
Age-related changes of cervical digit suggested it may represent a heterogeneous group of anomalies related to progressive cervical malsegmentation.
Dr. Gakuto Ujiie, Department of Pediatrics, Showa Medical University School of Medicine, 1-5-8 Hatanodai, Shinagawa, Tokyo 142-8666, Japan. E-mail: g.ujiie@med.showa-u.ac.jp
Abstract
Introduction: A cervical digit is an extremely rare congenital anomaly and an isolated, benign condition. This report describes the age-related evolution of a cervical digit (digit-like bone posterior to the cervical spine) accompanied by malsegmentation of the cervical spine.
Case Report: This is a follow-up study of a female infant with a cervical digit whose findings had been reported previously. The digit-like bone was articulated with the right posterior neural arch at C5. In addition, the right neural arches of C4, C5, and C6 were malsegmented. She was asymptomatic during her infancy; however, she slowly developed progressive restriction of neck movement beginning at 3 years of age. During her clinical course, she underwent three-dimensional computed tomography (CT) at ages 3 and 7 years, which revealed age-dependent morphological evolution of the malformation. CT demonstrated progressive ankylosis of the bilateral posterior arches of C4, C5, and C6. The cervical digit coalesced with the posterior neural arch at C5 and manifested as a bulky spinous process.
Conclusion: The morphological outcome was atypical compared with the typical manifestation of cervical digits, that is, only a supernumerary bone longitudinally orientated posterior to or attached to the spinous process.
Keywords: Cervical digit, anomalous spinous process, age-dependent evolution, segmental anomalies, Klippel-Feil sequence.
A congenital digit-like bone located posterior to the cervical spine, occasionally termed the cervical digit, is an extremely rare anomaly [1,2,3,4,5,6]. Nakano et al. reported the imaging findings of a female infant with a cervical digit, which were accompanied by abnormal segmentation of the adjoining neural arches [1]. She underwent three-dimensional computed tomography (3D-CT) at the ages of 3 and 7 years, which revealed morphological changes in the malformation over time. This report describes the age-related atypical evolution of this structure using imaging techniques.
The girl was born with a hard projection from the posterior neck. A 3D-CT revealed a digit-like structure attached to the lamina of C5, associated with malsegmentation of the right posterior arches of C4-C5-C6 (hypoplasia of C4 and fusion between C5 and C6) [1]. She was asymptomatic during infancy and early childhood. At 3 years of age, restriction of neck movement was noted, which progressed slowly thereafter. Neurological examination remained normal; she had no pain, and management consisted of clinical and radiological follow-up without surgery. A 3D-CT performed at 3 and 7 years of age revealed progressive ankylosis of the bilateral posterior arches of C4, C5, and C6, complete ankylosis on the right side, and incomplete fusion on the left side. Digit-like bone projections coalesced with the posterior neural arch of C5 and appeared as spinous process-like bulky bone projections (Figs. 1 and 2). Axial computed tomography images taken at 7 years of age excluded spinal canal stenosis at poorly segmented levels (Fig. 3).
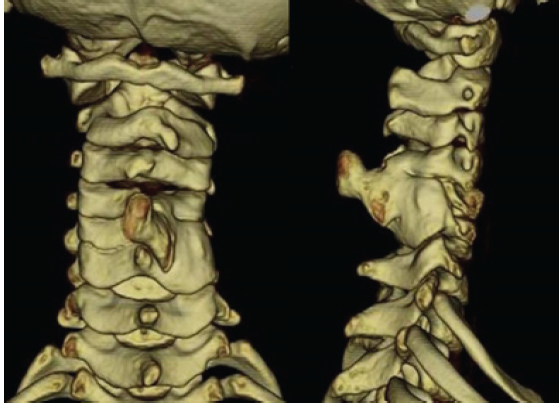
Figure 1: The three-dimensional computed tomography performed at the age of 3 years reveals progressive fusion in the posterior arches of vertebrae at C4–6 levels, together with deformed digit-like bone.
