
T1ρ mapping primarily reflects proteoglycan loss, while T2 mapping indicates collagen matrix disruption and increased cartilage water content. Combined assessment of T1ρ and T2 values improves prediction of early cartilage loss and may aid in early intervention to prevent post-traumatic osteoarthritis.
Dr. Gourab Biswas, Department of Orthopaedics, Max Superspeciality Hospital, New Delhi, India. E-mail: gourabbiswas2013@gmail.com
Abstract
Introduction: Early cartilage degeneration after anterior cruciate ligament (ACL) injury often precedes structural changes detectable on conventional imaging.
Aim: To evaluate the role of T1ρ and T2 mapping magnetic resonance imaging (MRI) in detecting early cartilage changes and predicting cartilage loss in ACL-injured knees.
Materials and Methods: A multicentric prospective observational study was conducted on 50 patients with early ACL injury. Quantitative MRI with T1ρ and T2 mapping was performed to assess cartilage composition and thickness. The study protocol was approved by the Institutional Ethics Committee, and written informed consent was obtained from all patients before inclusion.
Results: ACL-injured knees demonstrated elevated T1ρ and T2 values along with reduced cartilage thickness. Higher relaxation times correlated with early cartilage degeneration, particularly in patients with longer injury duration and associated meniscal pathology.
Conclusion: T1ρ and T2 mapping MRI are effective non-invasive tools for early detection of cartilage degeneration and may aid in predicting cartilage loss following ACL injury.
Keywords: Anterior cruciate ligament injury, cartilage degeneration, T1ρ mapping, T2 mapping, magnetic resonance imaging.
The anterior cruciate ligament (ACL) injury is a musculoskeletal condition, particularly among young people and athletes, and is a familiar cause of the premature development of post-traumatic osteoarthritis (PTOA) of the knee [1]. The majority of patients who have ACL reconstruction (ACLR) and joint stability despite effective reconstructions and regaining of joint stability experience gradual degeneration of cartilage, which leads to pain, functional losses, and reduction in quality of life 1015 years following injury [2]. Traditional clinical assessment and the regular diagnostic magnetic resonance imaging (MRI) techniques lack sufficient data to reveal the initial biochemical and microstructural changes in the cartilage of the articular joint, which are precursors of irreparable morphological damage [3]. Thus, there is currently an interest in more sophisticated quantitative MRI techniques that would be capable of identifying early cartilage degeneration at a potentially reversible stage and, therefore, be able to intervene at an opportune moment and achieve improved long-term outcomes after ACL injury [4]. Among these techniques, T1 rho (T1 rho) and T2 mapping MRI have been demonstrated to be promising non-invasive biomarkers of cartilage composition and cartilage integrity in vivo [5]. “T1r mapping, which is highly sensitive to the loss of proteoglycan of the cartilage extracellular matrix, is one of the first biochemical modifications to take place following the injury of a joint [6]. The degradation of the proteoglycans renders the cartilage vulnerable to compressive forces, and it is considered one of the primary precipitating factors in the events of cartilage degeneration and the development of osteoarthritis [7]. On the other hand, T2 mapping primarily provides information about the collagen fibro-water structure, which provides data on cartilage hydration and collagen network integrity [8]. The first signs of cartilage destruction and disruption of the collagen structure and high mobility of water are typical of an ACL injury, even in the presence of no visible cartilage deficiencies in the standard MRI tests [9]. There are several longitudinal studies that have indicated that the T1rho and T2 relaxation times are significantly higher in the femur and tibia cartilage compartments in ACL or injured individuals than in healthy controls, suggesting the degeneration of the matrix within a short time following the injury [10]. It is noteworthy that the alterations have been noted in the pre- and post-ACLR, and thus it has been established that the surgical stabilisation alone might not be adequate to inhibit the onwards cartilage degeneration [11]. Additional emergent evidence suggests that a post-ACL injury rise in baseline T1r and T2 values is predictive of cartilage thinning, volume decrease, and time osteoarthritis radiographic features [12]. This prediction capability is particularly true in the early post-injury period when the standard imaging is normal, but cartilage biochemical changes are already progressing [13]. The capacity to utilize T1r and T2 mapping as early imaging biomarkers of cartilage loss might hence provide the necessary prognostic information, which may be a risk stratifier and in patient-specific management. The quantitative MRI techniques also present helpful evaluations of the efficacy of disease-modifying interventions, rehabilitation, and new cartilage-preserving therapies of ACL-injured populations. However, T1r and T2 mapping have not been applied in clinical practice due to inconsistency in imaging regimes, difference in post-processing approaches, and variations in standardized thresholds to predict clinically significant cartilage loss despite potentials. In addition, comparative and auxiliary capabilities of T1r and T2 mapping in the signal of long-term cartilage consequences following early ACL injury are also being studied. In this way, T1 r and T2 MRI mapping of the cartilage in patients with early ACL injury are important predictors of cartilage loss that have to be thoroughly considered to gain a deeper insight into the post-traumatic cartilage degeneration, and facilitate the translation of quantitative MRI biomarkers into clinical and research practice.
