
Isolated extensor indicis proprius rupture may be clinically subtle and missed on MRI; in selected patients with intact extensor digitorum communis function, excision of a symptomatic scar stump without reconstruction may be definitive treatment.
Dr. Nicholas C Semenza, Division of Hand and Upper Extremity Surgery, Department of Orthopaedic Surgery, Allegheny Health Network, 320 East North Ave, Pittsburgh, Pennsylvania – 15212, United States. E-mail: nicholas.semenza@ahn.org
Abstract
Introduction: Isolated traumatic rupture of the extensor indicis proprius (EIP) is uncommon and may be masked by preserved index finger extension through the intact extensor digitorum communis (EDC). While primary repair or tendon transfer is standard when reconstruction is feasible, the functional redundancy of the dual-extensor index finger raises the question of whether excision alone can suffice in selected cases. We report what we believe to be the first documented case of intentional EIP stump excision without reconstruction as definitive surgical treatment following delayed-presentation traumatic EIP rupture.
Case Report: A 45-year-old diabetic male metalworker (glycated haemoglobin 7.7%) sustained a dorsal wrist laceration from sheet metal. The patient self-managed initially but subsequently presented to the emergency department 2 weeks later. He was ultimately referred to our hand clinic 2 months post-injury with persistent dorsal hand pain, a palpable scar mass, and near-intact index finger extension. Magnetic resonance imaging (MRI) demonstrated tenosynovitis without reported rupture; our independent review identified sequential EIP disappearance on axial slices consistent with rupture. A diagnostic-therapeutic corticosteroid injection provided only a transient benefit. Surgical exploration revealed a fibrotic, retracted EIP stump with intact EDC tendons. The stump was excised without reconstruction. At 2-week follow-up, the patient reported no pain, demonstrated a full composite fist, intact distal sensation, and preserved index finger extension with a well-healing incision.
Conclusion: EIP rupture may be underdiagnosed due to compensatory EDC extension and can be missed on MRI in the chronic fibrotic setting. In patients with preserved EDC function, significant comorbidities, and a non-viable chronic stump, excision without reconstruction eliminates a painful scar mass, reduces ongoing tenosynovitis, and avoids the morbidity of tendon transfer. Early functional results in this case are encouraging.
Keywords: Extensor indicis proprius, tendon rupture, dorsal hand laceration, tendon excision, index finger extension, case report.
The extensor indicis proprius (EIP) is the deep extensor of the forearm that provides independent extension of the index finger via the fourth dorsal compartment. Due to the index finger’s redundant extensor, the extensor digitorum communis (EDC), an isolated EIP rupture may present with preserved or near-normal active extension, facilitating missed or delayed diagnosis. The published literature on EIP injury is dominated by its use as a donor tendon for extensor pollicis longus (EPL) reconstruction [1,2], while reports of isolated traumatic EIP rupture and its management are sparse. In acute settings, primary repair is standard. In chronic or delayed presentations with tendon retraction and fibrosis, reconstruction via tendon grafting or transfer is generally advocated. However, given that intentional EIP harvest for transfer does not impair index finger extension when the EDC is intact [3,4], the need for reconstruction following traumatic EIP rupture with intact EDC function is not self-evident. We present a case of symptomatic, delayed-presentation EIP rupture in a diabetic patient managed by excision of the fibrotic stump alone and review the literature supporting this approach.
History and examination:
A 45-year-old right-hand-dominant male with type 2 diabetes mellitus (glycated haemoglobin [HbA1c] 7.7%) employed as a metalworker sustained a dorsal wrist laceration from sheet metal in October 2025. He self-managed the wound at home. Two weeks later, he presented to an emergency department with worsening dorsal wrist and forearm pain and swelling; oral antibiotics were prescribed, and no tendon injury was identified. Two months post-injury, he was referred to our hand surgery clinic, reporting persistent dorsal hand pain radiating into the index finger. He had undergone hand occupational therapy with minimal improvement. Examination revealed dorsal hand swelling, a palpable firm mass consistent with fibrotic scar tissue, and near-intact index metacarpophalangeal (MCP) extension with subtle weakness relative to the contralateral side; there was no frank extension lag.
