
This study shows myofascial release and therapeutic exercises are effective treatments for Bertolotti’s syndrome, despite their established use for low back pain.
Dr. Shweta Atwani, Department of Physiotherapy, NIMS University, Jaipur, Rajasthan, India. E-mail: atwanishweta149@gmail.com
Abstract
Introduction: Bertolotti’s syndrome is characterized by chronic low back pain due to lumbosacral transitional vertebrae (LSTV), where caudal lumbar vertebral enlargement leads to fusion or articulation with the sacrum or ilium. This condition results in discogenic disease and mobility restriction, causing pain in the back, hip, groin, and legs, often related to L5 nerve distribution. The discomfort varies and is linked to pathologies from LSTV, including scoliosis and joint issues. LSTV types, categorized by the Castellvi system, range from dysplastic processes to complete sacralization. The syndrome’s incidence is debated, estimated at 4–36%. Myofascial release (MFR) is a therapeutic technique targeting fascia to reduce muscle tension, improve mobility, and alleviate chronic pain. Previous studies suggest MFR, combined with other treatments, effectively reduces low back pain. However, research has not specifically assessed MFR’s impact on Bertolotti’s syndrome. This study aims to investigate MFR’s effects on the thoracolumbar fascia and quadratus lumborum combined with therapeutic exercises for affected patients.
Objectives: The objective of the study was to assess the effect of lumbosacral MFR along with therapeutic exercises for a patient with Bertolotti’s syndrome.
Case Report: The patient underwent 6 weeks of physiotherapy, with sessions 5 times weekly, each lasting 40–45 min. Initial exercises included lumbar flexion in quadruped and standing positions. The Bird Dog exercise involved alternating arm and leg raises. Spinal extension exercises were performed in prone positions. MFR techniques targeted the thoracolumbar fascia and quadratus lumborum, applying sustained pressure for specific durations to alleviate tension.
Results: The patient showed significant improvement in symptoms during treatment. The pain score decreased from 6/10 to 1/10, and the Oswestry disability index score was 4/50, indicating no disability. The patient performed daily activities comfortably and sat for 80 min without pain.
Conclusion: A patient with LSTV and persistent LBP following prior treatments might have their pain associated with reduced mobility. MFR and therapeutic exercises may serve as effective treatments for cases like type IIB Castellvi LSTV.
Keywords: Bertolotti’s syndrome, lumbosacral transitional vertebrae with low back pain, myofascial release, Castellvi Type IIb, lumbosacral myofascial release.
Bertolotti Syndrome is a clinical diagnosis for patients who suffer pain caused by a lumbosacral transitional vertebra (LSTV). LSTVs are birth defects in the vertebrae where an extended fifth lumbar (L5) transverse process connects or joins with the first sacral segment (S1). This transitional vertebra is characterized by either the sacralization of the L5 vertebra or the lumbarization of the S1 segment [1]. An LSTV is an anatomical variation characterized by different degrees of closeness or pseudoarticulation between the lowest lumbar vertebra and the sacral ala. LSTVs arise due to a combination of local chemotactic signals during embryonic development, causing the typically bifurcated and binary “lumbar” and “sacral” vertebrae to develop morphologically along distinct pathways. LSTVs are increasingly acknowledged as the most prevalent congenital defect of the lumbosacral spine, with an incidence ranging from 4% to 35%, and numerous practitioners report a general incidence of 10–12% based on the older Castellvi classification [2]. Individuals with an LSTV may experience symptoms associated with both arthritic and neurological irritation. This condition is typically referred to as Bertolotti syndrome, where the transitional anatomy leads to pain in the back, hip, groin, and/or legs along the L5 distribution. Bertolotti syndrome is a cause that is frequently missed in the assessment and management of back pain, with a cited prevalence of 4.6–7% in adults experiencing lower back pain. This is likely because diagnosing Bertolotti syndrome is complicated and often requires a process of exclusion for certain cases. The existing treatment options for this condition include conservative measures like rest, physiotherapy, manipulation, and injections, as well as surgical procedures like resection and fusion. Over a hundred