
Anterior iliac crest for bone graft harvesting with an open technique appears to be a safe procedure with low long-term donor site morbidity from the patients’ perspective when performed/supervised by an experienced surgical team in a tertiary-care teaching hospital. Level of Study: Level IV, Retrospective study.
Dr. Bhaskar Borgohain, Department of Orthopaedics and Trauma, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong - 793018, Meghalaya, India. E-mail: bhaskarprofessor@gmail.com
Abstract
Introduction: In orthopaedic practice, autologous bone grafts are routinely employed to aid fracture healing in non-unions. The anterior iliac crest (AIC) is readily accessible and a standard harvesting site in adults, yielding a generous quantity of bone grafts. Although autologous bone graft remains the gold standard, harvesting graft from the AIC may potentially risk donor site morbidity that is highlighted, especially in the western literature. Our objective in this study was to explore the quantum of donor site morbidity after harvesting AIC bone graft for various reconstructive orthopaedic surgeries.
Materials and Methods: A total of 44 patients of autologous AIC bone graft procedure for various reconstructive orthopedic surgeries (with an average follow-up of 3 years) were evaluated retrospectively on a 9-point retrospective questionnaire response to understand the extent of morbidity.
Results: Early post-operative pain at the donor site was reported by 19 patients, but the highest level of pain was only 3/10 in the Visual Analogue Scale (VAS). There was no major postoperative wound complication at the donor site (both as per file records/discharge paper and/or patient recollection). Only two patients experienced pain that lasted beyond 1 week. After stitch removal, the average pain in VAS reported was as low as 0.8, and none complained of any residual pain at the final follow-up. Only two patients experienced persistent paraesthesia at the donor site.
Conclusion: In our hands, AIC for bone graft harvesting was a safe and effective procedure with low donor site morbidity. This low morbidity appears to be due to multiple factors: (1) low volume of work compared to high volume/high turnover centres; (2) bone graft harvesting done by surgeons not below the rank of senior resident; (3) informed awareness in the surgical team about potential graft site morbidity; (4) adjunct local anaesthetic infiltration/post-operative regional block and pre-emptive analgesia.
Keywords: Anterior iliac crest graft, bone graft, donor area, morbidity, paresthesia, complications, orthopedics.
The problem of fracture site non-unions in some fractures is universal despite advances in our understanding of fracture biology, biomechanics, and surgical techniques. Autologous bone grafts are commonly used to promote fracture union during difficult and redo osteosynthesis. The anterior iliac crest (AIC) is the preferred harvest site due to the simplicity in harvesting (most surgeries are performed in the supine position) and the quantity and quality of bone graft obtainable. Being autogenous, it is non-immunogenic and tends to incorporate well into host bone (when compared to artificial bone grafts), being inherently both osteoconductive and osteoinductive [1]. The morbidity associated with harvesting iliac bone graft (IBG) in adults is well documented [2,3]. The potential complications of bone graft harvesting are bleeding, haematoma, pelvic fractures, nerve damage (sensory loss) and infection [4]. Severe and prolonged pain at the iliac crest after graft harvesting is reported [2,3,4]. To circumvent these issues, bone graft substitutes are now available. However, their lack of osteoinductivity, additional cost and risk of infection (being synthetic foreign materials) are currently the major concerns [5,6].