Imaging and diagnostic injection:
Magnetic resonance imaging (MRI) of the wrist and hand (T2-weighted axial series) demonstrated tenosynovitis of the EDC, extensor carpi radialis, and extensor carpi ulnaris; no tendon rupture was reported, and the EIP was not addressed. On our review, sequential axial slices showed the EIP as a discrete structure ulnar to the EDC index in proximal slices. This structure disappeared across consecutive distal slices on the MRI, demonstrating a pattern consistent with EIP rupture and retraction rather than tendon continuity (Fig. 1).
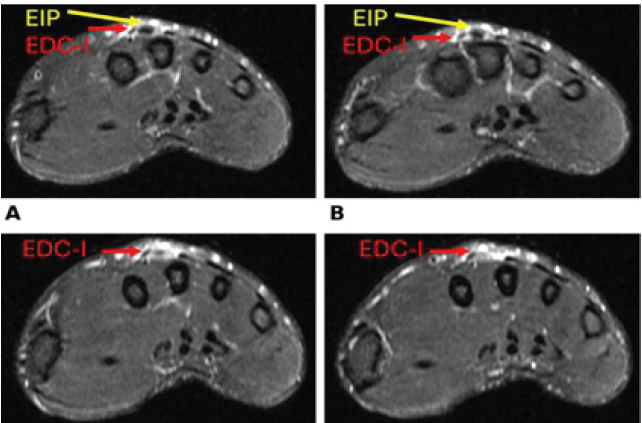
Figure 1: Sequential T2-weighted axial magnetic resonance imaging images of the hand demonstrating EIP rupture. (a and b) The EIP tendon (yellow arrow) is identifiable as a discrete low-signal structure lying ulnar to the EDC-index tendon within the fourth dorsal compartment. The EDC-index tendon is identified radial to the EIP tendon. (c and d) In consecutive distal slices, the EIP signal is absent, consistent with tendon rupture and proximal retraction. Surrounding EDC, ECR, and ECU tendons demonstrate tenosynovitis without rupture. EIP: Extensor indicis proprius, EDC: Extensor digitorum communis, ECR: Extensor carpi radialis, ECU: Extensor carpi ulnaris.
Two weeks later, a diagnostic-therapeutic injection of 1 mL betamethasone mixed with 1 mL ropivacaine into the fourth extensor compartment provided transient but unsustained relief, supporting a structural rather than purely inflammatory aetiology.
Operative findings and technique:
Under local anaesthesia (10 mL 1% lidocaine with epinephrine) and monitored anaesthesia care, a 4-cm longitudinal dorsal incision was made using a No. 15 blade. Tenotomy scissors were used for subcutaneous dissection into the fourth extensor compartment. The EDC tendons to the index and long fingers were identified and confirmed intact. The EIP was identified as a fibrotic scar ball representing the retracted proximal stump (Figs. 2 and 3).

Figure 2: Intraoperative photograph showing the fourth dorsal compartment exposed. The scarred, fibrotic extensor indicis proprius tendon stump (center) is visible adjacent to intact extensor digitorum communis tendons. Surgical marking lines are visible on the skin.

Figure 3: Intraoperative photograph following mobilization of the extensor indicis proprius scar stump, demonstrating its fibrotic, avascular character and relationship to intact adjacent structures.
