
Successful distraction osteogenesis depends more on biological and mechanical principles than on strict osteotomy geometry.
Pr. Pierre-Louis Docquier, Department of Orthopedic and Trauma, Cliniques Universitaires Saint-Luc, UCLouvain, Bruxelles, Belgique. Av. Hippocrate 10, 1200 Bruxelles, Belgique Email-ID: pierre-louis.docquier@uclouvain.be
Abstract
Introduction: Distraction osteogenesis is usually performed using a low-energy transverse metaphyseal osteotomy.
Case Report: We report two cases of femoral lengthening in which unintended fracture propagation resulted in non-straight osteotomy configurations (step-cut and butterfly-shaped). In both cases, stable fixation was maintained, and gradual distraction proceeded without complications, with early regeneration formation observed.
Conclusion: These cases illustrate that, when fundamental biological and mechanical principles are respected, unintended non-straight osteotomies may remain compatible with successful distraction osteogenesis.
Keywords: Paediatric orthopaedics, distraction osteogenesis, osteotomy, step-cut, butterfly-shaped, follow-up.
Distraction osteogenesis (callotasis) is a well-established method for treating limb length discrepancy (LLD), notably in conditions such as congenital femoral deficiency, and is used primarily in children and adolescents [1,2]. Developed by Ilizarov in the mid-20th century, the technique is based on a low-energy metaphyseal osteotomy, a latency period of approximately 5–7 days, and a gradual distraction rate of about 1 mm/day, allowing controlled bone regeneration formation while preserving soft-tissue adaptation [3]. In most descriptions, the osteotomy is a simple low-energy transverse metaphyseal cut, performed with minimal soft-tissue stripping and maximal preservation of periosteal blood supply [4]. This biologically respectful technique has been extensively validated and consistently provides reliable regeneration formation when combined with appropriate distraction protocols [5]. Nevertheless, transverse osteotomies have theoretical mechanical limitations, including limited rotational stability and a relatively small interfragmentary cancellous contact area [6]. Consequently, overall mechanical stability depends heavily on the chosen fixation device. Despite these limitations, the transverse metaphyseal osteotomy remains the standard in distraction osteogenesis. Non-straight osteotomy geometries (including step-cut, oblique, Z-shaped, and sigmoid osteotomies) have been described in angular correction, subtrochanteric femoral shortening during hip arthroplasty, and in acute or limited limb lengthening procedures [7]. Studies suggest that these alternative configurations may offer greater intrinsic stability and increased interfragmentary bone contact compared with a simple transverse osteotomy [6]. However, their application in gradual distraction osteogenesis is sparsely described, and no evidence currently supports their superiority over the classical low-energy transverse metaphyseal osteotomy. Their precise role in limb lengthening, therefore, remains uncertain. The aim of this report is not to promote alternative osteotomy designs but to illustrate safe intraoperative management when fracture propagation occurs during distraction osteogenesis. These cases highlight that the resulting non-straight geometries can remain compatible with successful gradual distraction and raise the question of whether osteotomy design may influence mechanical or biological aspects of distraction osteogenesis.
The first case is that of a 17-year-old girl who was followed for a type 1 right congenital femoral deficiency associated with a clinically significant LLD. The initial discrepancy measured 6.1 cm in favour of the left side. A left knee epiphysiodesis performed in 2019 partially reduced the discrepancy to 4.1 cm. Her medical history included gastro-oesophageal reflux disease treated with esomeprazole. She had no allergies or other comorbidities. Standard radiographs and long-leg standing films demonstrated right femoral shortening without significant angular deformity, and femoral morphology was compatible with intramedullary lengthening (Fig. 1).
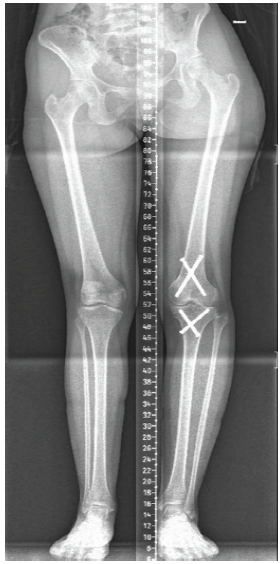
Figure 1: Long-leg standing radiograph of Case 1 showing right femoral shortening (4.1 cm) and four epiphysiodesis screws in the left knee.
