
Non-vascularized iliac crest autograft is a reliable, single-stage solution for restoring anatomy and function in selected hand and wrist bone defects.
Dr. Joana Páscoa Pinheiro, Department of Orthopedics and Trauma, Centro Hospitalar e Universitário Lisboa Norte, Hospital de Santa Maria, Lisbon, Portugal. E-mail: joanapascoapinheiro@gmail.com
Abstract
Introduction: Bone defects of the hand and wrist may result from trauma or tumour resection and represent a reconstructive challenge due to the complex anatomy and functional demands of this region. Autologous bone grafting is commonly used to restore bone stock and preserve hand and wrist function.
Case Report: Two patients with distal radius and carpal bone defects were treated using a non-vascularised iliac crest autograft. Patient 1 sustained a high-energy motorcycle accident resulting in an open distal radius fracture with significant metaphyseal bone loss, managed with definitive osteosynthesis and iliac crest autografting. Patient 2 presented with a locally aggressive midcarpal bone tumour; following wide resection, the defect was reconstructed through carpal arthrodesis using the same autograft. At the final follow-up, both patients were pain-free and able to perform full activities of daily living.
Conclusion: In selected cases, non-vascularised iliac crest autograft allows effective reconstruction of hand and wrist bone defects, providing stable bone healing, pain relief, and satisfactory functional outcomes.
Keywords: Iliac crest autograft, hand and wrist reconstruction, bone defects, distal radius fracture.
Hand and wrist bony defects can occur after trauma or be secondary to a specific disease, either by a tumour, infection, or idiopathic avascular necrosis. The complex anatomy of the hand and wrist represents a challenge for the orthopaedic surgeon as to restoring the size and shape of the defect and re-establishing the normal kinematics of the joints [1].
Autologous bone grafts have been used for several years to replace hand and wrist bony defects. Choosing the right graft to restore the anatomy in the distal upper limb depends on several factors. Bone characteristics, including shape, size, and structural properties; past surgeries; or trauma around the defect can influence the local conditions and affect the graft choice. In addition, we should provide minimal donor site morbidity [2,3].
An iliac bone crest graft in hand surgery reconstruction was first described by Wilson and Lance in 1965 [4]. It was defined as a safe option with a low rate of clinical complications, having adequate biomechanical properties and fibrocartilage ability [5]. We present immediate bone autografting in two patients with secondary hand and wrist bone defects in different clinical scenarios, where iliac crest autograft was used to reconstruct the anatomy. Functional outcomes were recorded, including the Visual Analogue Scale (VAS) score at rest to measure pain intensity, the Disabilities of the Arm, Shoulder, and Hand (QuickDASH) score, and the Patient-Rated Wrist Evaluation (PRWE) score. Subsequently, a brief literature review will be conducted based on the two clinical cases.
We present a 37-year-old male patient (Patient 1) with a right distal radius open fracture (Gustilo and Anderson grade IIIA) [6] after a high-energy motorcycle accident. Radiographs showed a complex distal radius fracture with a significant meta-epiphyseal bone loss (Fig. 1a and b).
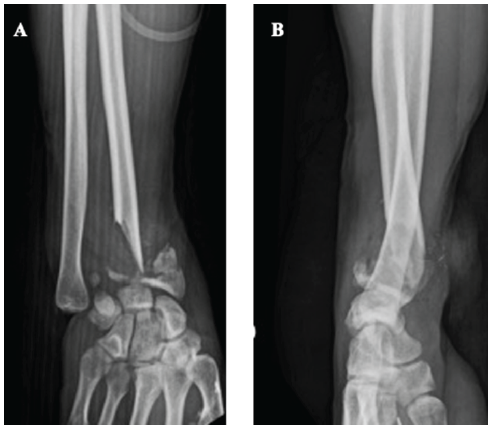
Figure 1: X-rays of the right distal radius open fracture with a significant loss of the meta-epiphyseal bone in anterior-posterior (a) and lateral (b) views. The defect measured was approximately 36.7 × 23.6 mm.
The defect was measured as 36.7 × 23.6 mm. Despite an unaffected radial styloid, part of the scaphoid facet was affected, together with a major defect at the lunate facet. Primary surgery consisted of stabilisation with an external fixator (Fig. 2a and b), and 8 days after the accident, the patient underwent definitive osteosynthesis with an iliac crest bone graft to fill the meta-epiphyseal defect (Fig. 3a and b). At 2-year follow-up, bony fusion was achieved, with the patient presenting a slight depression within the lunate facet area (Fig. 3c and d).