Study design:
The study was conducted as a multicentric prospective observational cohort study across the Departments of Orthopaedics and Radiology at multiple tertiary care teaching hospitals equipped with advanced musculoskeletal imaging facilities. The study protocol was approved by the Institutional Ethics Committees of all participating centres, and written informed consent was obtained from all patients before inclusion. The study was designed to evaluate the role of T1ρ and T2 mapping magnetic resonance imaging (MRI) as predictors of early cartilage degeneration following ACL injury. The study protocol was approved by the institutional ethics committees of all participating centres, and written informed consent was obtained from all patients before inclusion in the study.
Study setting:
The study was conducted as a multicentric investigation across the Departments of Orthopaedics and Radiology at multiple tertiary care teaching hospitals, all equipped with advanced musculoskeletal imaging facilities.
Study duration:
The study was carried out over a period of 18 months, including participant recruitment, baseline clinical evaluation, MRI acquisition, image processing, and data analysis.
Participants:
Patients presenting with knee injury suggestive of ACL tear were screened for eligibility. Recruitment was performed after confirming ACL injury through clinical examination and conventional MRI.
Inclusion criteria:
- Patients aged 18–40 years
- Patients with clinically and MRI-confirmed acute or subacute ACL injury
- Duration of injury ≤6 months
- No prior surgical intervention on the affected knee
- Willingness to provide written informed consent.
Exclusion criteria:
- Evidence of advanced osteoarthritis (Kellgren–Lawrence grade ≥2)
- History of previous knee surgery or fracture involving the affected knee
- Concomitant ligament injuries requiring immediate surgical management
- Inflammatory arthritis or systemic connective tissue disorders
- Contraindications to MRI (e.g., pacemakers, metallic implants, claustrophobia).
Study sampling:
A consecutive sampling method was used. All eligible patients presenting during the study period who fulfilled the inclusion criteria were recruited until the required sample size was achieved.
Study sample size:
The total sample size for the study was 50 participants. The sample size was selected based on feasibility, availability of eligible patients within the study duration, and consistency with previous imaging-based observational studies assessing quantitative MRI biomarkers in ACL injury.
Study groups:
Participants were categorised into two groups based on MRI findings:
- Group A: ACL-injured knees (affected knees)
- Group B: Contralateral uninjured knees or age-matched healthy controls (where applicable).
This grouping enabled comparison of quantitative cartilage parameters between injured and non-injured knees.
Study parameters:
The primary study parameters included:
- T1ρ relaxation time values of articular cartilage
- T2 relaxation time values of articular cartilage.
Secondary parameters included:
- Cartilage thickness and volume measurements
- Compartment-wise cartilage assessment (medial femoral, lateral femoral, tibial, and patellar cartilage)
- Demographic variables, such as age, sex, body mass index, and time since injury.
Study procedure:
Once the participants were enrolled, a comprehensive clinical assessment of the participants was conducted, which included history taking and physical examination of the knee joint. The ACL injury was initially confirmed by conventional MRI sequences to evaluate the related abnormalities in the meniscal or cartilage. Quantitative MRI acquisition of the T1rho and T2 mapping sequences with standardized imaging protocols followed this step. Trained radiologists who had no knowledge of clinical data manually (or semi-manually) segmented the cartilage areas of interest. Quantitative relaxation maps have been determined, and mean relaxation times of pre-determined cartilage compartments were observed.
Study data collection:
The information on clinical data was captured on a structured pro forma, which contained demographic information, characteristics of the injury, and the clinical findings. Quantitative data were obtained using MRI and stored electronically, and brought out to be analyzed. Anonymisation of all imaging data was done to protect the confidentiality of participants. The data quality checks were used to reduce variability in observers and allow uniformity in measurement.