By 2025, following the closure of all growth plates, the residual LLD (4.1 cm) remained symptomatic, and distraction osteogenesis was indicated. A low-energy transverse metaphyseal osteotomy of the right femur followed by fixation with a magnetic intramedullary lengthening nail (PRECICE®, NuVasive, San Diego, CA 92121, USA) was planned. The previous epiphysiodesis screws were removed during the same procedure. During completion of the osteotomy, unintended fracture propagation occurred, likely caused by incomplete bicortical drilling before the osteotome cut, resulting in a step-cut configuration, which was deemed sufficiently stable for gradual distraction. The step-cut configuration was not intentionally planned but resulted from fracture propagation. The post-operative course was uneventful. Pain was well controlled with a continuous femoral nerve block and multimodal systemic analgesia. The patient remained non-weight-bearing during distraction and for 1 month thereafter. Physiotherapy focused on early knee mobilisation. Distraction was well tolerated, with knee flexion discomfort being the only functional limitation. Follow-up radiographs demonstrated an 8 mm distraction gap at 1 week (Fig. 2) and 22 mm at 4 weeks, with early regenerate formation clearly visible (Fig. 3a). At the latest follow-up, radiographs confirmed consolidation of the regenerate, with maintained alignment and no mechanical complications (Fig. 3b).
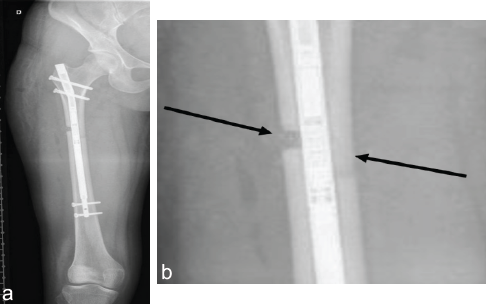
Figure 2: Magnetic intramedullary lengthening nail (a) with step-cut osteotomy (b). (a) Anteroposterior immediate post-operative radiograph showing the intramedullary lengthening nail. (b) Close-up radiographic view of the femoral step-cut osteotomy. The arrows indicate the step-cut osteotomy configuration resulting from intraoperative fracture propagation during a planned transverse metaphyseal osteotomy.
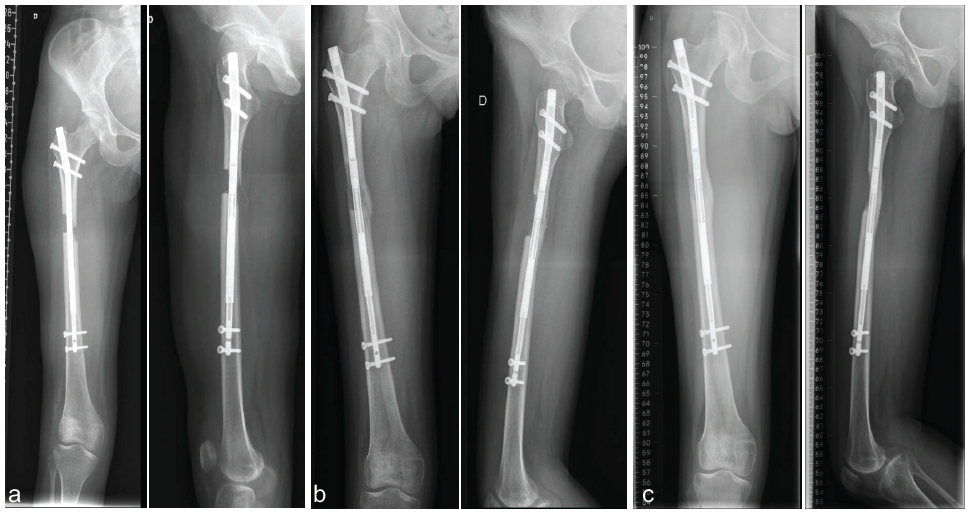
Figure 3: Radiographs of Case 1 during regenerate evolution. (a) Anteroposterior (AP) and lateral radiographs at 1 month postoperatively demonstrating early regenerate formation. (b) AP and lateral radiographs at 4-month follow-up, showing consolidation of the regenerate with maintained alignment. (c) AP and laterals radiographs at 6-months and the latest follow-up showing further consolidation with maintained alignment.