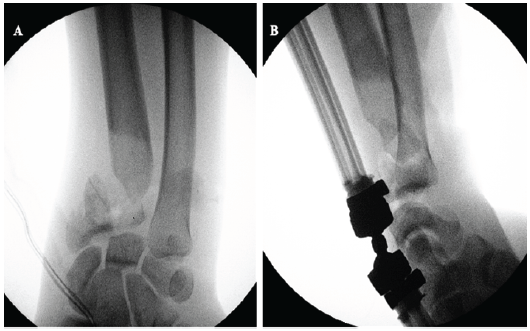
Figure 2: Intra-operative X-rays of the distal radius fracture primary stabilization using an external fixator. Anterior-posterior (a) and lateral (b) views.
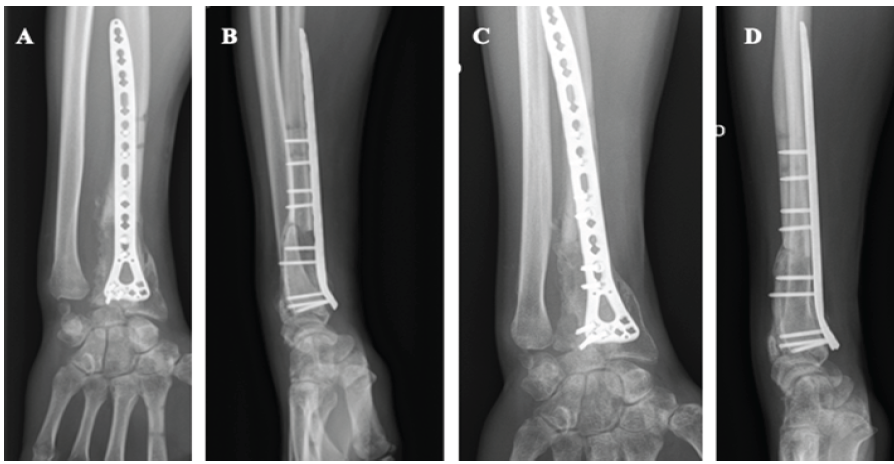
Figure 3: Anterior-posterior (a) and lateral (b) X-ray views 3 months after definitive distal radius fracture osteosynthesis with iliac crest bone graft. Equivalent X-rays presenting anterior-posterior (c) and lateral (d) views 2 years after definitive fixation.
An acceptable range of motion was observed (flexion 85°, extension 30°, and complete prono-supination), with a VAS score of 1, a quick DASH score of 15.9, and a PRWE of 30.5. This patient presented no limitations for daily living activities, including recreational sports. A 68-year-old male patient presented to us with a left midcarpal bone tumour originating from the trapezoid bone with more than 1 year of evolution (Fig. 4a and b). The clinical behaviour and magnetic resonance imaging were consistent with a locally aggressive bone tumour, with a core needle biopsy showing features supporting an osteoblastoma diagnosis (Figs. 4c, d and e).
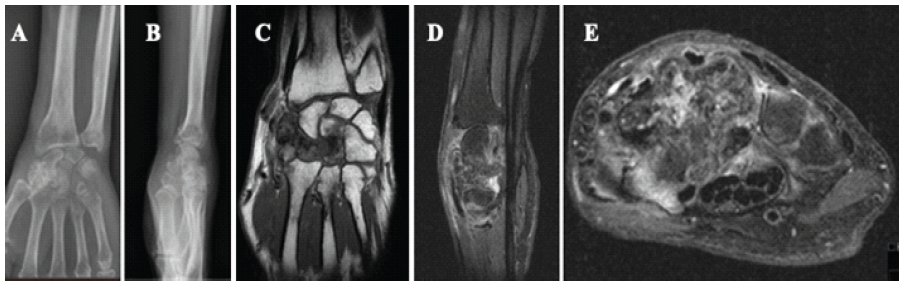
Figure 4: Anterior-posterior (a) and lateral (b) X-ray views presenting a locally aggressive carpal bone tumor; T1-weighted coronal image showing a bone tumor within the trapezium, trapezoid, and capitate areas (c); T1 fat-saturation-weighted sagittal (d) and axial (e) images of the same tumor and anatomical relations.