years have passed since Mario Bertolotti initially detailed the clinical link between back and leg pain and the anatomical characteristics of LSTV. et al. subsequently categorized LSTVs into four main groups, which include seven subcategories. In their report, they aimed to forecast the occurrence of lumbosacral herniated discs, rather than to detect patients with Bertolotti syndrome [2]. Bertolotti’s syndrome is characterized by persistent low back pain resulting from LSTV. In these patients’ spines, the enlargement of the caudal lumbar vertebrae at the transverse process results in the fusion or articulation of the transverse process with either the sacrum or the ilium, leading to discogenic disease and restricting mobility [3]. This congenital LSTV anomaly, which has diverse manifestations, can manifest as lower back pain syndrome in a patient’s thirties and forties. When the origin of the low back pain is determined to be LSTV, it is identified as Bertolotti’s syndrome. The discomfort associated with Bertolotti’s syndrome varies and stems from various pathologies resulting from the LSTV. These conditions encompass scoliosis, joint arthropathy, and muscle strains of the iliopsoas and quadratus lumborum. The alteration of the transitional vertebra can lead to nerve compression from compressed discs, resulting in neuropathic pain. Patients typically indicate daily pain levels exceeding 5 out of 10. Patients with Bertolotti’s syndrome report considerable pain and an average score exceeding 36% on the Oswestry disability scale, indicating moderate disability that impacts various elements of everyday living. Patients with LSTV often exhibit more pronounced spinal degeneration above the deformity compared to other causes of chronic lower back pain. Nonetheless, they generally experience comparable degrees of pain and disability to individuals with back pain who do not have LSTV. Due to its resemblance in pain and disability to other back pain sources, a Bertolotti’s Syndrome diagnosis consists of two components: A clinical pain evaluation and advanced imaging revealing these anomalies [3]. Clinically, Bertolotti’s syndrome manifests as different types of pain and tenderness, either symmetrically or asymmetrically, in the sacroiliac region, hip, and groin. Radicular pain could arise from nerve compression, or pseudo-radicular pain may occur from the bone-on-bone contact at the pseudo-articulated joint of the transverse vertebrae. Bertolotti’s syndrome manifests as non-specific back pain; consequently, diagnosis confirmation must be achieved through radiologic imaging of the lumbosacral spine. Radiographs of the lumbosacral spine will show either unilateral or bilateral enlargement of the transverse processes, which may articulate with the sacrum or ilium. A magnetic resonance imaging (MRI) of the lumbosacral spine can be added if radicular pain suggests the possibility of discogenic pain [3]. Bertolotti’s syndrome includes various forms of LSTV categorized by the Castellvi system. In 1984, Dr. Antonio Castellvi identified four specific types of LSTV by analyzing myelograms from 200 patients. The four categories of LSTV are the following: Type I – a dysplastic transverse process measuring a minimum of 19 cm in width; Type II – transverse process growth resulting in partial sacralization or lumbarization; Type III – full transverse process sacralization or lumbarization; and Type IV – a combination of complete sacralization and incomplete sacralization. Among the Castellvi classifications, Type 1 LSTV is the most common at 42%, then Type II at 38%, Type III at 8%, and Type IV at 5%. Disc herniations frequently occur at individual levels, although certain patients may experience herniations in several discs because of the LSTV [3,4] (Fig. 1).
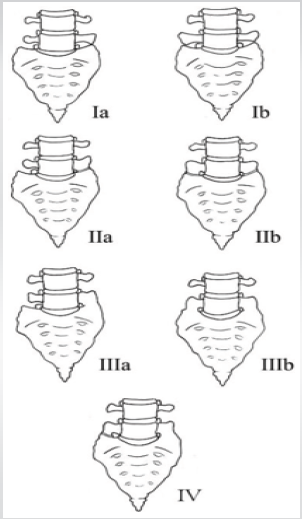
Figure 1: Illustration of Castellvi Classification of lumbosacral transitional vertebrae. Type I: Dysplastic transverse processes measuring a minimum of 19 mm in width. Ia: Unilateral (one side). Ib: Bilateral (both sides). Type II: Partial lumbarization or sacralization accompanied by an enlarged transverse process that creates a pseudarthrosis (false joint) with the nearby sacral ala. IIa: Unilateral. IIb: Bilateral. Type III: Total lumbarization or sacralization accompanied by an enlarged transverse process leading to full bony fusion with the neighboring sacral ala. IIIa: Unilateral. IIIb: Bilateral. Type IV: A combined condition in which one side exhibits a Type II presentation while the other side shows a Type III presentation.
