
Hip dislocation in late-onset methylmalonic acidemia is driven by dystonia rather than a static mechanical defect, which requires a dual-target approach by pairing definitive surgical management with aggressive neurological-directed medical therapy to fight the dynamic muscular forces which seem to be the biggest threat in this disease.
Dr C Sitsabesan, Department of Orthopaedic Surgery, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India. E-mail: sabesan101@gmail.com
Abstract
Introduction: Hip dislocation is a rare secondary complication due to neuromuscular dysfunction in organic acid disorders like methylmalonic acidemia (MMA). Surgical intervention in patients with metabolically driven basal ganglia lesions presents unique challenges for both physiological stability and mechanical success.
Case Report: An 11-year-old boy with late-onset MMA presented with generalised spasticity, involuntary movements, and a left hip deformity in flexion, adduction, and internal rotation. Imaging confirmed a left hip dislocation associated with coxa valga and caput valga. The patient was managed initially with muscle relaxants followed by surgical intervention consisting of a closed reduction, proximal femoral varus osteotomy, adductor tenotomy and a medial femoral caput epiphysiodesis. Post-operative management utilised an abduction brace; however, persistent spasticity created significant challenges in maintaining hip stability and compliance with the orthosis. Conclusion: Surgical management of hip dislocation in MMA requires addressing both the bony deformity and the underlying neuromuscular forces. While anatomical reduction is achievable, aggressive management of spasticity is critical to prevent recurrence in the acute post-operative period.
Conclusion: Methylmalonic acidemia, organic acid disorders, neuromuscular hip dislocation, coxa valga, caput valga, proximal femoral varus osteotomy.
Organic acid disorders (OADs) are a subset of inborn errors of metabolism that result in a toxic accumulation of organic acids in the body, which can lead to metabolic derangements and encephalopathies. Globally, methylmalonic acidemia (MMA) is a rare autosomal recessive disease with a birth prevalence of approximately 1.14/100,000 live births [1]. In India, its prevalence is 1.3–2.0 cases/100,000 live births, accounting for 20–40% of all organic acidemias [2]. MMA is a rare autosomal recessive metabolic disease. Methylmalonic acid is a breakdown product of essential amino acids such as isoleucine, methionine, valine and threonine. It is caused by a methylmalonyl-CoA mutase or cobalamin (Cbl, also known as vitamin B12) deficiency [3]. This cobalamin deficiency subtype has a better prognosis, as it may be responsive to hydroxocobalamin supplementation. These deficiencies lead to the accumulation of methylmalonic acid, which inhibits succinyl CoA formation and, hence, energy production in the Krebs cycle, leading to a cellular energy crisis. The resulting toxic buildup impairs renal function, causing chronic kidney failure, and can permanently damage the basal ganglia, leading to intellectual disability, dystonia and growth retardation. Late-onset MMA is a milder form of the disease where the child may remain asymptomatic until a triggering event causes a “metabolic stroke” which reveals the underlying disorder. Rarely, hip dislocations or subluxations may occur secondarily in disorders like MMA. The spasticity of the adductors and flexors overpower their antagonist muscle groups, leading to progressive dislocation of the hip. These are unlike the sudden, painful traumatic dislocations occurring with adults. A significant gap exists in the literature regarding the perioperative management of orthopaedic complications in children with MMA [4]. This report describes the challenges during perioperative management of hip dislocation secondary to late-onset MMA.