After discussion at the bone tumour multidisciplinary meeting, we promoted a tumour-wide resection, which caused a significant bone defect (30.7 × 27.2 mm). As such, our reconstructive strategy was based on a carpal arthrodesis (lunate-hamate-second and third metacarpal) using an iliac crest autograft (Fig. 5a and b).
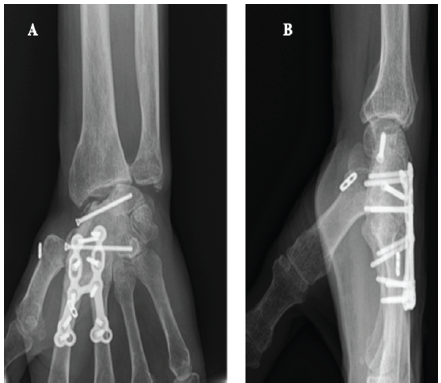
Figure 5: Anterior-posterior (a) and lateral (b) views of X-rays at final follow-up after tumor resection and carpal arthrodesis (lunate-hamate-second and third metacarpal) using an iliac crest autograft.
With almost 2 years of follow-up, bony fusion was achieved, with the patient presenting a moderate wrist motion (15° of flexion, 20° of extension, and complete pronation-supination), no finger movement restriction, a VAS score of 0, a quick DASH score of 15.9, and a PRWE of 24 and being able to perform all daily living activities.
In recent decades, advances in the treatment of hand and wrist bone defects have significantly influenced how surgeons approach these injuries, especially with a growing trend towards limb preservation, even in cases of substantial defects [7,8].
Non-vascularised iliac crest autograft has been described as an efficient and reliable procedure to fill bone defects in hand and wrist surgery [9]. Iliac crest bone grafts are a rich source of growth factors with a wide surface area, allowing bone formation and fast incorporation into the host site. It is relatively easy and rapid to harvest a generous amount of bone with limited donor-site morbidity [10,11]. Sen and Miclau reviewed the advantages of using iliac crest bone graft and suggested that it is the most cost-effective graft, especially to treat non-unions, due to unique osteogenic, osteoinductive, and osteoconductive characteristics [10]. Mehta et al. compared the intrinsic stem cell-like properties of the iliac crest and distal radius bone grafts and concluded that the iliac crest bone graft demonstrated a higher fibroblast colony-forming unit capacity and an increased capability to undergo both osteogenesis and adipogenesis [11]. Despite the well-known advantages of vascularised bone grafts, such as faster integration, less bone resorption, and better fracture healing potential, literature reports similar functional outcomes, including pain and joint range of motion, compared with non-vascularised bone grafts when approaching limited bone defects [9,12]. Vascularised grafts might be advantageous in bigger defects, although the literature is not consistent with the size limit for which these autografts are recommended. Some studies suggest a threshold of 5 cm, others between 6 and 7 cm [12,13]. Clarkson et al. studied 27 patients who underwent wrist arthrodesis after resection of a giant cell tumour of the distal radius using a vascularised free fibular graft or a non-vascularised structural iliac crest autograft. They concluded that although both techniques were effective regarding wrist functional outcomes, vascularised free fibular transfer should be considered only when a major skin defect is anticipated, allowing the inclusion of a vascularised skin paddle, or when the osseous defect is longer than 10 cm [14]. Furthermore, a systematic review by Allsopp et al. concluded that there was insufficient data to establish a relationship between the length of the graft and the need for vascular supply [15]. Furthermore, surgical and post-operative complications related to vascularised bone graft techniques must be considered, which favour non-vascularised bone grafts when treating small defects, such as the ones usually occurring within the wrist and hand [16,17]. Ebad Ali et al. performed a systematic review reporting functional outcomes of reconstruction after resection of bone tumours with both types of autografts. Although reporting quicker bone union and earlier recovery with vascularised grafts, functional outcomes remained the same in both groups, considering pain, range of motion, load-carrying abilities, and other social activities [18]. In both our cases, the graft allowed us to restore the anatomy of the upper limb, restoring the length and stabilising the distal radial and carpal structures, with a pain-free result. The choice for an iliac crest autograft to reconstruct the distal radius defect in Patient 1 was based on the ability to provide fast restoration of the anatomic configuration in the best possible way. The major handicap for this strategy relied on the absence of cartilage to replace the lost lunar articular surface. Nonetheless, there are limited options to provide a better reconstruction, namely with a fresh osteo-cartilaginous allograft, which is hard to obtain in our daily practice. Taking all together, the iliac crest graft and its intrinsic characteristics were favourable to bone consolidation and stable osteosynthesis, which were paramount in this scenario. In similar fashion, the limited defect presented by patient 2 after tumour resection was well reconstructed using an iliac crest autograft. Hand anatomic configuration was immediately restored, and despite the carpal fusion, there was an opportunity to maintain partial motion of the radio-carpal articulation. At the same time, a fast hand and wrist grip strength recovery, with no pain, was achieved. Immediate surgical reconstruction with bone autograft is recommended; in both cases, we chose a single-stage approach [19]. Primary osteosynthesis and immediate cortico-cancellous bone grafting are a reliable option to restore anatomy and preserve bone length (keeping muscles and ligaments under normal tension), thus reducing the risk of contracture and providing decent cosmetic and functional results [20,21]. For both cases that was the strategy followed, which was always supported by a stable osteosynthesis that provided a minimal post-operative period of casting and early rehabilitation [2.1]. This fact is particularly important since it will facilitate early return to work, reduce medical expenses, and minimise patient financial burden.