Data analysis:
The data collected were inputted into a spreadsheet, and statistical software was used to analyse the obtained data. Continuous variables were reported in terms of the mean and the standard deviation, whereas the categorical variables were reported in terms of their frequencies and percentages. The statistical tests, such as the independent t-test or Mann-Whitney U test, were used to carry out comparative analysis between the groups. Correlation analysis was used to determine the association between T1rho and T2 values and cartilage thickness or cartilage volume. A P-value that was below 0.05 was taken as significantly important.
Demographic profile and ACL injury characteristics:
The study population consisted mainly of young adults with a predominance of males. Most patients had complete ACL tears, and a considerable proportion presented with associated meniscal injury and bone contusion, indicating complex joint trauma early after injury (Table 1).
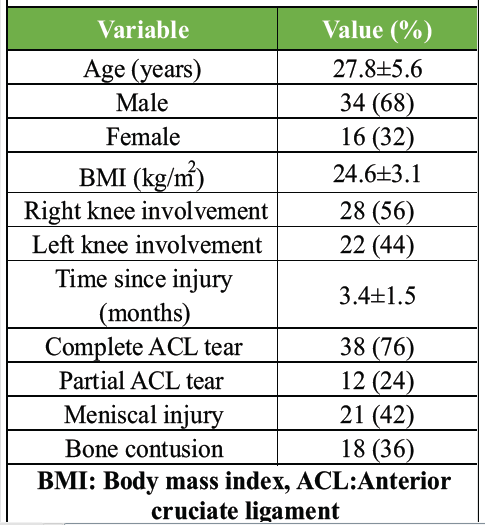
Table 1: Demographic profile and ACL injury characteristics (n=50)
Quantitative MRI relaxation values (T1ρ and T2) in injured versus control knees:
ACL-injured knees demonstrated significantly higher T1ρ and T2 relaxation values across all cartilage compartments compared with controls. These elevated values indicate early biochemical cartilage degeneration, including proteoglycan depletion and collagen matrix disruption (Table 2 and Fig. 1).
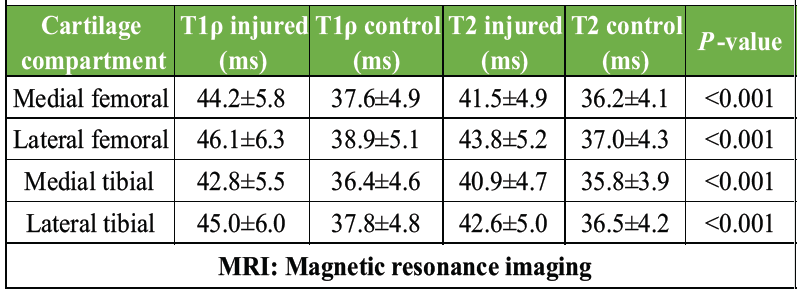
Table 2: Quantitative MRI relaxation values (T1ρ and T2) in injured versus control knees
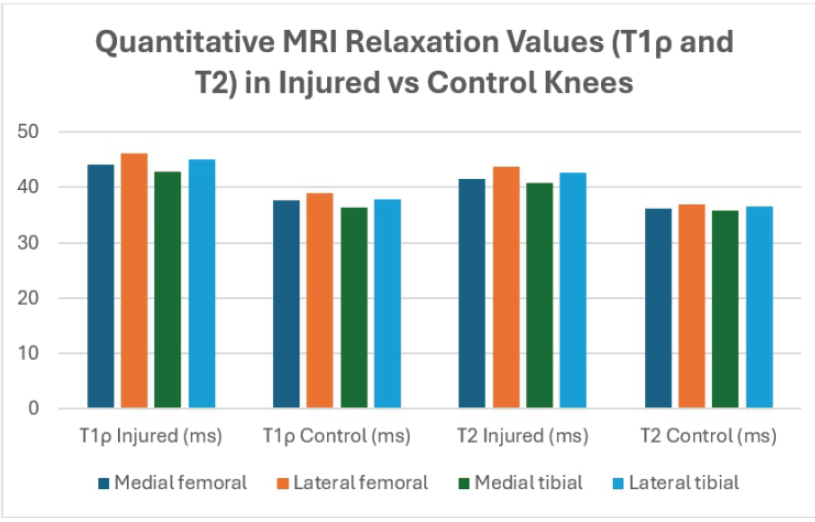
Figure 1: Quantitative magnetic resonance imaging relaxation values (T1ρ and T2) in injured versus control knees.
