
Rare mechanical dissociation at the helical blade-barrel interface can occur early after PFN fixation even without classical cut-out or infection.
Dr. Mantu Jain, Department of Orthopaedics, All India Institute of Medical Sciences, Bhubaneswar - 751019, Odisha, India. E-mail: montu_jn@yahoo.com
Abstract
Introduction: Proximal femoral nail (PFN) fixation is widely used for intertrochanteric (IT) fractures; however, implant-related complications remain a concern. While commonly reported failures include cut-out, back-out, and implant breakage, dissociation at the helical blade-barrel interface is extremely rare and poorly described in the literature. To the best of our knowledge, no prior case reports have described this specific mode of failure
Case Report: A 62-year-old male presented with pain in the left hip region following prior PFN fixation for an IT femur fracture. On evaluation, implant failure in the form of PFN nail breakage was identified. The patient underwent revision with a long PFN and lateral support plate. On post-operative day 21, he developed pain and implant prominence. Radiographs did not demonstrate classical blade back-out or cut-out but showed mechanical disengagement at the blade-barrel interface. Three-dimensional computed tomography confirmed dissociation of the barrel from the helical blade, with the blade remaining in situ within the femoral head. There was no evidence of infection. Revision surgery confirmed mechanical failure at the blade-barrel interface. The blade was replaced, and debridement was performed. Microbiological cultures were sterile. The patient had an uneventful recovery.
Conclusion: This case highlights a rare and early mechanical failure of PFN involving blade-barrel dissociation. Awareness of this failure mode and early radiological evaluation are essential to prevent complications and guide timely intervention.
Keywords: Intertrochanteric fracture, proximal femoral nail, implant failure, helical blade, mechanical dissociation.
Intertrochanteric (IT) femur fractures are common in the elderly population and are frequently managed using intramedullary fixation devices such as the proximal femoral nail (PFN) [1]. The introduction of the helical blade design has improved rotational stability and bone purchase, particularly in osteoporotic bone [2]. Despite these advantages, complications related to PFN fixation continue to be reported. Common modes of failure include helical blade cut-out, back-out, non-union, and implant breakage [3]. These are often attributed to poor reduction quality, improper implant positioning, and compromised bone quality. However, mechanical failure at the level of implant assembly, particularly involving the blade-barrel interface, is rarely described. We report a unique case of early mechanical dissociation of the helical blade from the barrel component of a PFN, occurring within 3 weeks of revision surgery, without evidence of infection or classical migration. This case highlights an uncommon but important failure mechanism that has implications for surgical technique and implant design.
A 62-year-old male presented with complaints of pain in the left hip region. He had previously sustained a left-sided IT femur fracture (AO/OTA type 31-A2), for which he underwent fixation with a short PFN at an outside institution. The patient had a history of bilateral total knee replacement performed 8 months prior and comorbidities, including type 2 diabetes mellitus and hypertension, both medically managed. At presentation, clinical and radiographic evaluation revealed implant failure in the form of PFN nail breakage (Fig. 1a and b), which was considered the probable time point of failure. The patient subsequently underwent revision surgery at our centre with the removal of the broken implant and fixation using a long PFN construct with a helical blade, augmented with an additional lateral support plate (Fig. 1c and d).
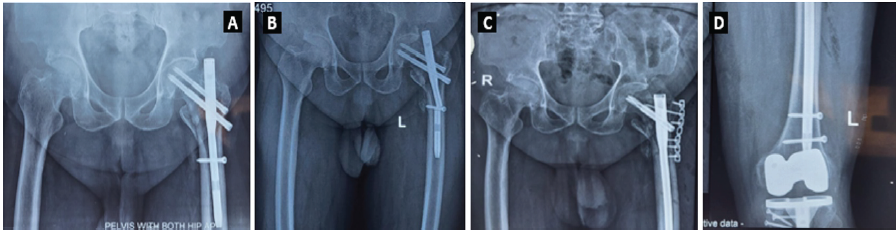
Figure 1: Proximal femoral nail done for intertrochanteric fracture (a); broken nail (b); revised with proximal femoral nail anti-rotation Asia 2 with helical blade and supported by lateral plate (c); distal locking showing prior total knee replacement (d).
Postoperatively, he was mobilised with partial weight-bearing using a walker. During the post-operative period, the patient developed progressively increasing pain over the left hip along with prominence of the proximal implant. At approximately 3 weeks postoperatively, radiographic evaluation demonstrated mechanical disengagement of the barrel component from the helical blade within the PFN assembly (Fig. 2a), suggestive of failure at the blade-barrel interface rather than classical cut-out or migration. Clinically, there was exposure of the barrel through the previous surgical incision, associated with serosanguinous discharge, without systemic signs of infection. To further delineate the implant failure and assess the fracture-implant relationship, a three-dimensional computed tomography scan was performed. The imaging confirmed dissociation of the barrel from the helical blade, with the blade remaining in situ within the femoral head and no evidence of intra-articular penetration or significant osteolysis (Fig. 2b). The patient subsequently underwent revision surgery. Intraoperatively, the dissociated components were removed (Fig. 2c), and a new helical blade was inserted with restoration of the locking mechanism under fluoroscopic guidance. Post-operative radiographs confirmed satisfactory implant positioning (Fig. 2d).