History and physical examination:
An 11-year-old male child presented with difficulty in walking, using his left upper limb, and difficulty in speaking. This patient was healthy till age 9 years, when he had an episode of acute gastroenteritis that triggered the above symptoms. He developed spasticity of both lower limbs (left more than right), the left upper limb, and difficulty speaking. He was diagnosed with an OAD, MMA (cobalamin-responsive type), after a thorough workup including a genetic analysis. Genetic analysis revealed a mutation in the MMAB gene (cblB subtype), confirming cobalamin-responsive MMA. His spasticity was more on the left side and on the lower limb. Initially, a reducible left hip subluxation was treated with an abduction brace. However, recurrent spasticity made this static orthotic brace difficult to wear, leading to dislocation progressively. Birth, antenatal, and family histories were unremarkable. He also struggled to wear the abduction brace due to recurrent episodes of spasticity. This led to recurrent episodes of left hip subluxation. His mother had no comorbidities, and her antenatal period was uneventful. His birth, postnatal and family histories were unremarkable. He is the second-born to non-consanguineous parents. The child had a global developmental delay, which resolved during childhood. On physical examination, the child had a normal sensorium with no intellectual disability. His anthropometric measurements showed that he was less than the third percentile for his height and weight. His higher mental functions were intact, and cranial nerve functions were normal. The tone of all four limbs was increased. The reflexes for his upper and lower limbs were exaggerated bilaterally. The power for his left upper limb was grade three as per MRC grading, while his right upper and lower limbs were grade five. His lower limb power on the left side was grade four. His posture was abnormal, with the left hip flexed, adducted and internally rotated with apparent shortening, giving the impression of a posterior hip dislocation. His left knee was in flexion with his ankle in equinus with a left thumb adduction deformity. All these deformities were not fixed and were due to spasticity, except for the left ankle equinus contracture, which was due to a gastrocnemius contracture predominantly, confirmed by the Silfverskiöld test. There were three centimetres of femoral shortening. He was unable to walk independently and had an abnormal gait. Over this 2-year period, he was under the care of paediatric neurology for medical treatment with muscle relaxants inclusive of diazepam, trihexyphenidyl and baclofen, along with a high dose of hydroxocobalamin due to the disease’s responsiveness to cobalamin. He has also been on a specialised diet which is devoid of propiogenic amino acids.
Diagnostic imaging and preoperative planning:
The current radiographs at the age of 11 years confirmed a neglected posterior left hip dislocation with acetabular dysplasia, coxa valga and caput valga. When the spasm is controlled, radiographs confirmed that the hip could be reduced with passive abduction (Fig. 1). Pre-operative calculation showed the Reimer’s index to be 64% (Fig. 2). Over this 2-year period from the diagnosis, the neck shaft angle of the affected left hip increased from 132° to 142° (Fig. 3). From an orthopaedic perspective, the main issues were the left hip dislocation, the adductor spasm, coxa valga, caput valga and the acetabular dysplasia in a spastic limb.
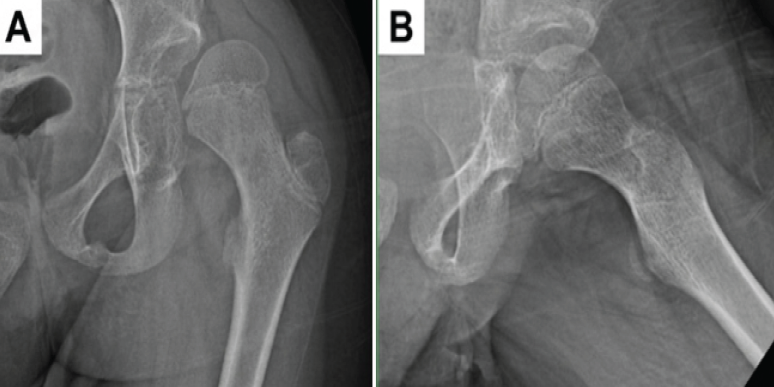
Figure 1: Pre-operative radiographic evaluation of the left hip joint, (a) Anteroposterior pelvic radiograph confirming a neglected posterior left hip dislocation along with coxa valga, caput valga, and acetabular dysplasia, (b) Passive abduction in anteroposterior radiograph demonstrating reduction of the femoral head into the acetabulum when muscular spasticity is controlled.