The existence of an LSTV changes spinal biomechanics by inducing hypomobility at the L5/S1 segment and increasing hypermobility in neighbouring lumbar segments. This disturbance in the spine’s mechanical alignment is associated with the emergence of lower back pain, possibly due to premature arthritic changes, disc herniations, degeneration, or stenosis. A study by Otani in 2001 showed that disc herniations happen more often and at an earlier age in individuals with LSTV than in those without it. Additional research indicates a higher occurrence of foraminal stenosis, disc degeneration, and facet degeneration at levels above the LSTV. Hanhivaara noted that Castellvi Types II, III, and IV LSTV are associated with increased lumbar disc degeneration, except for L2-L3. Moreover, individuals experiencing low back pain and LSTV exhibit a greater occurrence of sacroiliac joint dysfunction compared to those who do not have it [3]. Bertolotti’s Syndrome shows a debated incidence, estimated between 4% and 36% among people with LSTV. Castellvi et al. found that 4% of asymptomatic chiropractic patients had LSTV (Castellvi types II-IV), while others reported 18.7% prevalence in the general population, with more men affected than women. Most diagnoses were Castellvi Type Ia and Ib, followed by IIa, IIb, IIIa, IIIb, and IV. Despite high LSTV incidence, many remain asymptomatic, igniting debates on its role in back pain. While Castellvi linked pain to spinal anomalies, others argue it’s not associated with LSTV, complicating the definition of Bertolotti’s true prevalence, affirmed by Elster’s 7% LSTV finding in pain patients [3]. Nardo et al. showed that LSTV was linked to LBP and pain in the buttocks; types II and IV exhibited the strongest association, likely due to the pseudoarticulation between the L5 transverse process and the sacrum. Heightened severity and occurrence of LBP were similarly linked to Types II and IV. The relation between LBP and LSTV subgroups indicated that LSTV Types II and IV were connected to the existence of pain, along with pain severity and occurrence. The underlying pathophysiologic mechanism of pain linked to LSVT is still not well understood. Several suggested mechanisms involved the correlation of extraforaminal stenosis, disc herniations, and spinal stenosis with LSTV. Buttock pain linked to LSTV in Types II and IV might arise from nerve compression. Mechanical irritation of the nerve root can lead to pain with radicular features. Certain studies have shown a link between LSTV and extraforaminal stenosis resulting from the abnormal transverse process [5]. Bertolotti Syndrome involves multiple factors contributing to back pain. The majority of the impacted patients suffer from scoliosis. The unusual mechanical pressure results in facet joint arthropathy, along with iliopsoas and quadratus lumborum strain. Compression of nerve roots caused by the constriction of intervertebral foramina from enlarged fan-shaped transverse foramina can result in neurogenic claudication. A higher occurrence of disc protrusion or extrusion in the disc located above the transitional L5 vertebra has been observed in individuals with LBP. A reduced occurrence of disc protrusion or extrusion was observed in the disc situated beneath the transitional vertebra [6]. Myofascial release (MFR) is a distinct hands-on therapy method that aims to alleviate tension and limitations in the fascia, a connective tissue that envelops and sustains muscles, bones, and organs across the body. This treatment seeks to enhance mobility, decrease pain, and improve overall physical performance by targeting imbalances and limitations within the fascial system, an intricate myofascial and aponeurotic framework encasing the body that is essential for stabilizing the lumbar vertebrae on the sacral base [7]. MFR, which entails applying a low-load, long-duration stretch to the myofascial complex, is extensively utilized by physical therapists in treating LBP [8]. Fascia is richly supplied with mechanoreceptors that react to manual pressure; their activation in various spinal components like the posterior ligaments and zygapophyseal joint capsule has been associated with alterations in the neuromuscular reaction of the erector spinae [9,10,11]. While the exact mechanisms of action behind MFR remain uncertain, stimulating fascial mechanoreceptors could potentially trigger comparable neuromuscular alterations. Earlier research indicates that MFR, when used alongside other therapies, can alleviate pain and disability in those suffering from chronic low back pain [12,13]. However, no studies have specifically analyzed the effect of MFR on a patient with Bertolotti’s syndrome. Therefore, the present study analyses the effect of MFR on thoracolumbar fascia and quadratus lumborum with a therapeutic exercise protocol on a patient with Bertolotti’s syndrome.