A non-vascularised bone graft from the iliac crest is a safe, reliable, and reproducible option to treat hand and wrist bone defects in different clinical scenarios. In addition, iliac crest autografts have a low rate of donor site morbidity, allowing fast osteointegration and mechanical stability.
Non-vascularised iliac crest autograft is an effective single-stage option for selected hand and wrist bone defects, allowing anatomical restoration and functional recovery.
References
- 1. Ng CY, Watts AC. The use of non-vascularised osteochondral autograft for reconstruction of articular surfaces in the hand and wrist. J Bone Joint Surg Br 2012;94:1448-54. [Google Scholar] [PubMed]
- 2. Smith RJ, Brushart TM. Allograft bone for metacarpal reconstruction. J Hand Surg Am 1985;10:325-34. [Google Scholar] [PubMed]
- 3. Bruner JM. Use of single iliac-bone graft to replace multiple metacarpal loss in dorsal injuries of the hand. J Bone Joint Surg Am 1957;39-A:43-52. [Google Scholar] [PubMed]
- 4. Torpey B, Faierman E, Lehmann O. Phalangeal transfer for recurrent giant-cell tumor of the phalanx of a finger in a nine-year-old child. A case report with forty-one-year follow-up. J Bone Joint Surg Am 1994;76:1864-9. [Google Scholar] [PubMed]
- 5. Grechenig S, Worlicek M, Penzkofer R, Zeman F, Kujat R, Heiss P, et al. Bone block augmentation from the iliac crest for treatment of deep osteochondral defects of the knee resembles biomechanical properties of the subchondral bone. Knee Surg Sports Traumatol Arthrosc 2019;27:2488-93. [Google Scholar] [PubMed]
- 6. Kim PH, Leopold SS. Gustilo-Anderson classification. Clin Orthop Relat Res 2012;470:3270-4. Erratum in: Clin Orthop Relat Res 2012;470:3624. Erratum in: Clin Orthop Relat Res 2019;477:2388. [Google Scholar] [PubMed]
- 7. Yamamoto N, Hayashi K, Tsuchiya H. Progress in biological reconstruction and enhanced bone revitalization for bone defects. J Orthop Sci 2019;24:387-92. [Google Scholar] [PubMed]
- 8. Migliorini F, La Padula G, Torsiello E, Spiezia F, Oliva F, Maffulli N. Strategies for large bone defect reconstruction after trauma, infections or tumour excision: A comprehensive review of the literature. Eur J Med Res 2021;26:118. [Google Scholar] [PubMed]
- 9. Lesensky J, Nemec K, Kofranek I, Matejovsky Z Jr. Autologous structural iliac bone grafts in reconstructions of short bone defects in the hand and foot after primary bone tumor resections: A single-institution retrospective study. Eur J Orthop Surg Traumatol 2017;27:797-804. [Google Scholar] [PubMed]
- 10. Sen MK, Miclau T. Autologous iliac crest bone graft: Should it still be the gold standard for treating nonunions? Injury 2007;38 Suppl 1:S75-80. [Google Scholar] [PubMed]
- 11. Mehta DD, Dankert JF, Buchalter DB, Kirby DJ, Patel KS, Rocks M, et al. Distinct cell-intrinsic functional differences between iliac crest and distal radius autografts. J Hand Surg Am 2024;49:182.e1-10[3.1]. [Google Scholar] [PubMed]
- 12. Taylor GI, Miller GD, Ham FJ. The free vascularized bone graft. A clinical extension of microvascular techniques. Plast Reconstr Surg 1975;55:533-44. [Google Scholar] [PubMed]
- 13. Soucacos PN, Kokkalis ZT, Piagkou M, Johnson EO. Vascularized bone grafts for the management of skeletal defects in orthopaedic trauma and reconstructive surgery. Injury 2013;44 Suppl 1:S70-5. [Google Scholar] [PubMed]
