
Simultaneous correction of coronal plane varus deformity and abnormal posterior tibial slope during medial open-wedge proximal tibial osteotomy is essential in post-traumatic proximal tibial malunion to restore limb alignment, optimize knee biomechanics, and achieve favorable functional outcomes.
Dr. Kuru Parvir, Department of Orthopaedics, SDH Moonak, Sangrur - 148033, Punjab, India. E-mail: kpsingla9697@gmail.com
Abstract
Introduction: Malunion of proximal tibial fractures may lead to angular deformity, altered limb alignment, and abnormal knee biomechanics. Varus malalignment increases medial compartment loading and predisposes the knee to progressive pain, instability, and early osteoarthritis. In addition, changes in posterior tibial slope can significantly influence knee kinematics and cruciate ligament biomechanics. Corrective osteotomy remains the standard surgical treatment for symptomatic deformities. Medial open-wedge high tibial osteotomy allows controlled correction of coronal plane deformity while preserving bone stock and enabling simultaneous adjustment of posterior tibial slope. We present a case of post-traumatic genu varum with increased posterior tibial slope successfully managed with medial open-wedge proximal tibial osteotomy.
Case Report: A 39-year-old male presented with persistent pain, instability, and deformity of the left knee 10 months after sustaining a proximal tibial fracture that had been treated conservatively. Clinical examination demonstrated approximately 9° varus deformity. Radiological evaluation, including scanogram and computed tomography, revealed proximal tibial malunion with genu varum, decreased medial proximal tibial angle (78.1°), and increased posterior tibial slope of 14°, along with medial deviation of the mechanical axis and early degenerative changes. The patient underwent medial open-wedge proximal tibial osteotomy under fluoroscopic guidance. Controlled opening of the osteotomy allowed simultaneous correction of coronal plane varus deformity and restoration of posterior tibial slope. The osteotomy gap was filled with ipsilateral iliac crest cancellous bone graft and stabilised using a proximal tibial osteotomy plate. Postoperatively, early mobilisation and gradual weight-bearing were initiated. Radiographs confirmed restoration of mechanical alignment and correction of posterior tibial slope to approximately 6°. Functional outcome improved significantly, with the Lysholm knee score improving from 52 preoperatively to 94 at 1-year follow-up, indicating excellent functional recovery.
Conclusion: Medial open-wedge proximal tibial osteotomy is an effective technique for correcting post-traumatic genu varum with associated posterior tibial slope abnormalities. Simultaneous correction of coronal and sagittal plane deformities restores knee biomechanics, improves functional outcomes, and may prevent progression of degenerative joint changes.
Keywords: Post-traumatic genu varum, high tibial osteotomy, medial open-wedge osteotomy, posterior tibial slope, proximal tibial malunion, limb alignment correction.
Proximal tibial fractures are common injuries resulting from high-energy trauma in younger individuals and low-energy falls in older adults. These fractures significantly influence knee biomechanics, and inadequate reduction or prolonged conservative treatment may result in malunion. Malunion of the proximal tibia leads to angular deformities, altered load distribution across the knee joint, pain, instability, and early degenerative changes [1,2,3,4,5]. Varus malunion of the proximal tibia is particularly disabling, as it increases medial compartment loading, leading to progressive pain, functional limitation, and early osteoarthritis [1,6]. Once malunion is established, conservative management is usually ineffective, and surgical correction becomes necessary to restore mechanical alignment and improve function. In addition to coronal plane deformity, post-traumatic proximal tibial malunion may be associated with abnormal posterior tibial slope, which alters knee kinematics and increases stress on the cruciate ligaments [4]. Failure to address sagittal plane deformity may compromise functional outcomes despite adequate coronal alignment correction. Corrective osteotomy remains the cornerstone of management for symptomatic proximal tibial malunions. Among available techniques, medial open-wedge proximal tibial osteotomy (MOWHTO) allows accurate correction of varus deformity while preserving bone stock and enabling controlled restoration of the mechanical axis [3]. We report a case in which MOWHTO was performed with simultaneous correction of coronal plane deformity and posterior tibial slope, resulting in restoration of alignment and improved knee function.
Patient information:
A 39-year-old male presented to the orthopaedics outpatient department with complaints of pain, instability, and deformity of the left knee. The patient sustained a slip-and-fall injury 10 months back, following which he developed pain over the left knee and proximal leg. The patient was diagnosed with a proximal tibial fracture and managed conservatively with slab immobilisation for approximately 1 month at a different hospital. Despite treatment, the patient continued to experience pain, deformity, and instability, leading to significant functional limitation.