Cartilage thickness and time-dependent changes after ACL injury:
Significant cartilage thinning was observed in ACL-injured knees despite the absence of visible structural abnormalities on routine MRI. In addition, T1ρ values increased with time since injury, suggesting progressive biochemical cartilage deterioration in the early post-injury period (Table 3 and Fig. 2).
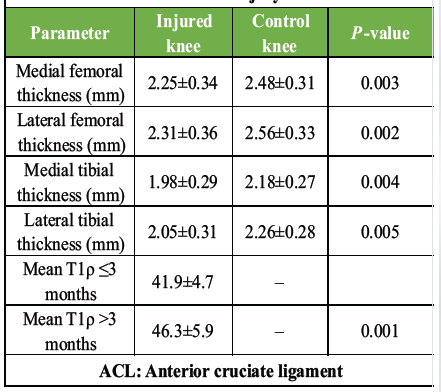
Table 3: Cartilage thickness and time-dependent changes after ACL injury
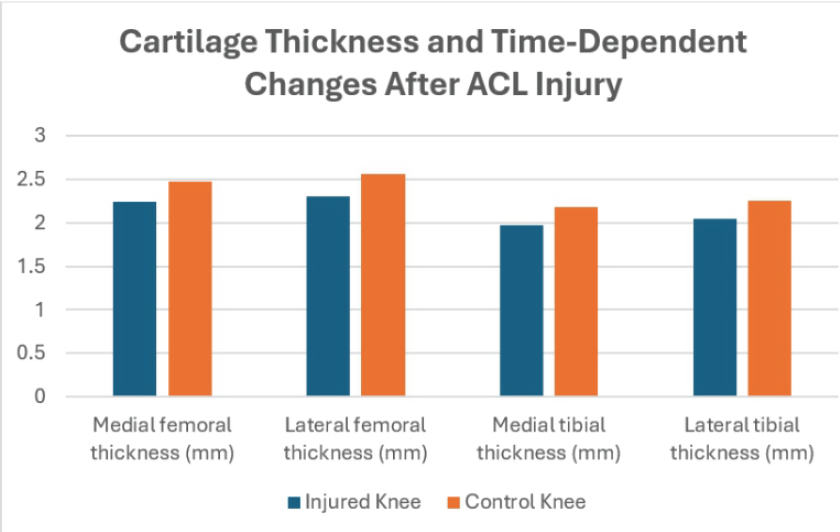
Figure 2: Cartilage thickness and time-dependent changes after anterior cruciate ligament injury.
Correlation and predictive factors of early cartilage loss:
Higher T1ρ and T2 relaxation times showed a significant negative correlation with cartilage thickness, confirming that biochemical degeneration is associated with structural cartilage loss. The combined elevation of T1ρ and T2 demonstrated the strongest predictive value for early cartilage degeneration following ACL injury (Table 4).