Figure 2: Disengagement of the helical blade from its barrel seen on X-ray (a); Computed tomography scan (b); removed helical blade and barrel (c); revised blade with plate construct with antibiotic stimulants (d).
Thorough wound debridement and excision of the sinus tract were performed, and local antibiotic delivery was achieved using calcium sulphate. There was no evidence of purulence or deep infection intraoperatively, and bone quality was considered suboptimal without significant osteolysis. Microbiological cultures obtained intraoperatively were sterile, and histopathological examination did not reveal any evidence of active infection, supporting a mechanical aetiology of failure. The post-operative course was uneventful, with satisfactory implant positioning confirmed on radiographs. The patient was advised strict non-weight-bearing for 6 weeks along with supervised physiotherapy. At the 3-month follow-up, the patient demonstrated complete clinical recovery with satisfactory functional outcome (Fig. 3)

Figure 3: Implants in place and union in progress.
PFN fixation is widely accepted as the treatment of choice for unstable IT fractures due to its biomechanical advantages, including a shorter lever arm, load-sharing properties, and improved rotational stability [2,3]. The introduction of the helical blade design has further enhanced fixation in osteoporotic bone by compaction of cancellous bone and increased resistance to rotation [3]. Despite these advantages, implant-related complications continue to be reported. The most commonly described modes of failure include helical blade cut-out, back-out, varus collapse, non-union, and implant breakage [4,5]. Studies have emphasised that these failures are multifactorial, involving both surgical technique and patient-related factors [2,4,5]. Poor reduction quality and loss of medial femoral cortical support have been identified as major predictors of implant failure, significantly increasing the risk of mechanical complications [6]. Similarly, an increased tip-apex distance and malposition of the blade have been strongly associated with fixation failure [7,8]. Biomechanically, failure of PFN constructs is typically attributed to excessive bending and torsional forces acting on the implant, particularly in the setting of inadequate fracture stability or poor bone quality [9]. Osteoporosis further compromises fixation by reducing bone purchase and increasing the likelihood of cut-out or implant migration, as highlighted in previous case reports [10,11]. In contrast to these well-described mechanisms, the present case demonstrates a rare and distinct mode of failure involving dissociation at the helical blade-barrel interface. Unlike classical cut-out or back-out, the helical blade in this case remained in situ within the femoral head, while the barrel component disengaged from the nail assembly. This indicates a failure of the internal locking mechanism rather than failure at the bone-implant interface. Very few studies have reported complications related to the locking mechanism of the helical blade. Siu et al. described intraoperative failures of blade locking, emphasising the importance of confirming proper engagement during insertion [12]. In addition, rare implant-related complications such as helical blade perforation into the joint have been reported, further highlighting the spectrum of atypical failure modes [13]. However, a comprehensive review of the available literature did not reveal any documented cases of post-operative dissociation of the blade-barrel interface as seen in our patient. To the best of our knowledge, this represents a previously unreported and unique mode of implant failure in PFN systems. The early onset of failure in our case, occurring within 3 weeks of revision surgery, suggests a primary mechanical issue rather than fatigue-related failure. Possible mechanisms include incomplete locking of the blade during insertion, manufacturing defects, or micro-motion at the interface leading to progressive loosening under cyclic loading conditions. Importantly, infection was ruled out in this case by sterile microbiological cultures and absence of intraoperative purulence, further supporting a purely mechanical aetiology. From a clinical perspective, this case underscores several important considerations. First, surgeons must ensure meticulous intraoperative verification of the locking mechanism of the helical blade. Second, early post-operative pain or implant prominence should prompt careful radiological evaluation, as atypical failure modes may be missed on routine assessment. Finally, awareness of such rare complications is essential for timely intervention and prevention of further morbidity.
This case highlights a rare and early mechanical failure of PFN fixation involving dissociation at the helical blade-barrel interface. Recognition of this uncommon failure mode is important for early diagnosis and timely revision. It also underscores the need for careful implant assembly and intraoperative verification of locking mechanisms to prevent such complications.
Not all proximal femoral nail failures present as cut-out or migration – early implant prominence may indicate rare blade-barrel dissociation, requiring prompt recognition and revision.