Clinical findings:
On examination, a varus deformity around 9° of the left knee was evident. Localised tenderness was present over the proximal tibia with mild swelling around the knee. There was no local rise of temperature or crepitus. Knee range of motion was painful and restricted. With no muscle wasting, distal neurovascular examination was normal.
Diagnostic assessment:
Plain radiographs of the left knee and leg were obtained as part of the initial evaluation. In view of the deformity and to accurately assess limb alignment, a scanogram of both lower limbs was ordered to evaluate the mechanical axis and quantify coronal plane malalignment. A computed tomography scan of the left knee was also performed to assess the extent of proximal tibial malunion, articular surface involvement, and bony anatomy for pre-operative planning (Figs. 1, 2, 3). Radiological evaluation revealed:
- Genu varum with decreased medial proximal tibial angle (MPTA) of 78.1° and altered posterior tibial slope of 14° (Fig. 4 and 5).
- Evidence of a healed proximal tibial fracture with malunion
- Depression of the medial tibial plateau contributing to altered knee biomechanics
- Medial deviation of the mechanical axis of the lower limb
- Early degenerative changes like medial compartment joint space narrowing with early subchondral sclerosis of the medial tibial plateau around the knee joint.

Figure 1: Non-contrast computed tomography images in axial and coronal planes showing the proximal tibial deformity.
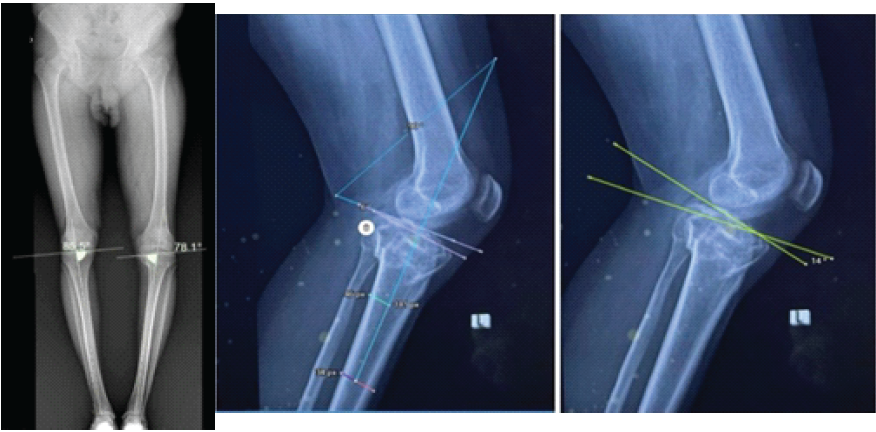
Figure 2: Radiological evaluation showed genu varum with decreased medial proximal tibial angle (78.1°) and increased posterior tibial slope of 14°.
The patient had undergone magnetic resonance imaging (MRI) of the left knee at an outside facility, which was reviewed as part of the pre-operative assessment. MRI revealed a sprain of the anterior cruciate ligament without discontinuity, along with post-traumatic changes involving the proximal tibia. Based on the clinical findings and comprehensive radiological assessment, a diagnosis of post-traumatic genu varum (9°) due to a malunited proximal tibial fracture with an associated increased posterior tibial slope 14° was established.

Figure 3: Intraoperative photograph showing the osteotomy site with opening of the medial wedge under C-arm fluoroscopic guidance.
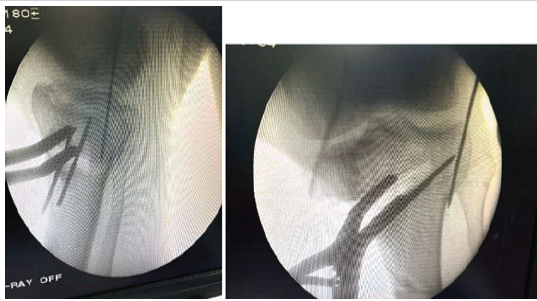
Figure 4: Intraoperative C-arm images showing medial osteotomy opening.