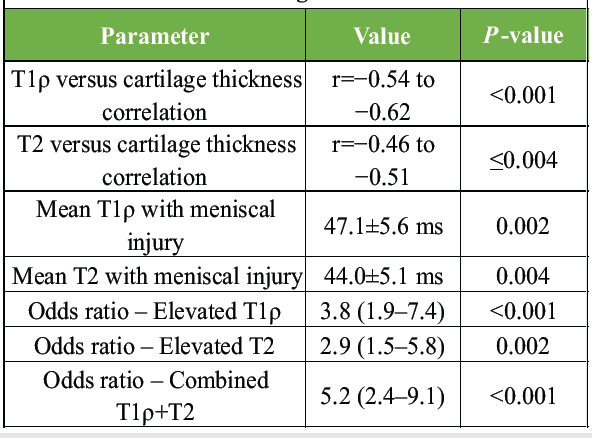
Table 4: Correlation and predictive factors of early cartilage loss
The present research has shown that quantitative MRI methods, namely, T1rr and T2 mapping, are sensitive indicators of early cartilage degeneration following ACL injury, even in a rather short period after the injury. We found significantly increased T1 4 values in all femorotibial compartments compared to the control knees in our group of 50 patients with early ACL injury (mean time since injury 3.4 + 1.5 months), with medial femoral values of 44.2 + 5.8 ms and lateral femoral values of 46.1 + 6.3 ms, and similarly increased T2 values (medial femoral 41.5 + 4.9 ms; lateral femoral 43.8 + 5.2 ms). These results indicate proteoglycan loss and collagen matrix breakdown earlier before morphologic abnormalities of the cartilage are observed. The findings are in good accord with the longitudinal studies of Williams et al. [14], which proved that initial changes of cartilage T2 parameters after ACLR were the predictors of subsequent cartilage degeneration. The 6-month variation in mean T2 between 17 ACLR patients indicated that early T2 texture changes were related to 2-year changes in mean T2 (R = 0.80, P = 0.0001), and early T2 texture changes were associated with subsequent medial femoral cartilage thickness loss (R = 0.48 − 0.72, P = 0.05). Although our measurement did not encompass the analysis of the texture, the observed increases in the T2 values and the strong negative correlations between T2 relaxation times and cartilage thickness (r = −0.46 −0.51, P = 0.004 or less) are in line with the trend of predictance of the biochemical changes of the early stages and subsequent structural damages as reported by Williams et al. [14]. Furthermore, the much smaller than normal cartilage thickness of our injured knees, which includes: Medial femoral thickness of 2.25 + 0.34 mm versus 2.48 + 0.31 mm in controls (P = 0.003), endorses the idea that early compositional alterations observed by T2 mapping are clinically important predictors of subsequent cartilage alteration. The role played in the T1R mapping of early cartilage degeneration was further supported by the comparison with the results of Osaki et al., [15] where the T1R mapping was done on 49 ACL-injured knees and the values showed a rise with the number of years elapsed after the injury, especially after 2 years. Osaki et al. found criminally high results of T1 r in the anterior and middle of the medial femur condyle when patient duration of injury was over 2 years compared with those of patients injured under 12 weeks and 12 weeks-2 years (P = 0. 05) [2]. A comparable time-dependent effect was also found, even though our cohort looked at a much earlier phase after injury, the mean T1R values were significantly larger in patients measured more than 3 months after injury (46.3 ± 5.9 ms) than in patients measured <3 months (41.9 ± 4.7 ms; P = 0.001). This stability implies that the degradation of proteoglycans starts early following ACL injury and evolves over time, which further supports a biological possibility of T14 as a sensitive indicator of early cartilage depletion. Effects of meniscal injury on cartilage health in our case are also in line with the study by Osaki et al. [15], who determined that patients with medial meniscus injury and a post-injury period of 12 weeks and longer had significantly higher T1 0 in the medial femur condyle than normal knees and ACL-injured knees, where there was no meniscal injury. The patients with comorbid meniscal tears also had significantly greater mean T1 (0.47 ± 0.56 ms vs. 42.9 ± 0.48 ms; P = 0.002) and T2 (0.44 ± 0.51 ms vs. 40.6 ± 0.45 ms; P = 0.004) in our analysis, which also points out that meniscal pathology has a compounding effect on cartilage matrix breakdown manifested as these results also confirm the idea that any changes in joint loading and shock absorption after meniscal damage hastens biochemical cartilage degradation in ACL injury. Our findings of a correlation between T1-elevation and early cartilage lesions are also aligned with the results of Hirose et al. [16], who assessed sagittal T1 maps in 23 individuals before and 1 year following ACLR. The baseline T1r values were found to be significantly higher in patients with cartilage lesions arthroscopically confirmed, with values of 40.7 ms and 38.0 ms at the medial femoral condylar site in those with lesions and 43.1 ms at the 1-year follow-up, respectively (Hirose