References
- 1. </p> [Google Scholar] [PubMed]
- 2. <ol> [Google Scholar] [PubMed]
- 3. <li>Kürüm H, Tosun HB, Aydemir F, Ayas O, Orhan K, Key S. Intertrochanteric femoral fractures: A comparative analysis of clinical and radiographic outcomes between talon intramedullary nail and intertan nail. Cureus 2023;15(12):e50877.</li> [Google Scholar] [PubMed]
- 4. <li>Boles EU, Kulper S, Whiffin K, Oentaryo MJ, Schneider K, Leung F, <em>et al</em>. Comparison of the dynamic cut-out failure modes of common proximal femoral fixation devices using a mesh-free computational method. J Orthop Res 2026;44(2):e70159.</li> [Google Scholar] [PubMed]
- 5. <li>Lee H, Lee SH, Lim W, Jo S, Jo S. Comparison of helical blade systems for osteoporotic intertrochanteric fractures using biomechanical analysis and clinical assessments. Medicina (Kaunas) 2022;58(12):1699.</li> [Google Scholar] [PubMed]
- 6. <li>Kumar N, Vatsya P, Salaria AK. Indigenous proximal femoral nails and their novel complications. Cureus 13(7): e16729..</li> [Google Scholar] [PubMed]
- 7. <li>Papanikolopoulos D, Kalligeros C, Polyzos A, Spitas V, Soranoglou V. Proximal femoral nail mechanical failure: A case report and biomechanical study. Cureus 2022;14(3):e23694.</li> [Google Scholar] [PubMed]
- 8. <li>Li Z, Gao J, Wu X, Chang Z, Liu X, Zhang L, <em>et al</em>. Risk factors for implant failure of PFNA-II in the treatment of intertrochanteric fractures (AO/OTA 31 A1 and A2). BMC Musculoskelet Disord 2025;26(1):784.</li> [Google Scholar] [PubMed]
- 9. <li>Baumgaertner MR, Curtin SL, Lindskog DM, Keggi JM. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am 1995;77(7):1058-64.</li> [Google Scholar] [PubMed]
- 10. <li>Turgut A, Kalenderer Ö, Karapınar L, Kumbaracı M, Akkan HA, Ağuş H. Which factor is most important for occurrence of cutout complications in patients treated with proximal femoral nail antirotation? Retrospective analysis of 298 patients. Arch Orthop Trauma Surg. 2016;136(5):623–30..</li> [Google Scholar] [PubMed]
- 11. <li>Sommers MB, Roth C, Hall H. Biomechanics of fixation failure. J Orthop Trauma 2004;18:361-8.</li> [Google Scholar] [PubMed]
- 12. <li>Kale A, Salunkhe R, Pervez FR, Shevate I, Sharma P. Treatment of Failed Proximal Femoral Nail Anti-rotation Asia (PFNA2) in a Severely Osteoporotic Patient With a Revision Stem. Cureus 2024;16(2):e55152.</li> [Google Scholar] [PubMed]
- 13. <li>Phalak M O, Chaudhari T, Chaudhari A K (August 01, 2024) Bipolar Hemiarthroplasty With a Calcar Stem for the Management of a Failed Proximal Femoral Nail Anti-rotation Asia (PFNA2) in a Case of Geriatric Unstable Intertrochanteric Femur Fracture. Cureus 16(8): e65980.</li> [Google Scholar] [PubMed]
- 14. <li>Siu YC, Ling SK, Ma CM, Lui TH. Intraoperative failures of the PFNa II spiral blade. Trauma Emerg Care 20161(2): 23-27.</li> [Google Scholar] [PubMed]
- 15. <li>Brunner A, Jöckel JA, Babst R. The PFNA proximal femur nail in treatment of unstable proximal femur fractures–3 cases of postoperative perforation of the helical blade into the hip joint. J Orthop Trauma 2008;22(10):731-6.</li> [Google Scholar] [PubMed]
- 16. </ol> [Google Scholar] [PubMed]
- 17. <p> [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Radiological Outcomes of Reamed Short Proximal Femoral Nailing in Intertrochanteric Fractures in Patients Aged 50 Years and Above
August 1, 2026 Radiological Outcomes of Reamed Short Proximal Femoral Nailing in Intertrochanteric Fractures in Patients Aged 50 Years and Above August 1, 2026 Evaluation of Orthopedic Outcomes of Proximal Femoral Nailing for Intertrochanteric Fractures and Predictive Value of Pre-operative Glycemic Status, Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio: A Prospective Study
August 1, 2026 Evaluation of Orthopedic Outcomes of Proximal Femoral Nailing for Intertrochanteric Fractures and Predictive Value of Pre-operative Glycemic Status, Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio: A Prospective Study June 1, 2026 Pseudoaneurysm of the Medial Femoral Circumflex Artery following Surgical Fixation of Trochanteric Femur Fracture: A Case Report
June 1, 2026 Pseudoaneurysm of the Medial Femoral Circumflex Artery following Surgical Fixation of Trochanteric Femur Fracture: A Case Report November 1, 2025 Impact of Tip Apex Distance, Cortical Reduction, and Lateral Wall Integrity on Radiological Union of Unstable Trochanter Fracture Treated with Proximal Femoral Nail: A Retrospective Observational Study
November 1, 2025 Impact of Tip Apex Distance, Cortical Reduction, and Lateral Wall Integrity on Radiological Union of Unstable Trochanter Fracture Treated with Proximal Femoral Nail: A Retrospective Observational Study