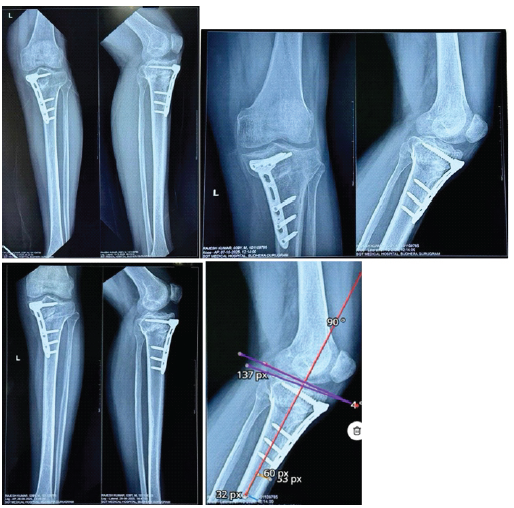
Figure 5: Postoperative radiographs showing implant in situ with restoration of posterior tibial slope at follow-up.
Diagnosis:
Post-traumatic genu varum (9°) due to a malunited proximal tibial fracture with associated increased posterior tibial slope of 14° in the left knee.
Surgical technique:
Preoperative planning:
Corrective medial open-wedge proximal tibial osteotomy with bone grafting and internal fixation was planned to restore coronal and sagittal plane alignment [3,4].
Operative procedure:
The patient was positioned supine on the operating table under epidural anaesthesia. A pneumatic thigh tourniquet was applied and inflated after limb exsanguination. The operative limb was prepared and draped in a sterile fashion. A standard medial approach to the proximal tibia was utilised. A longitudinal incision was made over the anteromedial aspect of the proximal tibia. Dissection was carried down through the subcutaneous tissue, and the pes anserinus was identified and retracted to expose the proximal medial tibial metaphysis. Under fluoroscopic guidance, a MOWHTO was performed. The osteotomy was carefully created, preserving the lateral cortical hinge. Gradual controlled opening of the osteotomy was carried out anteriorly and medially to achieve correction of the coronal plane varus deformity and restoration of the posterior tibial slope. Alignment was repeatedly assessed under image intensification. The osteotomy gap was filled with ipsilateral iliac crest cancellous bone graft to maintain the achieved correction and enhance biological healing. Definitive fixation was achieved using a 3-hole proximal tibial osteotomy plate with appropriate screws, ensuring stable fixation (Fig. 6). Final fluoroscopic images confirmed satisfactory mechanical axis correction, appropriate posterior tibial slope restoration, and stable construct fixation. (Fig. 6).

Figure 6: Clinical photograph at follow-up demonstrating full knee range of motion and return to normal daily activities.
Post-operative management:
Postoperatively, the patient received prophylactic intravenous antibiotics and analgesics. Early ankle and toe mobilization, along with static quadriceps exercises, were initiated. Non-weight-bearing ambulation with walker support was advised, with gradual progression to weight-bearing based on clinical and radiological evidence of healing.
Outcome and follow-up:
At 2 weeks postoperatively, the surgical wound was healthy with no signs of infection. Knee range of motion had improved, and pain was significantly reduced. Post-operative radiographs demonstrated restoration of mechanical axis alignment, along with correction of posterior tibial slope to 6°, and clinically, post-operative varus is 3°. The patient reported improved knee stability with painless weight-bearing. At the 3-month follow-up, radiographs showed maintained alignment with progressive union at the osteotomy site. The patient was able to ambulate comfortably with minimal support. At 1-year follow-up, the patient reported marked functional improvement with painless full weight-bearing. Radiological evaluation demonstrated complete osteotomy union with restoration of mechanical alignment and no implant-related complications. The post-operative scanogram demonstrated restoration of the mechanical axis with improvement of MPTA from 78.1° preoperatively to 87° postoperatively and correction of posterior tibial slope from 14° to 6°.
Functional outcome assessment:
Functional outcome was evaluated using the Lysholm-Gillquist knee scoring scale, a validated patient-reported outcome measure commonly used in ligamentous and deformity correction procedures. Preoperatively, the patient had significant functional limitation with a Lysholm score of 52 (poor outcome), reflecting the following:
- Pain during weight-bearing
- Instability (giving-way episodes)
- Difficulty in stair climbing and squatting
- Limp during
At 3 months postoperatively, the score improved to 82 (fair to good outcome), indicating substantial symptomatic relief and improved knee stability. At the 1-year follow-up, the patient achieved a Lysholm score of 94 (good outcome), demonstrating the following:
- Painless full weight-bearing
- No instability episodes
- Near-normal gait
- Ability to climb stairs and squat with minimal
This progressive improvement in Lysholm score correlated with radiological union, restoration of mechanical alignment, and posterior tibial slope correction. Additional functional outcome measures were also assessed to provide a comprehensive evaluation of post-operative recovery. The Knee Injury and Osteoarthritis Outcome Score (KOOS) improved from 48 pre-operatively to 89 at 1-year follow-up, demonstrating significant improvement in pain, symptoms, activities of daily living, and knee-related quality of life. The International Knee Documentation Committee (IKDC) subjective knee score improved from 42 pre-operatively to 86 postoperatively, reflecting marked functional recovery and improved knee stability.