et al., [16]) in patients with lesions versus 38.0 ms in patients without lesions (P = 0.025). Compared to that, the mean medial femoral T1 value in our ACL-injured patients (44.2 + 5.8 ms) relates closely with those of 1 year post-ACLR in the study by Hirose et al., although our patients were tested at a much earlier stage of the disease. This implies that significant changes in biochemical cartilages can be noticed shortly after ACL injury, and this is before surgery. The presence of the diagnostic performance of the T1 r and T2 mapping observed in our study is also justified by the results of Nishioka et al. [17], who proved that both T1 r and T2 mapping could identify International Cartilage Repair Society grade 1 cartilage lesions with high accuracy. It was found that cut-off values of 41.6 ms (T1rho) and 41.2 ms (T2) were identified, with T1rho having a sensitivity of 91.2 and specificity of 89.5 and T2 feasibility with a sensitivity of 76.5 and specificity of 81.6, based on the Nishioka et al. finding of the use of arthroscopy as the reference standard. Interestingly, some of the compartments of our ACL-injured knees had a higher mean value of T1r and T2 than these cut-off values, and they suggest that there were initially present defects in the cartilage matrix without any gross morphological abnormalities. This observation confirms the finding that quantitative MRI techniques have a greater ability to detect minor cartilaginous damage than conventional morphological imaging.” Finally, the correlation between the degeneration of the meniscus and cartilage in our study is comparable to the longitudinal results of Knox et al., who evaluated T14 and T2 of the meniscus and cartilage of the 2 years after the ACL injury and reconstruction. Knox et al. [18] reported that T1r/T2 signals more consistently showed increased signals in the anterior horn of the medial meniscus at all time points after reconstruction that were significantly positively correlated with medial tibial cartilage T1rT2 values. On the same note, we were able to show that cartilage T14 and T2 were higher in patients with meniscal injury, which reflected the interrelationship of degeneration in meniscal and articular cartilage tissues. Taken together, the interpretation of the present findings, together with the previous studies, is that T1r and T2 mapping MRI is highly indicative of early and progressive degeneration of the biochemical cartilage following ACL injury and early cartilage thinning and has a relationship with the chronicity of injury and meniscal pathology. These are quantitative imaging biomarkers and are thus promising in the early risk stratification, tracking disease progression, and implementation of timely interventions to prevent or delay the development of PTOA.
T1ρ and T2 mapping MRI are sensitive, non-invasive imaging biomarkers capable of detecting early biochemical cartilage degeneration following ACL injury, even before structural changes become evident on conventional imaging. Elevated relaxation times and reduced cartilage thickness observed in this study indicate early matrix deterioration and progressive cartilage loss. The significant association of these parameters with time since injury and concomitant meniscal pathology highlights their role in identifying high-risk patients. Combined assessment of T1ρ and T2 values enhances predictive accuracy and may facilitate early risk stratification, monitoring of disease progression, and timely intervention to prevent PTOA.
Early biochemical cartilage degeneration occurs soon after ACL injury and can be detected using quantitative MRI techniques, such as T1ρ and T2 mapping. These imaging biomarkers allow identification of cartilage damage before morphological changes appear on conventional MRI.
References
- 1. Fithian DC, Paxton LW, Goltz DH. Fate of the anterior cruciate ligament-injured knee. Orthop Clin North Am 2002;33:621-36. [Google Scholar] [PubMed]
- 2. Nelson F, Billinghurst RC, Pidoux I, Reiner A, Langworthy M, McDermott M, et al. Early post-traumatic osteoarthritis-like changes in human articular cartilage following rupture of the anterior cruciate ligament. Osteoarthritis Cartilage 2006;14:114-9. [Google Scholar] [PubMed]
- 3. Von Porat A, Roos EM, Roos H. High prevalence of osteoarthritis 14 years after an anterior cruciate ligament tear in male soccer players: A study of radiographic and patient relevant outcomes. Ann Rheum Dis 2004;63:269-73. [Google Scholar] [PubMed]