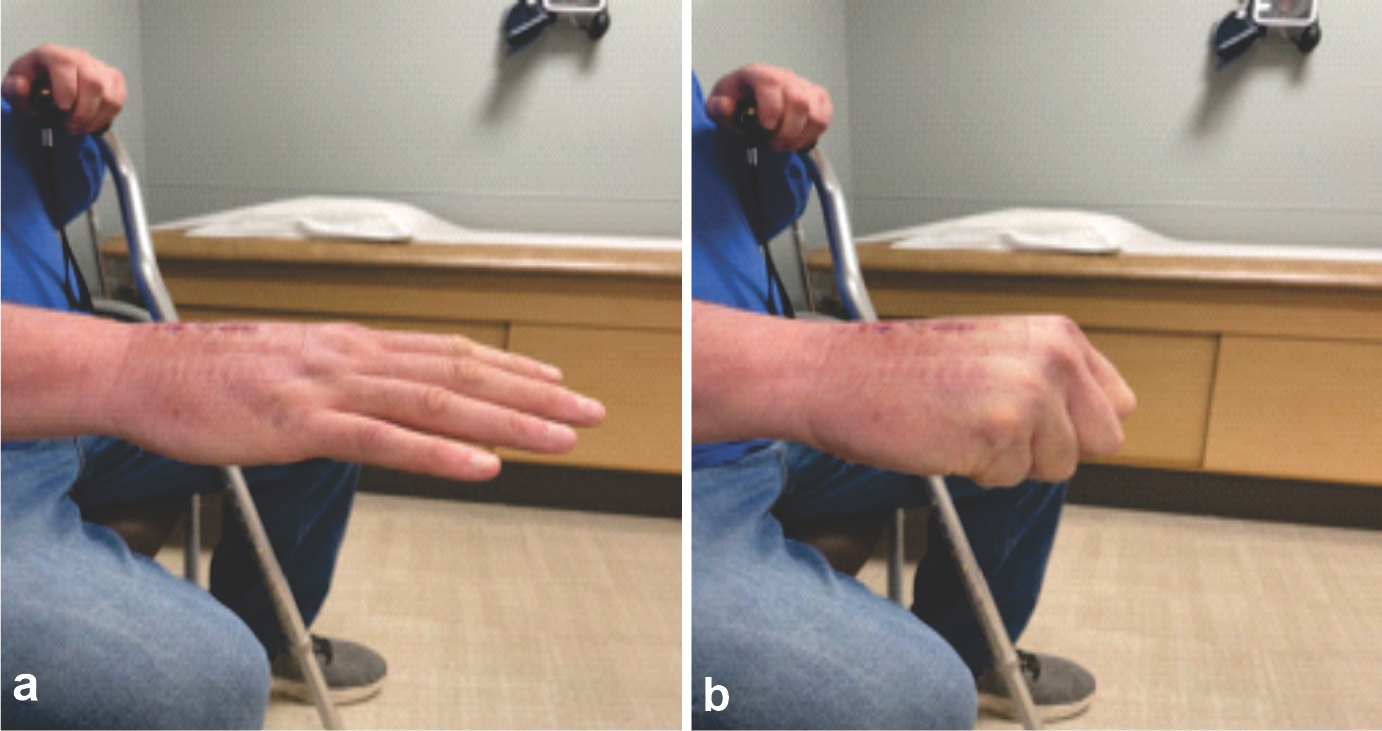
Figure 4:Two-week post-operative clinical photographs. (a) Dorsal view demonstrating a well-healing incision with no swelling or erythema and full index finger extension. (b) The patient demonstrates a full composite fist, confirming preserved flexor function and no extensor tethering.
Under ×3.5 loupe magnification, the scar was dissected free, and the tendon stump was debrided, pulled distally, and excised proximally. Residual scar tissue was removed. The wound was irrigated, the retinaculum was repaired, and the wound was closed with 3-0 Vicryl (deep) and 4-0 running Monocryl (skin).
Post-operative course:
The patient tolerated the procedure without complication and was placed in a soft, sterile dressing. At his 2-week post-operative visit, he reported complete resolution of pain. Examination demonstrated a well-healing incision, preserved distal sensation, intact index finger extension, and a full composite fist (Fig. 4a and b). He was advised to continue hand therapy and will be followed as needed.
EIP anatomy and functional redundancy:
The EIP arises from the distal dorsal ulna and interosseous membrane, courses through the fourth dorsal compartment, and inserts ulnar to the EDC-I into the extensor hood [5]. It is ulnar to the EDC-I in approximately 92% of anatomical specimens [6] and, unlike EDC tendons, lacks juncturae tendinum [7]. This anatomy underlies two clinically important principles: (1) Isolated EIP rupture need not produce a frank extension lag, as the EDC-I independently extends the index MCP; and (2) the absence of junctural tethering means a ruptured EIP stump retracts freely, forming the fibrotic mass encountered in our patient.
Delayed diagnosis and MRI limitations:
EIP rupture is susceptible to delayed diagnosis because preserved index extension via the EDC masks functional deficit. MRI, though generally considered the reference standard for soft-tissue hand pathology [8], has documented limitations for chronic extensor injuries. One study reported MRI sensitivity of only 44% for missed extensor tendon injuries versus 84% for ultrasound, attributing this to fibrotic scar tissue mimicking residual tendon signal [9]. In our case, the radiologist identified surrounding tenosynovitis but did not comment on the EIP – likely because the scarred stump blended with the fibrotic background [10]. Active sequential review of each compartment tendon on axial slices, looking for tendon disappearance, is necessary to avoid this pitfall.