Ethical considerations:
Ethical clearance was obtained from the Institutional Ethics Committee of NIMS University, Jaipur, Rajasthan. Approval No: NIMS/PTOT/Ethical/Dec/2025/02. Written informed consent was obtained from the participant. Confidentiality was maintained throughout the study.
The patient was a 30-year-old male working in an IT company as an IT analyst with a 6-month history of lower back pain radiating in the right leg that had been occasional before but had become much worse in the last 2 months. For his job, he was required to sit at least 10–12 h continuously. He consulted a general physician who prescribed him some non-steroidal anti-inflammatory drugs (NSAIDs) and muscle relaxants for the treatment, which, after 2 weeks, did not relieve his symptoms, so he stopped the medications and went to an orthopedic surgeon. The surgeon then ordered lumbar radiographs after routine examination, which were then reviewed by the radiologist. The radiograph revealed Castellvi Type IIb LSTV. The surgeon then referred the patient to the physical therapy clinic for further treatment with the primary diagnosis of LSTV with low back pain.
Clinical findings:
The patient described his symptoms as a dull, continuous ache causing discomfort in daily activities, leaving him incapable of performing ADLs. The condition got worse when he sat or stood continuously for a long time (more than 30–40 min) and felt better when he rested.
Investigations:
MRI:
Lumbarization of the S1 vertebral body was seen in the MRI. The L4-L5 level shows a diffuse annular disc bulge and mild protrusion and an annular disc tear indenting the ventral thecal sac. There is bilateral neural foraminal narrowing with compression of the right traversing nerve root. L4-L5, L5-S1 disc annular tear indenting the ventral thecal sac. Disc desiccation at L4-L5 and L5-S1 (Figs. 2, 3, 4) was also seen.
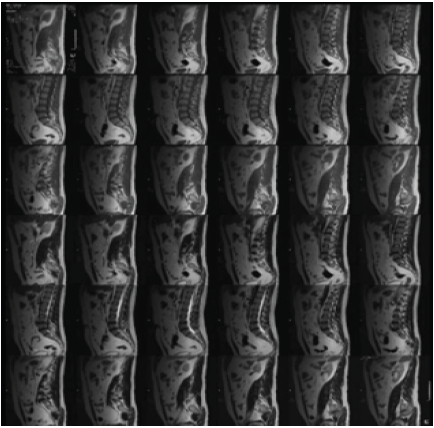
Figure 2: Magnetic resonance imaging-Lumbo-sacral spine.
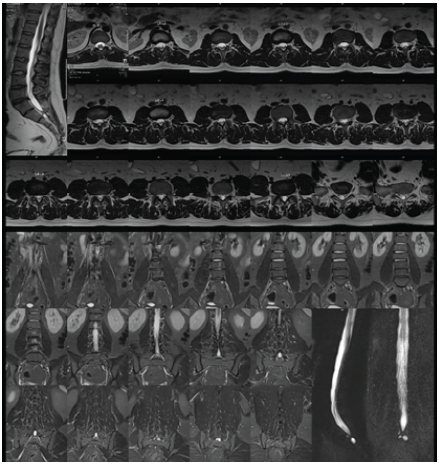
Figure 3: Magnetic resonance imaging-Lumbo-sacral spine.
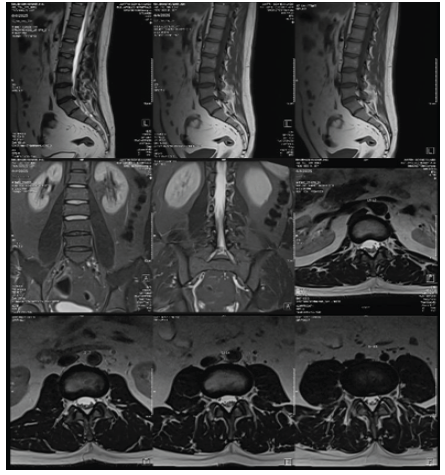
Figure 4: Magnetic resonance imaging-Lumbo-sacral spine.
X-ray:
Castellvi Type IIb LSTV was seen in the X-ray. L5 transverse processes were enlarged on both sides. Each enlarged transverse process showed a pseudo-articulation (false joint) with the sacral ala. There was no complete bony fusion, which ruled out Type III, and the involvement was bilateral, which made it “b” (Fig. 5).

Figure 5: X-ray, Lumbo-sacral spine AP view.