We conducted a retrospective study involving all patients of AIC bone graft harvesting (as part of their orthopaedic surgical treatment) between April 2010 and December 2015. All procedures were performed in compliance with institutional guidelines and with due approval by the appropriate institutional committee(s) vide Reference no. P87/19/87 vide letter no. NEIGR/IEC/M8/F9/19. We did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The aim was to assess donor site morbidities after harvesting of AIC bone graft in the department of orthopedics of a regional tertiary care teaching institute of India. The patients were identified from the operative records of the department of Orthopedics. All patients received pre-emptive intravenous paracetamol and adjunct local anesthetic infiltration/post-operative continuous regional block, and standard the World Health Organization (WHO) step ladder pattern of analgesia protocol after surgery was used as per pre-existing departmental pain control protocol. Only adults and adolescents (15 years and above) who have had bone graft obtained from the AIC were included in the study. These patients were then invited to answer a predefined questionnaire. The study was based on the retrospective 9-point retrospective questionnaire response as proposed by Pollock et al. [7]. The questionnaire was duly validated by a panel of experts with face validity and content validity, with an acceptable content validity index limit (0.8). The Visual Analog Scale (VAS) score records of the immediate post-operative period were included as well. All Patients were assessed retrospectively for complications (bone graft site morbidity at AIC) using the self-administered questionnaire which consisted of nine questions about (1) Pain at donor site and its effect on functions, (2) complications due to donor site surgery and (3) satisfaction with scar appearance, (4) a global outcome question at the end to understand the overall satisfaction/complications with bone graft harvesting. Demographic characteristics, harvest site confirmation, surgical indication for bone grafting, and any complications after surgery were also recorded. The participants were specifically asked about their post-operative pain, sensory disturbances like paresthesia, functional limitations, and cosmetic appearance of their scar, etc., in respect to the graft harvesting site.