Diabetes mellitus and tendon biology:
Type 2 diabetes adversely affects tendon physiology through the accumulation of advanced glycation end products, which alter collagen crosslinking, reduce viscoelasticity, and impair tenocyte function [11,12]. Our patient’s HbA1c of 7.7% reflects moderate glycaemic control at the time of surgery. Diabetic patients carry an approximately threefold elevated risk of tendon rupture and exhibit impaired post-injury healing characterised by hypertrophic scarring [13]. These changes explain the fibrotic, avascular stump encountered intraoperatively and informed our decision against reconstruction: performing a tendon transfer in a compromised tissue environment with a 2-month delay and extensive fibrosis carried a substantial risk of healing failure and adhesion. The intact EDC provided functional compensation, making excision alone the more favourable option.
Rationale for excision without reconstruction:
EIP harvest for tendon transfer – most commonly for EPL reconstruction – consistently preserves near-normal independent index extension through the intact EDC [3,4,14]. If intentional EIP removal does not impair function, traumatic EIP loss should logically produce the same result. Excision of the symptomatic stump aimed to (1) remove a painful mechanical mass, (2) eliminate the inflammatory stimulus of a non-viable tendon stump within the synovial compartment, and (3) decompress the fourth extensor compartment. Our patient’s outcome – pain-free, full composite fist, intact extension – supports this reasoning. We are unaware of prior reports specifically documenting EIP stump excision as definitive treatment for traumatic rupture; our case adds to the indirect evidence from EIP harvest series [3,4] and anomalous EIP excision reports [15-20].
Patient selection:
Based on this case and literature review, EIP excision without reconstruction appears most appropriate when: (1) The EDC is intact with preserved or near-normal MCP extension; (2) the EIP stump is chronic and non-viable; (3) significant comorbidities (e.g., diabetes, immunosuppression) increase reconstruction risk; and (4) the patient understands the potential for mild residual extension weakness. Acute EIP lacerations, younger patients without comorbidities, or concurrent EDC injury should prompt consideration of primary repair or reconstruction.
We report a case of delayed, post-traumatic EIP rupture in a diabetic patient managed by surgical excision of the fibrotic stump without reconstruction, with excellent early functional results. The case highlights that EIP rupture may be clinically and radiologically occult and that the functional redundancy of the dual-extensor index finger provides an anatomical rationale for excision alone when the EDC is intact. This approach warrants consideration in carefully selected patients and adds to the surgical decision-making framework for EIP injuries.
When MRI does not explicitly identify EIP rupture but clinical findings – palpable scar mass, index pain, and penetrating dorsal trauma – suggest it, the surgeon should actively review axial sequences for sequential tendon disappearance. In diabetic patients with a chronic, non-viable EIP stump and intact EDC, excision without reconstruction is a legitimate surgical alternative that may offer equivalent functional recovery with reduced morbidity compared to tendon transfer.
References
- 1. Magnussen PA, Harvey FJ, Tonkin MA. Extensor indicis proprius transfer for rupture of the extensor pollicis longus tendon. J Bone Joint Surg Br 1990;72:881-3. [Google Scholar] [PubMed]
- 2. Sperati G, Ceri L. Transposition of the extensor indicis proprius (EIP) for inveterate post-traumatic rupture of the extensor pollicis longus (EPL) of the hand. 12 Clinical cases. Acta Biomed 2019;90:147-51. [Google Scholar] [PubMed]
- 3. Ha C, Hong IT, Oh CH, Ryu H, Chung J, Han SH. Clinical outcomes of extensor indicis proprius tendon transfer for extensor pollicis longus tendon rupture. Hand Surg Rehabil 2024;49(10):1243-1249. [Google Scholar] [PubMed]
- 4. Kitano K, Tado K, Shibata T, Yoshida T. Independent index extension after indicis proprius transfer: Excision of juncturae tendinum. J Hand Surg Am 1996;21:992-6. [Google Scholar] [PubMed]