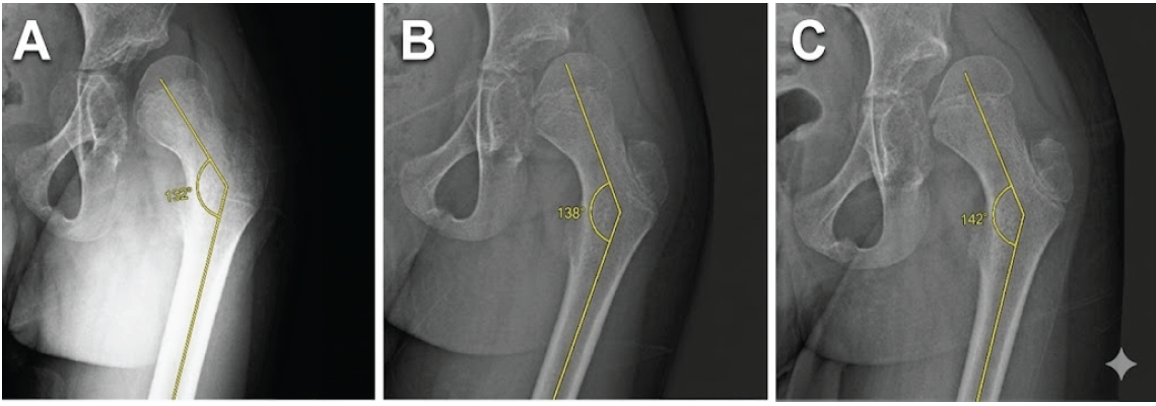
Figure 2: Serial radiographic tracking of the progressive left neck-shaft angle deformity, (a) Radiograph at initial presentation demonstrating a left neck-shaft angle of 132° and hip subluxation, (b) Interval follow-up radiograph showing progression of coxa valga with the neck-shaft angle increasing to 138° driven by neuromuscular spasticity, (c) Pre-operative radiograph at age 11 years confirming severe progression to a neck-shaft angle of 142° associated with a complete, neglected posterior hip dislocation.

Figure 3: Pre-operative measurement of Reimer’s migration index on an anteroposterior pelvic radiograph. Hilgenreiner’s line and Perkins’ line are constructed alongside parallel alignment tracking lines. Measurement of the femoral head width relative to the migrated portion extending beyond Perkins’ line yields a calculated Reimer’s migration index of 64%, confirming left hip dislocation.
Surgical management:
Examination of the hip under general anaesthesia, in the supine position, showed reducibility with abduction. An adductor tenotomy was done. Then we proceeded with a femoral varus corrective osteotomy at the subtrochanteric level and fixed it with a proximal femoral plate (Fig. 4a) to reduce the neck shaft angle to 120° (Fig. 5). Lastly, a femoral medial caput epiphysiodesis was done by curetting the inferior medial physis of the femoral caput (Fig. 4b).
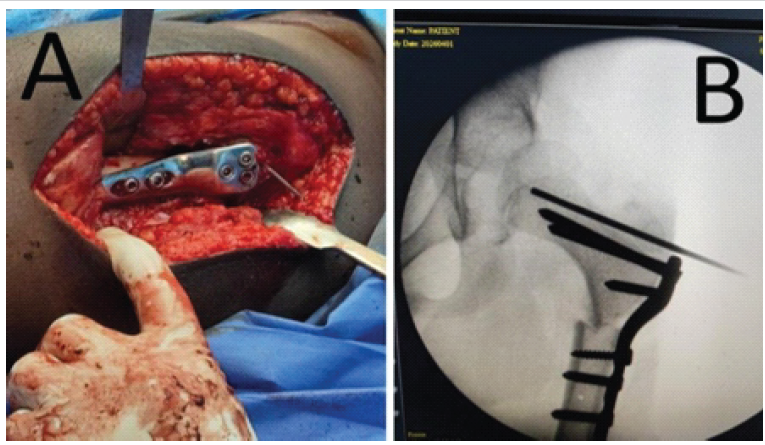
Figure 4: (a) Intraoperative clinical photograph of the left proximal femur fixation. Surgical exposure reveals the site of the varus corrective osteotomy site at the subtrochanteric level fixed with a proximal femoral plate, (b) Intraoperative fluoroscopic visualization of the medial femoral caput epiphysiodesis. C-arm image demonstrating structural fixation with the proximal femoral plate. A curette is introduced through the femoral neck to meticulously curette the inferior-medial physis of the left femoral caput, providing targeted growth modulation to correct the caput valga deformity.