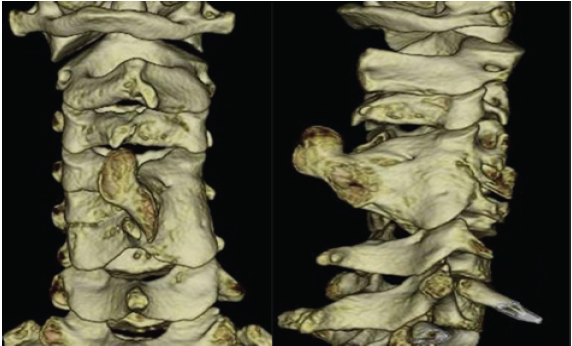
Figure 2: The three-dimensional computed tomography, performed at the age of 7 years, reveals overt ankylosis of the posterior arches of C4, C5, and C6, and the cervical digit evolves into a bulky bone projection contiguous with the right posterior arch of C4 and C5, mimicking a spinous process.

Figure 3: Axial view of the computed tomography, performed at the age of 7 years, indicates that the spinal canal is normal.
The progression observed in this case, from a congenital digit-like bone attached to the cervical vertebrae to a hyperplastic spinous bone, differs from what is seen in most cases of cervical digits. In these cases, the condition typically manifests as supernumerary digit- or phalanx-like bone(s) that retain their morphological characteristics from birth to adulthood [2,3,4,5,6]. In contrast, the final manifestations observed in our patient resembled those found in patients with an anomalous spinous process or a posterior neural arch [7,8,9,10,11]. As observed in the present case, although an anomalous or hyperplastic projection from the spinous process or neural arch is not completely ossified, bone protrusion may be confused with a typical cervical digit (a supernumerary bone posterior to the cervical spine). Thus, we would like to term such cases with a malformed projection of the neural arch “atypical cervical digit”. Table 1 summarises previous reports on typical and atypical cervical digits.
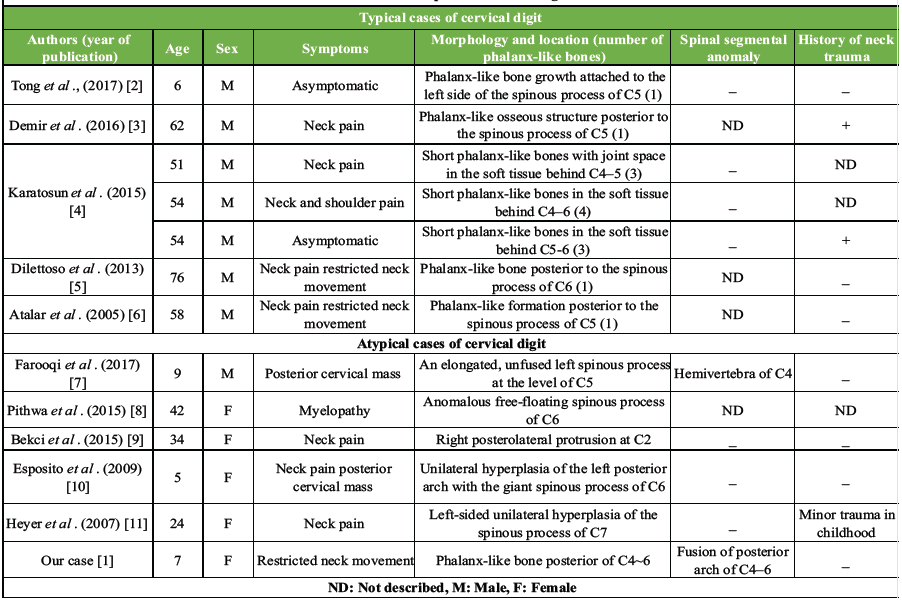
Table 1: Case reports of cervical digit
The association with ankylosis or malsegmentation of the posterior neural arches observed in the present case may be unique compared to the manifestation of atypical cases with cervical digits. Most cases of atypical cervical digits show only morphological aberrations of the posterior neural arch. There was only one documented case of an atypical cervical digit associated with spinal malsegmentation; however, a 9-year-old boy showed an elongated spinous process of C5, accompanied by a hemivertebra of C4 in a previous report [7]. In the present case, malsegmentation of the anterior spinal component differed from that of the posterior neural arch. From a developmental perspective, the present case is classified under the broad category of Klippel–Feil syndrome, which is characterised by congenital fusion of two or more cervical vertebrae [12,13].
The present case represents a rare congenital anomaly characterised by a digit-like bone arising from the cervical spine and progressive hyperplasia of the posterior neural arch. This uncommon association can manifest as atypical cervical digits. It is tempting to consider the cervical digit as a heterogeneous group of anomalies, with malsegmentation of the cervical spine being one subgroup within this category.