Malunited proximal tibial fractures remain a complex orthopaedic challenge because of the associated disturbance in lower limb biomechanics, altered load distribution across the knee joint, and progressive degenerative changes. Persistent varus malalignment increases stress across the medial compartment, accelerating cartilage wear and contributing to early osteoarthritic changes if left untreated [1,5,6]. Restoration of the mechanical axis is therefore essential not only for symptomatic relief but also for preservation of long-term knee function. Brouwer et al. demonstrated satisfactory functional outcomes following both opening wedge and closing wedge osteotomy techniques, supporting the role of deformity correction in symptomatic varus knees [7,8]. Posterior tibial slope is another important determinant of knee biomechanics and cruciate ligament function. Abnormal increase in posterior tibial slope following proximal tibial malunion may alter tibiofemoral kinematics, increase anterior tibial translation, and contribute to functional instability [4]. Medial open-wedge proximal tibial osteotomy provides the advantage of controlled correction in both coronal and sagittal planes, making it particularly useful in post-traumatic deformities associated with altered posterior tibial slope [3,9]. In the present case, simultaneous correction of varus malalignment and increased posterior tibial slope resulted in restoration of alignment, improved knee stability, and sustained functional recovery. Functional outcome assessment demonstrated substantial post-operative improvement. The Lysholm–Gillquist Knee Score improved from poor pre-operative function to good functional outcome at 1-year follow-up. Additional validated outcome measures also demonstrated significant recovery, with improvement in KOOS, IKDC, and WOMAC scores correlating with restoration of alignment and radiological union. Clinically, the patient achieved painless full weight-bearing, improved knee stability, a near-normal gait pattern, and a return to routine daily activities without significant limitation. The favourable outcome observed in the present case may be attributed to meticulous pre-operative planning, accurate deformity analysis, preservation of the lateral cortical hinge, stable internal fixation, and structured post-operative rehabilitation. Similar studies have emphasised the importance of precise correction and maintenance of mechanical alignment in achieving satisfactory long-term outcomes following high tibial osteotomy [5,6,10]. Although medial open-wedge proximal tibial osteotomy is associated with potential complications such as lateral cortical hinge fracture, delayed union, non-union, infection, implant irritation, neurovascular injury, and loss of correction, no major complications were encountered in the present case. Careful surgical technique, gradual controlled opening of the osteotomy, biological augmentation with autologous iliac crest cancellous bone graft, and stable plate fixation likely contributed to successful healing and maintenance of correction. Previous literature has similarly reported that preservation of the lateral hinge and stable fixation are critical factors influencing osteotomy healing and complication rates [11,12]. The present case involved a relatively young and active patient with satisfactory bone quality, which favoured predictable healing and rehabilitation following deformity correction. Restoration of native knee biomechanics through corrective osteotomy may help delay progression of degenerative arthritis and postpone the need for joint arthroplasty in younger individuals. Earlier return to functional activity and preservation of the native joint may additionally reduce long-term socioeconomic burden and improve quality of life [10,13,14]. Despite the encouraging outcome, this report represents a single-case experience, and larger studies with longer follow-up are required to further evaluate long-term maintenance of correction, survivorship, and progression of degenerative changes following medial open-wedge proximal tibial osteotomy in post-traumatic genu varum deformity.
Medial open wedge proximal tibial osteotomy is an effective technique for managing post-traumatic genu varum, as it enables simultaneous correction of coronal plane deformity and posterior tibial slope. Restoration of mechanical alignment leads to pain relief, improved knee function, and prevention of progressive degenerative changes. Early recognition and appropriate surgical management are key to achieving favourable long-term outcomes.
Simultaneous correction of coronal alignment and posterior tibial slope should be considered in post-traumatic proximal tibial malunion to optimise knee biomechanics and long-term functional outcomes.