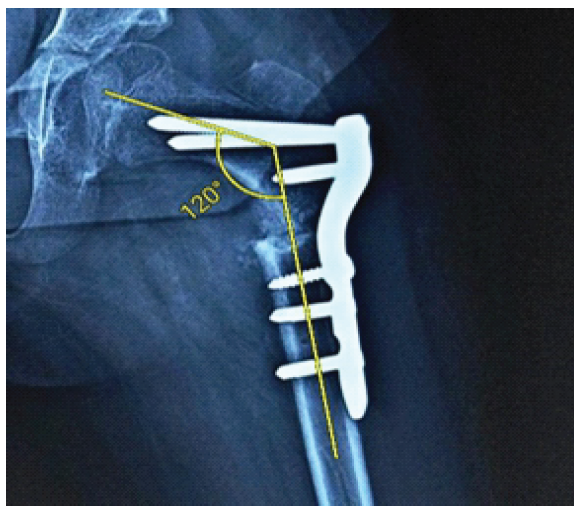
Figure 5: Post-operative radiographic evaluation of the left hip reconstruction. Anteroposterior radiograph demonstrating stable reduction of the left hip joint following an open adductor tenotomy, a proximal femoral varus corrective osteotomy, and a medial femoral caput epiphysiodesis. Rigid internal fixation achieved with a specialized proximal femoral plate reveals a neck-shaft angle corrected to 120°.
Specialised anaesthetic management:
This child required specialised anaesthetic care. General anaesthesia was induced with intravenous fentanyl 60 mcg, propofol 50 mg and atracurium 15 mg. Tracheal intubation was successful with a 5.0 mm cuffed tube. Maintenance relied on sevoflurane in an oxygen-air mixture; nitrous oxide was strictly avoided due to its inhibition of cobalamin-dependent enzymes. Intraoperative fluids were restricted to 0.9% normal saline to prevent exogenous lactate loading. One unit of packed red blood cells countered an estimated 220 mL blood loss. Cefuroxime, 1.6 g, was administered as surgical antibiotic prophylaxis. Reversal of neuromuscular blockade was achieved with neostigmine 1.5 mg and glycopyrrolate 0.3 mg.
Post-operative challenges:
Post-operative challenges include the spasticity that was triggered possibly due to a metabolic crisis, which further complicated his management process. This required intensive care unit care for his metabolic and spasticity management in the form of a fentanyl infusion. In the lower limbs, the spasticity led to left hip and knee flexion deformities, left foot equinus, right foot dorsiflexion and toe flexion deformities. With the aid of our occupational therapy team, the child was measured up for a left hip abduction brace of 30° that was used to prevent a hip dislocation postoperatively. Multiple other static orthotic devices, such as a left ankle-foot orthosis and anterior knee splint, were used to mobilise him with walker support and also to prevent the formation of contractures due to spasticity (Fig. 6a and b). A left-sided thumb abduction splint was also applied for the thumb adduction deformity. Despite utilising maximum doses of neurological muscle relaxants, persistent left knee flexion and ankle equinus contractures severely restricted the patient’s mobility. Following a multidisciplinary consultation with the paediatric neurology team, 50 units of botulinum toxin injection were administered directly into the child’s left medial hamstring (Fig. 7a), and an additional 50 units were injected into the left gastrocnemius muscle (Fig. 7b).

Figure 6: Post-operative clinical photograph demonstrating the various orthotic devices. (a) The patient is positioned supine in bed demonstrating application of a specialized hip abduction brace set at 30° to secure structural joint stability. Concurrently, a customized left ankle-foot orthosis and an anterior knee extension splint are applied to prevent the formation of fixed soft-tissue contractures due to spasticity. (b) The patient is being mobilized with an anterior knee splint and ankle foot orthosis aided with the support of a walker.
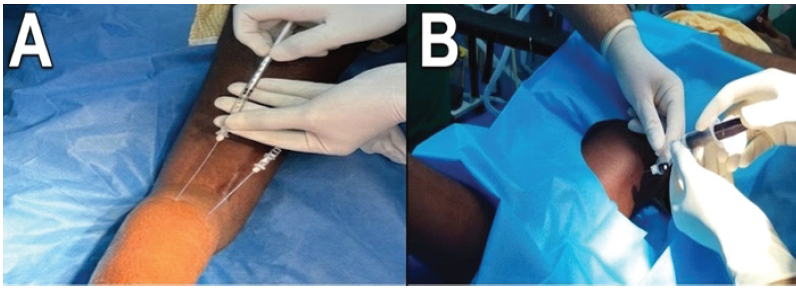
Figure 7: Post-operative chemical neuromodulation for persistent spasticity. (a) Targeted administration of botulinum toxin Type A injection into the spastic left medial hamstring muscles, (b) Synchronous administration of botulinum toxin Type A injection directly into the spastic left gastrocnemius muscle belly. This dual-target intervention effectively suppressed the spasticity facilitating compliance with custom hip abduction orthoses.