A total of 44 adults and adolescents (15 years or above) underwent AIC bone graft harvesting in this 5-year period. Retrospective questionnaire feedback from all 44 patients was obtained over a period of 4 weeks. There were 28 males and 16 females, the mean age at surgery 35.7 years (range 15–64 years). Out of 44 patients, 32 patients underwent operation for non-union of the lower limb fractures, while 22 patients for the upper limb non-unions. The average follow-up period was 3 years. The results were summarised in a table and figures for clarity in Table 1 and Fig. 1, respectively.
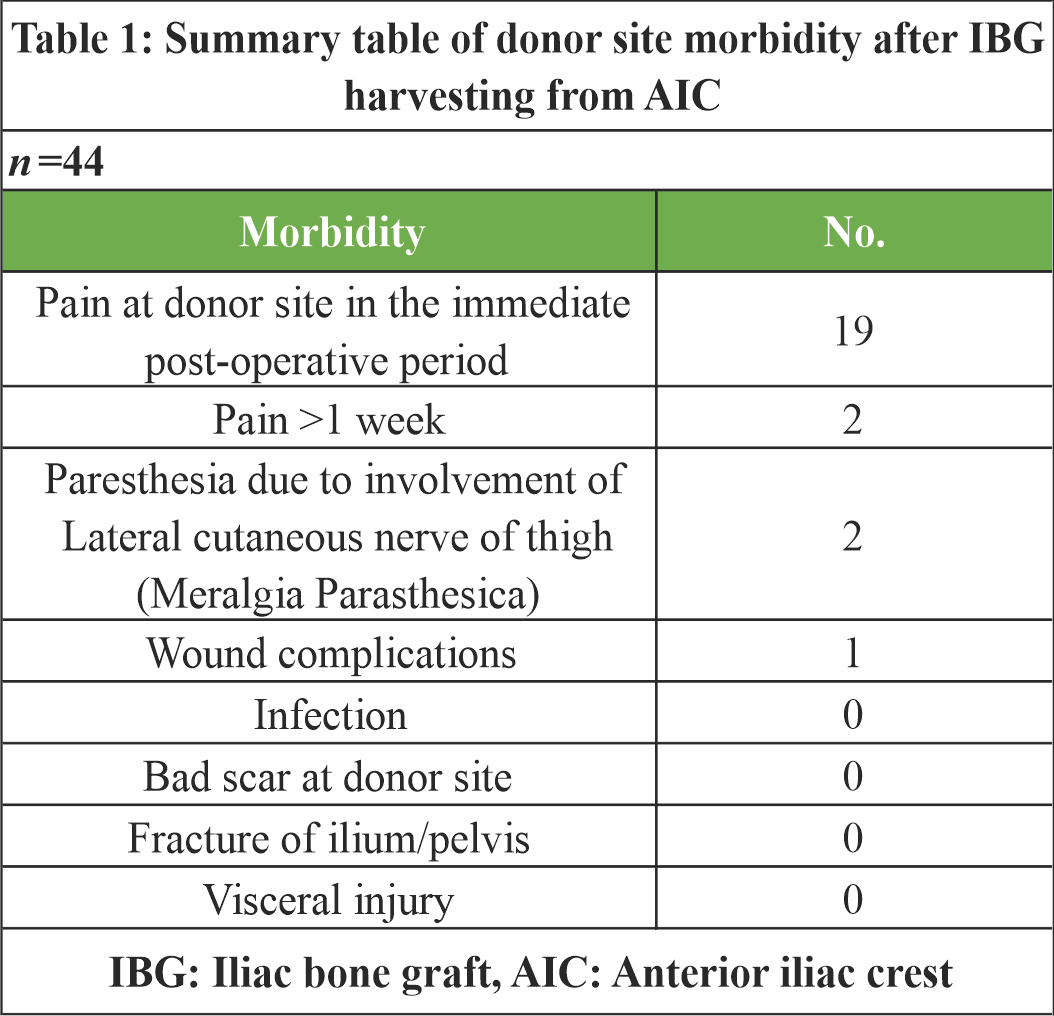
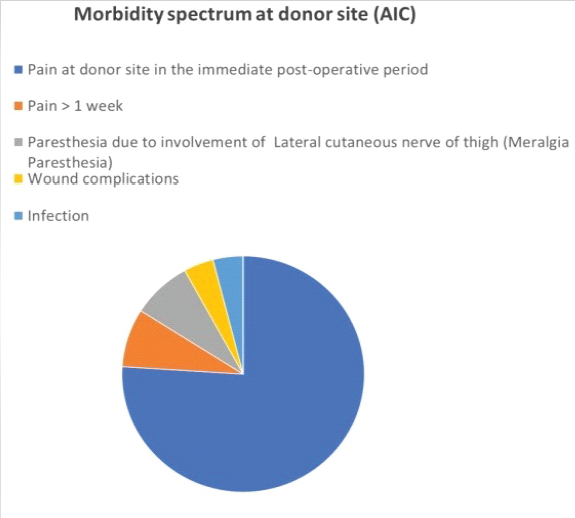
Figure 1: Distribution of Donor-site Morbidity
Early post-operative pain at the donor site was reported by 19 out of 44 patients (43.2%), and of these, only two (4.5%) patients experienced pain that lasted for more than a week. A VAS was used to measure the intensity of pain. After stitch removal, the average pain in VAS retrospectively was below 2. One patient had a minor wound complication without any sequalae. None complained of any residual pain at the final follow-up. Only two patients (Both were females) reported a VAS score above 3 until stitch removal. Patients who were operated on their lower extremities did require some form of walking aid (axillary crutches, frame walkers) for a period of at least 6 weeks due to restrictions on full weight bearing and not due to pain from the graft donor site. There were no major post-operative wound complications at the donor site. Apart from paresthesia at the donor site reported by two patients (4.5%), no major post-operative wound complications were reported from the AIC donor site. All patients were satisfied with the scar, and none had any identifiable functional limitations related to the harvest site at final follow up.