- 14. Clarkson PW, Sandford K, Phillips AE, Pazionis TJ, Griffin A, Wunder JS, et al. Functional results following vascularized versus nonvascularized bone grafts for wrist arthrodesis following excision of giant cell tumors. J Hand Surg Am 2013;38:935-40.e1. [Google Scholar] [PubMed]
- 15. Allsopp BJ, Hunter-Smith DJ, Rozen WM. Vascularized versus nonvascularized bone grafts: What Is the evidence? Clin Orthop Relat Res 2016;474:1319-27. [Google Scholar] [PubMed]
- 16. Arai K, Toh S, Tsubo K, Nishikawa S, Narita S, Miura H. Complications of vascularized fibula graft for reconstruction of long bones. Plast Reconstr Surg 2002;109:2301-6. [Google Scholar] [PubMed]
- 17. Fujihara Y, Yamamoto M, Hidaka S, Sakai A, Hirata H. Vascularised versus non-vascularised bone graft for scaphoid nonunion: Meta-analysis of randomised controlled trials and comparative studies. JPRAS Open 2023;35:76-88. [Google Scholar] [PubMed]
- 18. Ebad Ali SM, Razak S, Khan WF, Khan S, Khaimchandani D, Akhtar UR, et al. Outcomes of reconstruction with vascularized vs non vascularized bone graft after resection of bone tumours- a systematic review and meta-analysis. J Ayub Med Coll Abbottabad 2023;35:307-12. [Google Scholar] [PubMed]
- 19. Stahl S, Lerner A, Kaufman T. Immediate autografting of bone in open fractures with bone loss of the hand: A preliminary report. Case reports. Scand J Plast Reconstr Surg Hand Surg 1999;33:117-22. [Google Scholar] [PubMed]
- 20. Saint-Cyr M, Miranda D, Gonzalez R, Gupta A. Immediate corticocancellous bone autografting in segmental bone defects of the hand. J Hand Surg Br 2006;31:168-77. [Google Scholar] [PubMed]
- 21. Freeland AE, Jabaley ME, Burkhalter WE, Chaves AM. Delayed primary bone grafting in the hand and wrist after traumatic bone loss. J Hand Surg 1984;9:22-8. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 An Economically Feasible Solution for Distal Radius Fractures Treated with Column-specific Fixation
March 1, 2026 An Economically Feasible Solution for Distal Radius Fractures Treated with Column-specific Fixation December 1, 2025 Recurrent Giant Cell Tumor of the Carpal Bones in an Adult Male Managed by En-bloc Excision, Extended Curettage, Bone Grafting, and all-Kirschner Wire Fixation: A Rare Case Report and Literature Review
December 1, 2025 Recurrent Giant Cell Tumor of the Carpal Bones in an Adult Male Managed by En-bloc Excision, Extended Curettage, Bone Grafting, and all-Kirschner Wire Fixation: A Rare Case Report and Literature Review December 1, 2025 Functional and Radiological Outcomes Following Volar Locking Plate Fixation for Distal Radius Fractures: A Prospective Analytical Study
December 1, 2025 Functional and Radiological Outcomes Following Volar Locking Plate Fixation for Distal Radius Fractures: A Prospective Analytical Study November 1, 2025 The Use of a Tendon Protector Sheath for Prevention of First Extensor Compartment Tendon Adhesions after Radial Column Plating for Distal Radius Fracture: A Case Report
November 1, 2025 The Use of a Tendon Protector Sheath for Prevention of First Extensor Compartment Tendon Adhesions after Radial Column Plating for Distal Radius Fracture: A Case Report