Examination/evaluation:
On the initial visit, a history, including a body chart, was taken, and a physical examination was performed. Physical examination revealed an ectomorphic build with a slouched posture. Tenderness of Grade 2 noted at left PSIS. Straight leg raising was positive over the right leg, which suggested that the patient was having lumbar radiculopathy. At the time of the physiotherapy evaluation, the pain was described as a moderate 6 out of 10 on the Numeric Pain Rating Scale (NPRS) and was in the right lower back region just superior to the right PSIS, radiating to the right buttock. Pain was aggravated by bending forward and standing or sitting for longer than 40 min. Oswestry Low Back pain disability questionnaire/The Oswestry Disability Index (ODI) was administered and scored. The ODI is an LBP questionnaire consisting of 10 questions used to measure low back disability, stage a patient’s acuity status, and monitor change over time. The higher scores indicate greater levels of disability due to LBP. The ODI score obtained from the 10 questions was 24 points out of 50 points, indicating a moderate disability (48%).
Diagnosis:
The integration of subjective and objective assessments produced the following findings. The patient experienced persistent LBP for 6 months. His initial ODI score was 48%, reflecting moderate disability, while his NPRS score was 6. The LBP of the patient was thought to be linked to hypomobility in the lumbar spine due to the Castellvi Type IIb LSTV.
Physiotherapy intervention:
The patient was explained in detail about the study, its aim, objectives, and procedures. Informed consent was signed before the administration of treatment. The patient was recommended to maintain his daily routine without changes or extended rest to accurately evaluate the impact of MFR and therapeutic exercises. The patient underwent physiotherapy treatment 5 days a week for 6 weeks. Each session was 40–45 min. The initial mobility exercise involved a quadruped lumbar flexion activity. He was directed to hold the flexed position for 30 s and to repeat this 3 times. The second lumbar exercise involved a standing single-leg lumbar flexion and side-bending activity aimed at targeting the stretch specifically to the right lumbosacral area. He was directed to maintain this stance for 30 s for 2 sets [14].
Bird dog exercise:
The individual is in a quadruped stance and executes the bird dog exercise. The patient raises one hand upwards and the opposite leg upwards. This is done again with the other leg and the hand. It is recommended to perform this exercise for 10 repetitions [15].
Exercises for spinal extension:
- This patient is in a prone position on the mat, raising one leg into the air and then lifting the other leg up. The individual raises both legs off the ground for 5–10 s. This activity is performed in sets of 10 repetitions. At first, the patient does just 2–3 sets, gradually increasing to 10 sets [15]
- The patient is positioned face down on the mat and raises both hands above while maintaining the position for 5–10 s. This activity is performed for 10 repetitions in each set. At first, the patients do only 1–2 sets, and then gradually it is raised to 5 sets.
- This exercise is done with the patient positioned prone on the mat. The patient first raises one arm and then the opposite leg. This action is performed again with the other arm and leg. This activity is performed for 10 repetitions in each set. At first, the patients do just 2–3 sets, which is gradually increased to 10 sets [15].
MFR of the thoracolumbar fascia: Maintained pressure is exerted for 5 min along the fascia, without gliding over the skin or pushing the tissue, employing a cross-handed grip with hands positioned at the T12-L1 regions and on the sacrum [16]. MFR of the quadratus lumborum involves positioning the elbow of the cranial hand above the iliac crest, laterally to the lumbar paravertebral muscles, and over the quadratus lumborum area, while the caudal hand rests on the subject’s thigh. Gentle pressure is subsequently exerted with the elbow angled toward the centre of the spinal column while the opposite hand performs light traction along the patient’s leg; this method is utilized for 7 min on the affected side [16]. Home program (after 6 weeks of treatment): The exercises provided to the patient in the study protocol were recommended 2 times daily with 15 repetitions for each exercise, encompassing both mobility exercises and spinal extension exercises. For office tasks, it was advised that he take stretching breaks every 1–2 h. He was also told to refrain from sitting for over 80 min at a stretch.
Treatment outcome:
The patient indicated substantial progress and a decrease in symptoms over the course of the treatment phase. By the conclusion of the treatment, the pain score on the NPRS dropped from a peak of 6/10–1/10, and the ODI score obtained from the 10 questions was 4 points out of 50 points, indicating no disability (8%). The patient was able to perform the ADLs actively without any discomfort, and he reported that he was able to sit for 80 min without any pain or discomfort. Follow Up (after 6 weeks of completion of treatment): The patient performed the prescribed exercises each day after the completion of the study duration, and the evaluation revealed an NPRS of 1/10, experiencing discomfort only after sitting for over 100 min. The ODI score recorded was 5 points, signifying no disability.