We tried to understand the extent of donor site morbidity in patients (a rather homogeneous group of adults and adolescents above 15 years of age, all having limb bone non-unions after fractures) after AIC bone graft harvesting. Although AIC is both popular and preferred as a source of autogenous bone graft donor site and is generally considered safe, nevertheless, morbidity and complications are not unreal. The reported incidence of such complications after iliac crest bone graft harvesting ranges from 2% to 39%, pain at the donor site being the most frequent among them [1,8]. Other known complications include fractures, neurovascular injury, urethral injury, infections, herniation of abdominal contents, pelvic instability, cosmetic defects, hematomas, and tumor transplantation [9]. Fortunately, major complications are uncommon (tend to resolve with appropriate management), and minor complications may continue for months to years [2]. Pollock et al. reported donor site pain (experienced by 62% of their patients) as the commonest complication lasting <6 weeks [7]. The reported incidence of temporary pain varied [10] from 2.8% to 17%. Chronic pain after graft harvesting was reported [11] in 29% of their patients. Several hypotheses exist to explain the origin of such post-harvest pain; the precise cause, however, remains unclear. It could be due to nerve injury or disruption of the musculature during graft harvesting [12]. Goulet et al., reported pain in 37.9% of their patients at 6-month follow-up, with persistent pain in 18.3% of them even at 2 years [2]. In our study too, 19 (43.2%) patients reported early post-operative pain at the donor site following surgery, but only two patients had pain lasting more than a week. It may be mentioned that the previous studies apply to bone grafts taken from the posterior iliac crest for spine surgeries, where the gluteal muscles are released from the iliac crest. Nerve injury is not an uncommon complication during iliac crest graft harvesting [4]. Several sensory nerves are known to be inherently at risk. The lateral cutaneous nerve of the thigh is vulnerable during harvesting the AIC [13]. The superior cluneal nerves are at risk during harvesting of the posterior iliac crest [14]. If injured, the typical neurogenic symptoms include pain, tingling, numbness, and paraesthesia along the distribution of the injured nerve. All patients were clinically examined for checking sensation along the lateral cutaneous nerve of the thigh – only two patients in our study had chronic altered sensation at the donor site. Knowledge about the anatomy of the lateral cutaneous nerve of the thigh and its common variations seems to be important to avoid injuries. None had infection, vascular injury, haematoma, extensive bruising, scar numbness, fracture, or chronic pain in our study. The reported rate of minor complications (resolve without any intervention) is between 10% and 40%. Minor complications reported are superficial infection, haematoma, and temporary paraesthesia [1,2,4,10,11,12]. Major complications can be neurologic injury, vascular injury, deep infection, large haematoma, bowel herniation, fracture or pelvic instability with impaired gait [15]. We did not do a radiological evaluation to confirm the absence of any fractures in our study. In a systematic review, Sulistyani et al. [16] reported lower complications after fibular bone graft harvesting and reported a high complication rate after iliac bone graft (IBG), irrespective of the size of the bone graft harvested or the age of the donor (without major comorbidities) for all non-vascularised bone graft harvesting. However, Brandenburg et al. [17] in their study reported that the graft volume and length of scar do have a significant effect on the extent of donor site morbidity (including neurogenic pain) in vascularised IBG harvesting donor site. Schott et al. [18] reported (in a single-centre study with a small sample size) lower than anticipated morbidity in paediatric patients of IBG, except donor site pain lasting up to 30 days after harvesting. Lopez et al. [19], Bernstein et al. [20] and Missiuna et al. [21] even suggested avoiding open techniques and consider minimally invasive techniques (e.g. bone grinder and trephine technique, transcrestal technique, etc.) of graft harvesting to reduce the extent of post-operative pain, need for walker support and length of hospital stay. The limitations of our study are its small sample size and lack of a control arm for comparison. However, the participation of all 44 patients represented 100% of patients from this institute who underwent bone grafting during this specific period, adding to the strength of the study. Being a single-centre study, external validity may be limited, but it provides a snapshot of graft site morbidity. Absence of a control group reduces the value of this study; however, currently, there is a lack of any published work in this area from this region. Future work should consider registered clinical trials to compare various techniques (open and minimally invasive techniques of bone graft harvesting). The validated questionnaire adapted from Pollock et al. [7] is not a subjective evaluation but can be considered analogous to a patient-reported outcome measurement tool and quality of life; it was previously used for the same study objectives in patients undergoing spinal fusions. Questionnaire has the ability to measure quality of life, such as WHOQOL-BREF – a 26-item self-report measure for adults to assess self-perceived quality of life [22]. Another drawback is the retrospective nature of our study with the possibility of bias concerning the patients’ ability to clearly recall the past level of pain and minor complications during their post-operative pain, that too after an average follow-up of 3 years, and thus limits the ability to establish a clear causal relationship. However, each participant was clinically examined as a part of the evaluation for a comprehensive assessment of possible residual complications of graft harvesting to fill up the gap in information. Observer and interviewer bias was minimised by standardising the process of collecting participants’ responses and cross-checking by a panel. Being a retrospective study, it was not possible to correlate the quantity of bone graft harvested with donor site morbidity. While interpreting the findings of our study, the limitations of a retrospective design, single-centre study and small sample size, and the possibility of selection bias – all may be taken into consideration.