Hip dislocations are quite rare in OADs but have been noted [4]. Neuromuscular disorders in general pose a threat in the management of these conditions in the form of recurrence. Hip dislocations secondary to MMA pose a dual challenge. While the anatomy may be corrected, the bigger threat is the dynamic muscular forces due to spasticity. Suppressing these forces seems to be critical to prevent recurrence. Hence, we also administered a botulinum toxin injection following surgery to reduce the spasticity during the time needed for the union of the osteotomy site. There are various presentations of MMA depending on the degree of genetic mutation. The patient presented with a B12-responsive intermediate phenotype, a variant that typically manifests in childhood with a more stable metabolic profile than the classic neonatal-onset form. Unlike “benign” adult variants or severe subtypes, this intermediate profile allows for a specialised management window. By administering hydroxocobalamin to reduce residual enzyme activity, alongside a restricted propionic amino acid diet and levocarnitine for metabolite clearance, we achieved the physiological stability necessary for our orthopaedic intervention. This metabolic responsiveness was critical in preventing catabolism and ensuring perioperative safety [3]. MMA represents one of the most challenging metabolic disorders encountered in paediatric anaesthesia. This case illustrates several key principles in managing such patients for prolonged major surgery [5]. Avoidance of metabolic triggers was central to our strategy. Nitrous oxide was excluded from the anaesthetic plan, as it irreversibly inactivates methionine synthase and impairs cobalamin-dependent pathways, potentially precipitating acute decompensation in MMA [5,6]. Lactate-containing fluids were substituted with normal saline [6]. Regional anaesthesia as an adjunct played a pivotal role [6]. Caudal epidural blockade with bupivacaine and morphine attenuated the surgical stress response, reduced systemic opioid requirements, and provided extended post-operative analgesia – all critical in limiting catabolism [6]. OADs are considered a cerebral palsy mimic but are attributed to a neurogenic cause [7]. The major difference between MMA and cerebral palsy is that MMA is a progressive neurometabolic disorder, whereas the latter is not. Damage to the basal ganglia from toxic metabolites can lead to dystonia rather than steady spasticity seen in cerebral palsy, which creates erratic forces on the joint. Unlike the predictability of spastic diplegia, the neuromuscular profile of MMA-related hip instability is characterised by an unpredictable interplay of spasticity and dystonia, causing recurrent episodes of hip subluxation leading to an eventual dislocation. As Sung et al. noted for children with cerebral palsy [8], prophylactic varus osteotomy could have been done earlier, but the dystonic muscle forces would have continued to pose a risk of hip dislocation; hence, we provided him with an abduction brace initially. Unlike primary developmental dysplasia of the hip (DDH), where the defect is often structural or mechanical at birth, hip instability in MMA is neurogenic. While the acetabulum is initially well formed, the absence of a properly seated femoral head, caused by neuromuscular imbalance, deprives the socket of the biological stimulus needed for deep formation [9]. Consequently, this could lead to secondary acetabular dysplasia over time. The development of coxa valga is due to the deforming muscle forces of the spastic muscles. A proximal femur varus osteotomy would reduce the risk of dislocation by decreasing the forces on the hip [8]. It also indirectly lengthens the muscles crossing the hip by shortening the femur. Finally, it also increases and hence improves the moment arm of the hip. These collectively reduce the chances of recurrence. Caput valga is a proximal femoral epiphyseal deformity due to tethered growth that has been mentioned in DDH cases [10]. This results in a horizontal orientation of the physis with the femoral epiphysis in valgus with reference to the femoral neck axis [10]. In our case, it was the result of the neuromuscular forces. This entity has not been reported in MMA. In our case, we avoided a transphyseal screw due to the risk of joint penetration and secondary complications such as chondrolysis [10]. Hence, we curetted the inferior medial proximal femoral physis with the hypothesis that normal growth at the superior lateral physis would eventually correct this deformity.