References
- 1. Lee DC, Byun SJ. High tibial osteotomy. Knee Surg Relat Res 2012;24:61-9. [Google Scholar] [PubMed]
- 2. Kuwashima U. High tibial osteotomy: The past, present, and future. J Joint Surg Res 2023;1:103-7. [Google Scholar] [PubMed]
- 3. Pape D, Rupp S. Preoperative planning for high tibial osteotomies. Oper Tech Orthop 2007;17:2-11. [Google Scholar] [PubMed]
- 4. Thomas A, Round J. Basic principles of lower limb deformity correction. Surgery (Oxford) 2023;41:255-61. [Google Scholar] [PubMed]
- 5. Sabzevari S, Ebrahimpour A, Roudi MK, Kachooei AR. High tibial osteotomy: A systematic review and current concept. Arch Bone Jt Surg 2016;4:204-12. [Google Scholar] [PubMed]
- 6. Rossi R, Bonasia DE, Amendola A. The role of high tibial osteotomy in the varus knee. J Am Acad Orthop Surg 2011;19:590-9. [Google Scholar] [PubMed]
- 7. Aglietti P, Rinonapoli E, Stringa G, Taviani A. Tibial osteotomy for the varus osteoarthritic knee. Clin Orthop Relat Res 1983;176:239-51. [Google Scholar] [PubMed]
- 8. Brouwer RW, Bierma-Zeinstra SM, Van Raaij TM, Verhaar JA. Osteotomy for medial compartment arthritis of the knee using a closing wedge or an opening wedge controlled by a Puddu plate. A one-year randomised, controlled study. J Bone Joint Surg Br 2006;88:1454-9. [Google Scholar] [PubMed]
- 9. Pan CS, Wang X, Ding LZ, Zhu XP, Xu WF, Huang LX. The best position of bone grafts in the medial open-wedge high tibial osteotomy: A finite element analysis. Comput Methods Programs Biomed 2023;228:107253. [Google Scholar] [PubMed]
- 10. Naudie D, Bourne RB, Rorabeck CH, Bourne TJ. Survivorship of the high tibial valgus osteotomy. A 10- to -22-year followup study. Clin Orthop Relat Res 1999;367:18-27. [Google Scholar] [PubMed]
- 11. Berk AN, Gachigi KK, Trofa DP, Piasecki DP, Fleischli JE, Saltzman BM. Early postoperative complications and associated variables after high tibial osteotomy and distal femoral osteotomy: A 15-year experience from a single academic institution. Am J Sports Med 2023;51:2574-82. [Google Scholar] [PubMed]
- 12. Pape D. Complications in high tibial (medial opening wedge) osteotomy. Arch Orthop Trauma Surg 2004;124:649-53. [Google Scholar] [PubMed]
- 13. Bastard C, Mirouse G, Potage D, Silbert H, Roubineau F, Hernigou P, et al. Return to sports and quality of life after high tibial osteotomy in patients under 60 years of age. Orthop Traumatol Surg Res 2017;103:1189-91. [Google Scholar] [PubMed]
- 14. Amendola A, Rorabeck CH, Bourne RB, Apyan PM. Total knee arthroplasty following high tibial osteotomy for osteoarthritis. J Arthroplasty 1989;4 Suppl:S11-7. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Arthroscopic Repair of Meniscal Medial Root Tears: The Necessity of Concomitant Realignment Osteotomy
August 1, 2026 Arthroscopic Repair of Meniscal Medial Root Tears: The Necessity of Concomitant Realignment Osteotomy July 1, 2026 All-inside Circumferential Fiber Augmentation of Medial Meniscus Combined with Medial Open-wedge High Tibial Osteotomy
July 1, 2026 All-inside Circumferential Fiber Augmentation of Medial Meniscus Combined with Medial Open-wedge High Tibial Osteotomy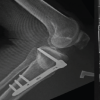 June 1, 2026 Pes Anserinus and Superficial Medial Collateral Ligament Preserving High Tibial Osteotomy Combined with Arthroscopic Medial Meniscus Root Repair for Medial Compartment Osteoarthritis with Varus Deformity: A Prospective Case Series of 20 Patients
June 1, 2026 Pes Anserinus and Superficial Medial Collateral Ligament Preserving High Tibial Osteotomy Combined with Arthroscopic Medial Meniscus Root Repair for Medial Compartment Osteoarthritis with Varus Deformity: A Prospective Case Series of 20 Patients February 1, 2026 Outcome of Medial Open Wedge High Tibial Osteotomy for Knee Osteoarthritis: A Case Series
February 1, 2026 Outcome of Medial Open Wedge High Tibial Osteotomy for Knee Osteoarthritis: A Case Series