This case report illustrates the feasibility of conducting MFR on a patient believed to have LBP linked to a Type IIB LSTV (Bertolotti’s). The objectives for this patient focused on restoring complete pain-free spinal movement and achieving pain-free ADLs. On completion of the treatment, the patient exhibited complete pain-free active and passive spinal movement while sitting and standing, resumed pain-free ADLs, and achieved an 8% score on the ODI, indicating extremely minimal or no disability related to his LBP. These findings align with additional research on the LSTV that similarly indicated a decrease in pain and/or disability following various manual therapies like MFR or exercise regimens [16]. Debate persists regarding whether an LTV can cause LBP leading to Bertolotti syndrome. Several studies have indicated that radiological evidence of LTVs appears with the same frequency in patients with LBP as in those without. Consequently, it is challenging to ascertain whether the existence of an LSTV can be the only cause of LBP. The diarthrodial joint on the sacrum, which may arise during hemisacralization, can alter the biomechanics of the lumbar spine by inducing hypomobility at this region. The absence of movement at the LSTV level may lead to heightened stress in adjacent vertebral segments. This heightened stress and alteration in biomechanics may make an individual more susceptible to LBP when subjected to greater physical strain, such as sitting or standing for extended periods. Regrettably, there is scarce information regarding this proposed direct cause-and-effect connection [14]. Numerous studies have recorded various treatment approaches that successfully alleviate back pain and enhance mobility. In this group of patients, both surgical and conservative approaches can successfully address LSTV. Patients experiencing back pain, whether they have LSTV or not, typically undergo conservative treatment, which includes NSAIDs and physical therapy [17]. Positional changing exercises and spinal movement therapy were also suggested to enhance symptoms by boosting muscle strength, coordination, and adaptability [18].
Limitations and further recommendations:
Additional clinical observation concerning physiotherapy management is necessary with larger sample sizes and multiple clinical settings, and more standardized measurements of clinical outcomes to identify optimal comprehensive clinical practices for management of various classifications of Bertolotti’s syndrome to increase the accuracy rate of the study.
The patient discussed in this case report was referred to physical therapy due to a lack of improvement with prior treatments, which included rest, anti-inflammatory medications, and muscle relaxants. Even with the history intake and physical examination, it remains challenging to establish if this patient’s LSTV caused the LBP. The site of his discomfort around the LSTV, and the discovery of hypomobility in this region, suggest that the LSTV may have played a role in the pain and dysfunction resulting in Bertolotti’s Syndrome. This case report indicates that an MFR combined with therapeutic exercises might be an effective intervention for patients with LBP, even with a Type IIB Castellvi LSTV.
While MFR and therapeutic exercises are well-established for the conservative management of low back pain, their application to the management of Bertolotti’s Syndrome remains unexplored. This study bridges this gap by demonstrating that MFR and therapeutic exercises can be an effective treatment in Bertolotti’s Syndrome.