A cervical digit as a congenital anomaly may change with ageing, such as atypical evolution of its structure and progressive cervical malsegmentation.
References
- 1. Nakano Y, Aizawa M, Kako Y, Mizuno K, Itabashi K, Nishimura G.A neonate with an anomalous bone attached to the cervical spine. Spine J2013;13:e5-7. [Google Scholar] [PubMed]
- 2. TongMJ, XiangGH, HeZL, Xu HZ, Tian NF.Cervical digit in a child: A case report. Med (Baltimore)2017;96:e9348. [Google Scholar] [PubMed]
- 3. Demir MK, Yılmaz B, Toktaş ZO, Akakın A, Eksi MS, Konya D.Cervical digit: A rare developmental anomaly. Spine J2016;16:e295-6. [Google Scholar] [PubMed]
- 4. Karatosun V, Özaksoy D, Balcı A, Günal İ.Cervical digits: A report of 3 cases. Acta Orthop Traumatol Turc2015;49:453-5. [Google Scholar] [PubMed]
- 5. Dilettoso S, Uccello A, Dilettoso A, Dilettoso B, Uccello M.Supernumerary phalanx-like bone formation posterior to C6 spinous process. Spine J2013;13:587. [Google Scholar] [PubMed]
- 6. Atalar H, Yavuz OY, Doğruel H, Catal SA, Sayli U.Phalanx-like osseous structure posterior to the cervical vertebrae: A hitherto unreported location for a rare anomaly. Acta Orthop Traumatol Turc2005;39:361-4. [Google Scholar] [PubMed]
- 7. Farooqi RR, Mehmood M, Kotwal HA. Hyperplasia of lamina and spinous process of C5 vertebrae and associated hemivertebrae at C4 level. J Orthop Case Rep2017;7:79-81. [Google Scholar] [PubMed]
- 8. Pithwa YK. Anomalous cervical spinous process leading to myelopathy. Spine (Phila Pa 1976) 2015;40:E1117-9. [Google Scholar] [PubMed]
- 9. Bekci T, Aslan K, Gunbey HP, Turgut E, Incesu L.A rare cause of chronic neck pain: accessory cervical spinous process. Spine J2015;15:e15-6. [Google Scholar] [PubMed]
- 10. Esposito G, De Bonis P, Tamburrini G, Massimi L, Byvaltsev V, Di Rocco C,et al. Unilateral hyperplasia of the left posterior arch and associated vertebral schisis at C6 level. Skelet Radiol 2009;38:1191-5. [Google Scholar] [PubMed]
- 11. Heyer CM, Nicolas V, Peters SA.Unilateral hyperplasia of a cervical spinous process as a rare congenital variant of the spine. ClinImaging2007;31:434-6. [Google Scholar] [PubMed]
- 12. Samartzis DD, Herman J, Lubicky JP, Shen FH.Classification of congenitally fused cervical patterns: Epidemiology and role in the development of cervical spine-related symptoms. Spine2006;31:E798-804. [Google Scholar] [PubMed]
- 13. Guille JT, Miller A, Bowen JR, Forlin E, Caro PA.The natural history of Klippel-Feil syndrome: clinical, roentgenographic, and magnetic resonance imaging findings at adulthood. J Pediatr Orthop1995;15:617-26. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 October 10, 2022 Ochronotic hip arthropathy – A case report
October 10, 2022 Ochronotic hip arthropathy – A case report April 10, 2016 Short stature Revealing a Pycnodysostosis: A Case Report
April 10, 2016 Short stature Revealing a Pycnodysostosis: A Case Report January 1, 2025 Re-arthroscopic Findings 18 Years After Osteochondral Autologous Transplantation for Cartilage Lesion in the Knee: A Case Report
January 1, 2025 Re-arthroscopic Findings 18 Years After Osteochondral Autologous Transplantation for Cartilage Lesion in the Knee: A Case Report September 1, 2025 A Rare Case of Septic Arthritis of the Knee Associated with Pathological Neck of Femur Fracture Caused by Serratia Marcescens – A Case Report
September 1, 2025 A Rare Case of Septic Arthritis of the Knee Associated with Pathological Neck of Femur Fracture Caused by Serratia Marcescens – A Case Report