- 5. Rockwell WB, Butler PN, Byrne BA. Extensor tendon: Anatomy, injury, and reconstruction. Plast Reconstr Surg 2000;106:1592-603; quiz 1604, 1673. [Google Scholar] [PubMed]
- 6. Srinivasan S, Dearman B. Anatomy of the extensor tendons to the index finger. J Hand Surg Am 1996;21:923-7. [Google Scholar] [PubMed]
- 7. Von Schroeder HP, Botte MJ. The functional significance of the long extensors and juncturae tendinum in finger extension. J Hand Surg Am 1993;18:641-7. [Google Scholar] [PubMed]
- 8. Klauser AS. MRI of the extensor tendons of the wrist. AJR Am J Roentgenol 2018;211:W107-16. [Google Scholar] [PubMed]
- 9. Ozcanli H, Senel E, Ergunes M. The diagnostic value of ultrasonography and magnetic resonance imaging in missed hand tendon injuries. Hand Surg Rehabil 2023;42:215-22. [Google Scholar] [PubMed]
- 10. Chung CB, Steinbach LS. MR imaging of the extensor mechanism of the fingers: MR imaging-anatomic correlation. Radiographics 2003;23:1471-88. [Google Scholar] [PubMed]
- 11. Xu J, Wang J, Ji Y, Liu Y, Jiang J, Wang Y, et al. The impact of diabetes mellitus on tendon pathology: A review. Front Pharmacol. 2024;15:1491633. [Google Scholar] [PubMed]
- 12. Zellers JA, Vaidya R, Lake SP. Effect of diabetes on tendon structure and function: Not limited to collagen crosslinking. J Diabetes Sci Technol 2023;17:89-98. [Google Scholar] [PubMed]
- 13. Bedi A, Fox AJ, Harris PE, Deng XH, Ying L, Warren RF, et al. Diabetes mellitus impairs tendon-bone healing after rotator cuff repair. J Shoulder Elbow Surg 2010;19:978-88. [Google Scholar] [PubMed]
- 14. Anderson GA, Lee V, Sundararaj GD. Extensor indicis proprius opponensplasty. J Hand Surg Br 1991;16:334-8. [Google Scholar] [PubMed]
- 15. Kwon SY, Kim TJ. Anomalous extensor indicis proprius muscle causing dorsal compartment syndrome. J Korean Orthop Assoc 2013;48:68-71. [Google Scholar] [PubMed]
- 16. Seki A, Fujita S. Extensor indicis proprius and extensor digitorum communis rupture after volar locked plating of the distal radius: A case report. J Orthop Sci 2013;18:350-4. [Google Scholar] [PubMed]
- 17. Pham DT, Nguyen TS. Delayed rupture of extensor indicis proprius and extensor pollicis longus following volar plating of distal radius fracture: A case report. Clin Case Rep 2025;20:3171-8. [Google Scholar] [PubMed]
- 18. Zhou J, Frey C, Segovia N, Yao J. Anatomic relationship of extensor indicis propius and extensor digitorum communis: Implications for tendon transfer. World J Orthop 2022; 13(11): 978-985. [Google Scholar] [PubMed]
- 19. David MA. The effects of type II diabetes mellitus on tendon homeostasis and healing. J Orthop Res 2019;37:1191-200. [Google Scholar] [PubMed]
- 20. Doyle JR. Extensor tendons-acute injuries. In: Green DP, Hotchkiss RN, Pederson WC, editors. Green’s Operative Hand Surgery. 4th ed. New York: Churchill Livingstone; 1999. p. 1950-87. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Posterior Acetabular Wall Fracture Mimicking a Subcapital Femoral Neck Fracture on Plain Radiographs: A Diagnostic Pitfall and the Role of Intraoperative Fluoroscopy: A Case Report
August 1, 2026 Posterior Acetabular Wall Fracture Mimicking a Subcapital Femoral Neck Fracture on Plain Radiographs: A Diagnostic Pitfall and the Role of Intraoperative Fluoroscopy: A Case Report August 1, 2026 To Explore or Not? Conservatively Managed Brachial Artery Injury with Good Collateral Flow After Elbow Reduction: A Case Report
August 1, 2026 To Explore or Not? Conservatively Managed Brachial Artery Injury with Good Collateral Flow After Elbow Reduction: A Case Report August 1, 2026 An Unusual Catastrophic Neurological Complication Following a Routine Arthroscopic Multiligament Knee Reconstruction: A Case Report
August 1, 2026 An Unusual Catastrophic Neurological Complication Following a Routine Arthroscopic Multiligament Knee Reconstruction: A Case Report August 1, 2026 Post-operative C5 Palsy Following Posterior Cervical Decompression and Fusion: A Case Report
August 1, 2026 Post-operative C5 Palsy Following Posterior Cervical Decompression and Fusion: A Case Report