With short-lived post-operative pain and a low frequency of complications after harvesting of AIC bone grafts for various orthopaedic procedures, we found that the AIC remains a safe site for bone graft harvesting in adolescent and adult patients. There was no significant long-term morbidity associated with well-performed open AIC graft harvesting when performed/supervised by trained surgeons in the setting of elective surgeries in a teaching hospital. Inadvertent injury to the lateral cutaneous nerve of the thigh during this procedure appears to be the primary concern that may add to long-term morbidity. In our hands (single-centre study with small sample size), AIC for bone graft harvesting with an open technique was a safe and effective procedure with low donor site morbidity. This low morbidity appears to be due to multiple factors: (1) low volume of work compared to high volume/high turnover centres, (2) bone graft harvesting done by a surgeon not below the rank of senior resident, (3) informed awareness in the surgical team about graft site morbidity, (4) adjunct local anaesthetic infiltration/post-operative continuous regional block, and (5) application of the standard WHO step ladder pattern of analgesia protocol after surgery. While interpreting the findings of our study, the limitations of a retrospective design, single-centre study, and small sample size, and the possibility of selection bias – all may be taken into consideration.
In this single-center, retrospective, patient-reported study, open AIC graft harvesting was found to be a safe procedure, with low donor site morbidity when performed in a tertiary care set up. Familiarity of the procedure by an experienced tertiary-care team, team awareness about potential donor-site morbidity and good perioperative analgesia may have contributed to low donor site morbidity.
References
- 1. Arrington ED, Smith WJ, Chambers HG, Bucknell AL, Davino NA. Complications of iliac crest bone graft harvesting. Clin Orthop 1996;329:300-9. [Google Scholar] [PubMed]
- 2. Goulet JA, Senunas LE, DeSilva GL, Greenfield ML. Autogenous iliac crest bone graft. Complications and functional assessment. Clin Orthop 1997;339:76-81. [Google Scholar] [PubMed]
- 3. Dimitriou R, Mataliotakis GI, Angoules AG, Kanakaris NK, Giannoudis PV. Complications following autologous bone graft harvesting from the iliac crest and using the RIA: A systematic review. Injury 2011;42:S3-15. [Google Scholar] [PubMed]
- 4. Banwart JC, Asher MA, Hassanein RS. Iliac crest bone graft harvest donor site morbidity. A statistical evaluation. Spine 1995;20:1055-60. [Google Scholar] [PubMed]
- 5. Nandi SK, Roy S, Mukherjee P, Kundu B, De DK, Basu D. Orthopaedic applications of bone graft & graft substitutes: A review. Indian J Med Res 2010;132:15-30. [Google Scholar] [PubMed]
- 6. Virk S, Sandhu HS, Khan SN. Cost effectiveness analysis of graft options in spinal fusion surgery using a Markov model. J Spinal Disord Tech 2012;25:E204-10. [Google Scholar] [PubMed]
- 7. Pollock R, Alcelik I, Bhatia C, Chuter G, Lingutla K, Budithi C, et al. Donor site morbidity following iliac crest bone harvesting for cervical fusion: A comparison between minimally invasive and open techniques. Eur Spine J 2008;17:845-52. [Google Scholar] [PubMed]
- 8. Fowler BL, Dall BE, Rowe DE. Complications associated with harvesting autogenous iliac bone graft. Am J Orthop ( Belle Mead NJ) 1995;24:895-903. [Google Scholar] [PubMed]
- 9. Seiler JG 3rd, Johnson J. Iliac crest autogenous bone grafting: Donor site complications. J South Orthop Assoc 2000;9:91-7. [Google Scholar] [PubMed]