In the second case, we present a 5-year-old boy with multiple congenital anomalies, including severe femoral hypoplasia. A persistent, clinically significant LLD prompted further evaluation. Radiographs confirmed femoral hypoplasia without major angular deformity (Fig. 4).

Figure 4: Long-leg standing radiograph of Case 2 showing acetabulum agenesis and left iliac bone hypoplasia associated with left femoral congenital hypoplasia and limb length discrepancy.
Intramedullary lengthening was contraindicated due to age and abnormal femoral morphology [8]. A 5-cm femoral lengthening using a 3D hexapod external fixator (Orthex® hexapod system, OrthoPediatrics, Warsaw, Indiana, USA) was therefore planned. Intraoperatively, a low-energy metaphyseal osteotomy was initiated through a minimally invasive approach. During completion, fracture propagation resulted in a butterfly-shaped osteotomy with a central wedge fragment. Fracture propagation was likely related to altered femoral morphology and bone quality in congenital femoral deficiency. The configuration was assessed as sufficiently stable and was accepted for gradual distraction. A 3D hexapod external fixator was applied (Fig. 5).
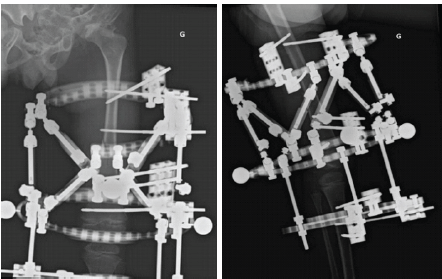
Figure 5: Anteroposterior and lateral radiographs obtained 3 days postoperatively following application of the hexapod external fixator.
The post-operative course was uncomplicated, with clean pin sites and early mobilisation. Distraction was initiated after the latency period, following standard protocol. Radiographs 1 month postoperatively showed approximately 3 cm of distraction (Fig. 6), with further progression confirmed 3 months postoperatively (Fig. 7a). The hexapod was removed, and a long-leg cast was applied for 2 weeks. At the latest follow-up, the child is walking without protection. Radiographs demonstrated progressive maturation and consolidation of the regenerate, with stable alignment and no pin-site or mechanical complications (Fig. 7b).
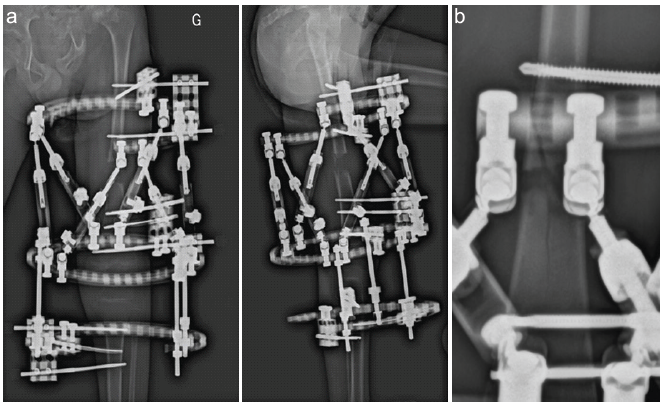
Figure 6: Four-week post-operative radiographs demonstrating ongoing distraction in Case 2. (a) Anteroposterior and lateral radiographs showing distraction progression with the 3D hexapod external fixator. (b) Close-up radiographic view of the butterfly-shaped osteotomy. The arrows indicate the butterfly-shaped osteotomy configuration resulting from intraoperative fracture propagation during a planned transverse metaphyseal osteotomy.