The management of complex organic acidurias like MMA with hip dislocation necessitates a multidisciplinary approach. Successful outcomes depend on the integrated efforts of pediatric neurology for metabolic stability, orthopedics for structural correction and mobility, anesthetic expertise for intraoperative metabolic management, and a dedicated rehabilitative team for aggressive targeted physiotherapy and occupational therapy to optimize functional recovery and post-operative nursing care. Unlike an osteotomy correction for other pathologies, this child requires long term surveillance till adulthood and lifetime metabolic management.
Because hip dislocation in late-onset methylmalonic acidemia is driven by dystonia rather than a static mechanical defect, achieving long-term skeletal stability requires a dual-target approach. Definitive surgical management must be paired with aggressive neurological directed medical therapy to fight the dynamic muscular forces which seem to be the biggest threat in this disease.
References
- 1. Jin L, Han X, He F, Zhang C. Prevalence of methylmalonic acidemia among newborns and the clinical-suspected population: A meta-analyse. J Matern Fetal Neonatal Med 2022;35:8952-67. [Google Scholar] [PubMed]
- 2. Shibata N, Hasegawa Y, Yamada K, Kobayashi H, Purevsuren J, Yang Y, et al. Diversity in the incidence and spectrum of organic acidemias, fatty acid oxidation disorders, and amino acid disorders in Asian countries: Selective screening vs. Expanded newborn screening. Mol Genet Metab Rep 2018;16:5-10. [Google Scholar] [PubMed]
- 3. Ramsay J, Morton J, Norris M, Kanungo S. Organic acid disorders. Ann Transl Med 2018;6:472. [Google Scholar] [PubMed]
- 4. Prasad N, Gottlich C, Nhan D, Hamosh A, Sponseller PD. Orthopaedic problems in 35 patients with organic acid disorders. J Pediatr Orthop 2021;41:e457-63. [Google Scholar] [PubMed]
- 5. Sharar SR, Haberkern CM, Jack R, Scott CR. Anesthetic management of a child with methylmalonyl-coenzyme a mutase deficiency. Anesth Analg 1991;73:499-501. [Google Scholar] [PubMed]
- 6. Gupta A, Dudeja Y, Ramachandran R, Subramaniam R. Anaesthetic considerations in a child with methylmalonic acidemia and its literature review. BMJ Case Rep 2020;13:e237270. [Google Scholar] [PubMed]
- 7. Pearson TS, Pons R, Ghaoui R, Sue CM. Genetic mimics of cerebral palsy. Mov Disord 2019;34:625-36. [Google Scholar] [PubMed]
- 8. Sung KH, Kwon SS, Chung CY, Lee KM, Kim J, Lee SY, et al. Fate of stable hips after prophylactic femoral varization osteotomy in patients with cerebral palsy. BMC Musculoskelet Disord 2018;19:130. [Google Scholar] [PubMed]
- 9. Presedo A, Rutz E, Howard JJ, Shrader MW, Miller F. The etiology of neuromuscular hip dysplasia and implications for management: A narrative review. Children (Basel) 2024;11:844. [Google Scholar] [PubMed]
- 10. Torode IP, Young JL. Caput valgum associated with developmental dysplasia of the hip: Management by transphyseal screw fixation. J Childrens Orthop 2015;9:371-9. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 10, 2020 Reviewers Acknowledgement & Photo-gallery August 2020
August 10, 2020 Reviewers Acknowledgement & Photo-gallery August 2020 July 10, 2024 Selection of Interferential Screw for Fixation of Graft in Tibial Tunnel during Anterior Cruciate Ligament Reconstruction by Novel Probe Test
July 10, 2024 Selection of Interferential Screw for Fixation of Graft in Tibial Tunnel during Anterior Cruciate Ligament Reconstruction by Novel Probe Test July 10, 2022 Impressive Remodeling of the Fractured Femur with Transposition of the Fractured Parts, Treated Conservatively with skin Traction, in a 3-Year-Old Boy
July 10, 2022 Impressive Remodeling of the Fractured Femur with Transposition of the Fractured Parts, Treated Conservatively with skin Traction, in a 3-Year-Old Boy September 24, 2017 Isolated Pure Lateral Dislocation of Elbow in a 9-year-old Child: A Rare Case Report
September 24, 2017 Isolated Pure Lateral Dislocation of Elbow in a 9-year-old Child: A Rare Case Report