Gold SM, et al. Complications following tension-band fixation of patellar fractures with cannulated screws compared with Kirschner wires. J Bone Joint Surg Am 2013;95:653-9. [Google Scholar] [PubMed]
- 8. Sayum Filho J, Lenza M, Teixeira De Carvalho R, Pires OG, Cohen M, Belloti JC. Interventions for treating fractures of the patella in adults. Cochrane Database Syst Rev 2015;2:CD009651. [Google Scholar] [PubMed]
- 9. Hambright DS, Walley KC, Hall A, Appleton PT, Rodriguez EK. Revisiting tension band fixation for difficult patellar fractures. J Orthop Trauma 2017;31:e66-72. [Google Scholar] [PubMed]
- 10. Steinmetz S, Brügger A, Chauveau J, Chevalley F, Borens O, Thein E. Practical guidelines for the treatment of patellar fractures in adults. Swiss Med Wkly 2020;150:w20165. [Google Scholar] [PubMed]
- 11. Kaufer H. Mechanical function of the patella. J Bone Joint Surg Am 1971;53:1551-60. [Google Scholar] [PubMed]
- 12. Cho JW, Kent WT, Cho WT, Kim JK, Moon KH, Yeo DH, et al. Miniplate augmented tension-band wiring for comminuted patella fractures. J Orthop Trauma 2019;33:e143-50. [Google Scholar] [PubMed]
- 13. Hsu KL, Chang WL, Yang CY, Yeh ML, Chang CW. Factors affecting the outcomes of modified tension band wiring techniques in transverse patellar fractures. Injury 2017;48:2800-6. [Google Scholar] [PubMed]
- 14. Smith ST, Cramer KE, Karges DE, Watson JT, Moed BR. Early complications in the operative treatment of patella fractures. J Orthop Trauma 1997;11:183-7. [Google Scholar] [PubMed]
- 15. Sun Y, Sheng K, Li Q, Wang D, Zhou D. Management of comminuted patellar fracture fixation using modified cerclage wiring. J Orthop Surg Res 2019;14:324. [Google Scholar] [PubMed]
- 16. Khan I, Dar MY, Rashid S, Butt MF. Internal fixation of transverse patella fractures using cannulated cancellous screws with anterior tension band wiring. MOJ Orthop Rheumatol 2016;10:21-6. [Google Scholar] [PubMed]
- 17. Böstman O, Kiviluoto O, Santavirta S, Nirhamo J, Wilppula E. Fractures of the patella treated by operation. Arch Orthop Trauma Surg 1983;102:78-81. [Google Scholar] [PubMed]
- 18. Cramer KE, Moed BR. Patellar fractures: Contemporary approach to treatment. J Am Acad Orthop Surg 1997;5:323-31. [Google Scholar] [PubMed]
- 19. Shrestha B, Kandel PR, Shrestha KM, Shrestha S, Pandey S, Chhetri P. Surgical management of clavicle fracture with precontoured locking plate. J Univ Coll Med Sci. 2024;12(2):6-9. doi:10.3126/jucms.v12i02.69371. [Google Scholar] [PubMed] [CrossRef]
- 20. Jun J, Lee JH, Han J, Kim SH, Kim S, Cho GC, et al. Characteristics of fall-from-height patients: a retrospective comparison of jumpers and fallers using a multi-institutional registry. Clin Exp Emerg Med. 2024 Mar;11(1):79-87. doi: 10.15441/ceem.23.074. [Google Scholar] [PubMed] [CrossRef]
- 21. Turgut K, Sarihan ME, Colak C, Güven T, Gür A, Gürbüz S. Falls from height: A retrospective analysis. World J Emerg Med. 2018;9(1):46-50. doi: 10.5847/wjem.j.1920-8642.2018.01.007. [Google Scholar] [PubMed] [CrossRef]
- 22. Cho JW, Kent WT, Cho WT, Kim JK, Moon KH, Yeo DH, Kim BS, Oh CW, Oh JK. Miniplate Augmented Tension-Band Wiring for Comminuted Patella Fractures. J Orthop Trauma. 2019 Apr;33(4):e143-e150. doi: 10.1097/BOT.0000000000001390. [Google Scholar] [PubMed] [CrossRef]
- 23. Sun Y, Sheng K, Li Q, Wang D, Zhou D. Management of comminuted patellar fracture fixation using modified cerclage wiring. J Orthop Surg Res. 2019 Oct 17;14(1):324. doi: 10.1186/s13018-019-1385-5. [Google Scholar] [PubMed] [CrossRef]
- 24. Hoshino CM, Tran W, Tiberi JV, Black MH, Li BH, Gold SM, Navarro RA. Complications following tension-band fixation of patellar fractures with cannulated screws compared with Kirschner wires. J Bone Joint Surg Am. 2013 Apr 3;95(7):653-9. doi: 10.2106/JBJS.K.01549. [Google Scholar] [PubMed] [CrossRef]



Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 A Rare Case of Combined Tibial Plateau Fracture with Tibial Tuberosity Avulsion Injury: Case Report
March 1, 2026 A Rare Case of Combined Tibial Plateau Fracture with Tibial Tuberosity Avulsion Injury: Case Report August 1, 2025 Complex Scapulothoracic Disruption Managed with Scapular Dual Column Plating and Acromion Tension Band Osteosynthesis: A Radiological and Functional Success Story
August 1, 2025 Complex Scapulothoracic Disruption Managed with Scapular Dual Column Plating and Acromion Tension Band Osteosynthesis: A Radiological and Functional Success Story October 1, 2024 Comparative Study of Inferior Pole of Patella Fracture Treated with Transosseous Technique using Modified Krackow’s Technique Versus Traditional Anterior Tension Band Wiring
October 1, 2024 Comparative Study of Inferior Pole of Patella Fracture Treated with Transosseous Technique using Modified Krackow’s Technique Versus Traditional Anterior Tension Band Wiring April 10, 2024 Tension Band Wiring in Gap Non-union Patella – A Simple Technique with Profound Results: Case Report
April 10, 2024 Tension Band Wiring in Gap Non-union Patella – A Simple Technique with Profound Results: Case Report