- 4. Potter HG, Jain SK, Ma Y, Black BR, Fung S, Lyman S. Cartilage injury after acute, isolated anterior cruciate ligament tear: immediate and longitudinal effect with clinical/MRI follow-up. Am J Sports Med 2012;40:276-85. [Google Scholar] [PubMed]
- 5. Su F, Hilton JF, Nardo L, Wu S, Liang F, Link TM, et al. Cartilage morphology and T1rho and T2 quantification in ACL-reconstructed knees: A 2-year follow-up. Osteoarthritis Cartilage 2013;21:1058-67. [Google Scholar] [PubMed]
- 6. Barenius B, Ponzer S, Shalabi A, Bujak R, Norlén L, Eriksson K. Increased risk of osteoarthritis after anterior cruciate ligament reconstruction: A 14-year follow-up study of a randomized controlled trial. Am J Sports Med 2014;42:1049-57. [Google Scholar] [PubMed]
- 7. Williams A, Coyle C, Bruno S, et al[tps5.1]. OCT Predicts T2 Change Over 6 and 12 Months in Subjects with Early Articular Cartilage Degeneration. 57th Annual Meeting of the Orthopaedic Research Society. Long Beach CA; 2011. p. 96. [Google Scholar] [PubMed]
- 8. Chu CR, Williams A, Tolliver D, Kwoh CK, Bruno S 3rd, Irrgang JJ. Clinical optical coherence tomography of early articular cartilage degeneration in patients with degenerative meniscal tears. Arthritis Rheum 2010;62:1412-20. [Google Scholar] [PubMed]
- 9. Price JS, Till SH, Bickerstaff DR, Bayliss MT, Hollander AP. Degradation of cartilage type II collagen precedes the onset of osteoarthritis following anterior cruciate ligament rupture. Arthritis Rheum 1999;42:2390-8. [Google Scholar] [PubMed]
- 10. David-Vaudey E, Ghosh S, Ries M, Majumdar S. T2 relaxation time measurements in osteoarthritis. Magn Reson Imaging 2004;22:673-82. [Google Scholar] [PubMed]
- 11. Goodwin DW, Wadghiri YZ, Zhu H, Vinton CJ, Smith ED, Dunn JF. Macroscopic structure of articular cartilage of the tibial plateau: Influence of a characteristic matrix architecture on MRI appearance. AJR Am J Roentgenol 2004;182:311-8. [Google Scholar] [PubMed]
- 12. Liess C, Lusse S, Karger N, Heller M, Glüer CC. Detection of changes in cartilage water content using MRI T2-mapping in vivo. Osteoarthritis Cartilage 2002;10:907-13. [Google Scholar] [PubMed]
- 13. Mosher TJ, Dardzinski BJ, Smith MB. Human articular cartilage: influence of aging and early symptomatic degeneration on the spatial variation of T2–preliminary findings at 3 T. Radiology 2000;214:259-66. [Google Scholar] [PubMed]
- 14. Williams A, Winalski CS, Chu CR. Early articular cartilage MRI T2 changes after anterior cruciate ligament reconstruction correlate with later changes in T2 and cartilage thickness. J Orthop Res 2017;35:699-706. [Google Scholar] [PubMed]
- 15. Osaki K, Okazaki K, Takayama Y, Matsubara H, Kuwashima U, Murakami K, et al. Characterization of biochemical cartilage change after anterior cruciate ligament injury using T1ρ mapping magnetic resonance imaging. Orthop J Sports Med 2015;3:2325967115585092[tps6.1]. [Google Scholar] [PubMed]
- 16. Hirose J, Nishioka H, Okamoto N, Oniki Y, Nakamura E, Yamashita Y, et al. Articular cartilage lesions increase early cartilage degeneration in knees treated by anterior cruciate ligament reconstruction: T1ρ mapping evaluation and 1-year follow-up. Am J Sports Med 2013;41:2353-61. [Google Scholar] [PubMed]
- 17. Nishioka H, Hirose J, Nakamura E, Okamoto N, Karasugi T, Taniwaki T, et al. Detecting ICRS grade 1 cartilage lesions in anterior cruciate ligament injury using T1ρ and T2 mapping. Eur J Radiol 2013;82:1499-505. [Google Scholar] [PubMed]
- 18. Knox J, Pedoia V, Wang A, Tanaka M, Joseph GB, Neumann J, et al. Longitudinal changes in MR T1ρ/T2 signal of meniscus and its association with cartilage T1p/T2 in ACL-injured patients. Osteoarthritis Cartilage 2018;26:689-96. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 MRI–Histopathology Correlation of Cartilage and Bone in Early Knee Osteoarthritis
December 1, 2025 MRI–Histopathology Correlation of Cartilage and Bone in Early Knee Osteoarthritis August 6, 2024 A Comparative Study on Correlation between Magnetic Resonance Imaging and Arthroscopic Findings in the Knee Joint Injuries
August 6, 2024 A Comparative Study on Correlation between Magnetic Resonance Imaging and Arthroscopic Findings in the Knee Joint Injuries December 10, 2022 Bosworth Ankle Injuries – Treatment Challenges in Late and Neglected Presentations
December 10, 2022 Bosworth Ankle Injuries – Treatment Challenges in Late and Neglected Presentations January 28, 2015 Plagiarism- Cut it at the roots
January 28, 2015 Plagiarism- Cut it at the roots