References
- 1. McGrath K, Schmidt E, Rabah N, Abubakr M, Steinmetz M. Clinical assessment and management of Bertolotti syndrome: A review of the literature. Spine J 2021;21:1286-96. [Google Scholar] [PubMed]
- 2. Jenkins AL 3rd., O’Donnell J, Chung RJ, Jenkins S, Hawks C, Lazarus D, et al. Redefining the classification for Bertolotti syndrome: Anatomical findings in lumbosacral transitional vertebrae guide treatment selection. World Neurosurg 2023;175:e303-13. [Google Scholar] [PubMed]
- 3. Crane J, Cragon R, O’Neill J, Berger AA, Kassem H, Sherman WF, et al. A comprehensive update of the treatment and management of Bertolotti’s syndrome: A best practices review. Orthop Rev (Pavia) 2021;13:24980. [Google Scholar] [PubMed]
- 4. Barwar N. Bertolotti’s Syndrome: Prevalence, Classification and Current Concepts of Management: A Review. Orthop Muscular Syst 2019;8:266. [Google Scholar] [PubMed]
- 5. Nardo L, Alizai H, Virayavanich W, Liu F, Hernandez A, Lynch JA, et al. Lumbosacral transitional vertebrae: Association with low back pain. Radiology 2012;265:497-503. [Google Scholar] [PubMed]
- 6. Aihara T, Takahashi K, Ogasawara A, Itadera E, Ono Y, Moriya H. Intervertebral disc degeneration associated with lumbosacral transitional vertebrae: A clinical and anatomical study. J Bone Joint Surg Br 2005;87:687-91. [Google Scholar] [PubMed]
- 7. Willard FH, Vleeming A, Schuenke MD, Danneels L, Schleip R. The thoracolumbar fascia: Anatomy, function and clinical considerations. J Anat 2012;221:507-36. [Google Scholar] [PubMed]
- 8. Barnes JF. Myofascial Release: The Search for Excellence: A Comprehensive Evaluatory and Treatment Approach. Pennsylvania: JF Barnes; 1990. [Google Scholar] [PubMed]
- 9. Schleip R. Fascial plasticity-a new neurobiological explanation: Part 1. J Bodyw Mov Ther 2003;7:11-9. [Google Scholar] [PubMed]
- 10. Holm S, Indahl A, Solomonow M. Sensorimotor control of the spine. J Electromyogr Kinesiol 2002;12:219-34. [Google Scholar] [PubMed]
- 11. Lalanne K, Lafond D, Descarreaux M. Modulation of the flexion-relaxation response by spinal manipulative therapy: A control group study. J Manipulative Physiol Ther 2009;32:203-9. [Google Scholar] [PubMed]
- 12. Ajimsha MS, Daniel B, Chithra S. Effectiveness of myofascial release in the management of chronic low back pain in nursing professionals. J Bodyw Mov Ther 2014;18:273-81. [Google Scholar] [PubMed]
- 13. Licciardone JC. Osteopathic manipulative treatment in patients with low back pain. Clin Rheumatol 2011;30:871-2. [Google Scholar] [PubMed]
- 14. Brenner AK. Use of lumbosacral region manipulation and therapeutic exercises for a patient with a lumbosacral transitional vertebra and low back pain. J Orthop Sports Phys Ther 2005;35:368-76. [Google Scholar] [PubMed]
- 15. Pandey E, Kumar N, Das S. Effect of stretching on shortened Quadratus Lumborum muscle in non-specific low back pain. Indian J Physiother Occup Ther 2018;11:80-6. [Google Scholar] [PubMed]
- 16. Arguisuelas MD, Lisón JF, Doménech-Fernández J, Martínez-Hurtado I, Coloma PS, Sánchez-Zuriaga D. Effects of myofascial release in erector Spinae myoelectric activity and lumbar spine kinematics in non-specific chronic low back pain: Randomized controlled trial. Clin Biomech (Bristol) 2019;63:27-33. [Google Scholar] [PubMed]
- 17. Almeida DB, Mattei TA, Sória MG, Prandini MN, Leal AG, Milano JB, et al. Transitional lumbosacral vertebrae and low back pain: Diagnostic pitfalls and management of Bertolotti’s syndrome. Arq Neuropsiquiatr 2009;67:268-72. [Google Scholar] [PubMed]
- 18. Chalian M, Soldatos T, Carrino JA, Belzberg AJ, Khanna J, Chhabra A. Prediction of transitional lumbosacral anatomy on magnetic resonance imaging of the lumbar spine. World J Radiol 2012;4:97. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 A Case of Fixation Using Poly-L-Lactic Acid Pins for Chronic Juvenile Massive Osteochondritis Dissecans of the Knee
February 1, 2026 A Case of Fixation Using Poly-L-Lactic Acid Pins for Chronic Juvenile Massive Osteochondritis Dissecans of the Knee June 1, 2026 Bipolar Clavicle Fracture: A Rare Entity of the Commonest Fracture – A Case Report
June 1, 2026 Bipolar Clavicle Fracture: A Rare Entity of the Commonest Fracture – A Case Report July 1, 2026 Response to Letter to the Editor: Clavicle Fracture Non-Union in a 3-Year-Old Child: A Case Report and Literature Review
July 1, 2026 Response to Letter to the Editor: Clavicle Fracture Non-Union in a 3-Year-Old Child: A Case Report and Literature Review January 10, 2021 Late Presenting Pediatric Radial Neck Fracture: A Case Report and Review of the Literature
January 10, 2021 Late Presenting Pediatric Radial Neck Fracture: A Case Report and Review of the Literature