- 10. Schnee CL, Freese A, Weil RJ, Marcotte PJ. Analysis of harvest morbidity and radiographic outcome using autograft for anterior cervical fusion. Spine (Phila Pa 1976) 1997;22:2222-7. [Google Scholar] [PubMed]
- 11. Fernyhough JC, Schimandle JJ, Weigel MC, Edwards CC, Levine AM. Chronic donor site pain complicating bone graft harvesting from the posterior iliac crest for spinal fusion. Spine 1992;17:1474-80. [Google Scholar] [PubMed]
- 12. Kurz LT, Garfin SR, Booth RE Jr. Harvesting autogenous iliac bone grafts. A review of complications and techniques. Spine 1989;14:1324-31. [Google Scholar] [PubMed]
- 13. Kargel J, Dimas V, Tanaka W, Robertson OB, Coy JM, Gotcher J, et al. Femoral nerve palsy as a complication of anterior iliac crest bone harvest: Report of two cases and review of the literature. Can J Plast Surg 2006;14:239-42. [Google Scholar] [PubMed]
- 14. Lu J, Ebraheim NA, Huntoon M, Heck BE, Yeasting RA. Anatomic considerations of superior cluneal nerve at posterior iliac crest region. Clin Orthop 1998;347:224-8. [Google Scholar] [PubMed]
- 15. Shin SR, Tornetta P 3rd. Donor site morbidity after anterior iliac bone graft harvesting. J Orthop Trauma 2016;30:340-3. [Google Scholar] [PubMed]
- 16. Sulistyani LD, Julia V, Rizki TZ, Dharmawan DK. Donor site morbidity of nonvascularized bone graft: A systematic review. Pesqui Bras Odontop Clín Integr 2023;23:e220029. [Google Scholar] [PubMed]
- 17. Brandenburg LS, Voss PJ, Mischkowsky T, Kühle J, Ermer MA, Weingart JV, et al. Donor site morbidity after computer assisted surgical reconstruction of the mandible using deep circumflex iliac artery grafts: A cross-sectional study. BMC Surg 2023;23:4. [Google Scholar] [PubMed]
- 18. Schott T, Eisenberg KA, Vuillermin CB, Bae DS, Waters PM, Bauer AS. Donor-site morbidity for iliac crest harvesting for pediatric scaphoid nonunion. J Hand Surg 2023;48:833.e1-5. [Google Scholar] [PubMed]
- 19. Lopez GD, Hijji FY, Narain AS, Yom KH, Singh K. Iliac crest bone graft: A minimally invasive harvesting technique. Clin Spine Surg 2017;30:439-41. [Google Scholar] [PubMed]
- 20. Burstein FD, Simms C, Cohen SR, Work F, Paschal M. Iliac crest bone graft harvesting techniques: A comparison. Plast Reconstr Surg 2000;105:34-9. [Google Scholar] [PubMed]
- 21. Missiuna PC, Gandhi HS, Farrokhyar F, Harnett BE, Dore EM, Roberts B. Anatomically safe and minimally invasive transcrestal technique for procurement of autogenous cancellous bone graft from the mid-iliac crest. Can J Surg 2011;54:327-32. [Google Scholar] [PubMed]
- 22. Wong FY, Yang L, Yuen JW, Chang KK, Wong FK. Assessing quality of life using WHOQOL-BREF: A cross-sectional study on the association between quality of life and neighborhood environmental satisfaction, and the mediating effect of health-related behaviors. BMC Public Health 2018;18:1113. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report
July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report June 1, 2026 A Rare Case of Giant Cell Tumor of the First Metatarsal: En Bloc Resection and Fibular Autograft Reconstruction
June 1, 2026 A Rare Case of Giant Cell Tumor of the First Metatarsal: En Bloc Resection and Fibular Autograft Reconstruction January 1, 2026 Successful Management of a 40-Year-Old Non-union of the Humeral Shaft with Pseudoarthrosis with Plate Fixation and Bone Grafting: A Case Report
January 1, 2026 Successful Management of a 40-Year-Old Non-union of the Humeral Shaft with Pseudoarthrosis with Plate Fixation and Bone Grafting: A Case Report December 1, 2025 Novel Technique for Extracting Metallic Debris from a Broken Reamer-Irrigator-Aspirator-2 Head within the Intramedullary Canal
December 1, 2025 Novel Technique for Extracting Metallic Debris from a Broken Reamer-Irrigator-Aspirator-2 Head within the Intramedullary Canal