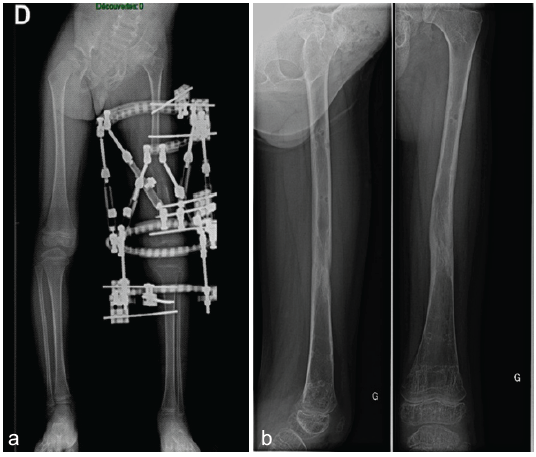
Figure 7: Radiographs of Case 2 during and after femoral lengthening. (a) Mid-distraction Anteroposterior (AP) radiograph showing the butterfly-shaped osteotomy configuration. (b) AP and lateral radiographs at 8-months and the last follow-up after frame removal, showing progressive regenerate maturation with maintained alignment.
Distraction osteogenesis is widely used to manage congenital or acquired lower LLD [2,3,8,9]. Its success is based on a low-energy metaphyseal osteotomy, preservation of periosteal vascularity, stable fixation, and controlled distraction [3,8,9,10]. The low-energy transverse metaphyseal osteotomy remains the standard approach due to its biological safety and predictable regenerate formation [3,8,9,10], despite its theoretical mechanical limitations [6]. Non-straight osteotomy geometries have been described in other orthopaedic settings, including angular correction and subtrochanteric shortening in hip arthroplasty, and may offer enhanced rotational stability and increased interfragmentary bone contact [6,7,11,12,13]. Their use in gradual distraction osteogenesis is only sparsely reported, and no study has shown clear superiority over the classical transverse cut [2,3,8]. In the present cases, intraoperative fracture propagation during an intended transverse osteotomy required conversion into non-straight geometries. In both patients, the modified osteotomies (step-cut and butterfly-shaped) offered sufficient intrinsic stability and cancellous bone contact to permit safe distraction without complications. Early regenerate formation occurred at both osteotomy sites. These observations are limited by the accidental nature of the osteotomy patterns and the absence of biomechanical comparison. However, they suggest that osteotomy geometry may be more flexible than traditionally assumed, provided that the fundamental principles of distraction osteogenesis (preserved vascularity, stable fixation, and an appropriate distraction rate) are respected [2,6]. Nevertheless, these cases do not support any claim of superiority of non-straight osteotomies over the classical transverse metaphyseal cut, which remains the standard technique. Further biomechanical and clinical studies are warranted to determine whether osteotomy design significantly influences mechanical behavior or biological outcomes during distraction osteogenesis.
These two cases illustrate that unintended fracture propagation during a planned low-energy transverse metaphyseal osteotomy does not necessarily compromise the feasibility of distraction osteogenesis. When biological principles are preserved and fixation remains stable, controlled non-straight osteotomy configurations, such as step-cut or butterfly-shaped patterns, may still allow safe and effective limb lengthening. These observations do not support the routine use of non-straight osteotomies in distraction osteogenesis, and the classical transverse metaphyseal osteotomy should remain the standard technique. However, in selected intraoperative situations, adapting the osteotomy geometry may represent a reasonable salvage strategy without jeopardising the lengthening process.
In distraction osteogenesis, controlled acceptance of a non-straight osteotomy may allow continuation of lengthening when intraoperative fracture propagation occurs, provided stability and biology are preserved.
References
- 1. Azhideh A, Hosseini N, Haseli S, Park C, Venugopal N, Abadi A, <em>et al</em>. Osteotomies: Indications, imaging appearance, surgical techniques, and complications. Diagnostics (Basel) 2025;15:1184.</li> [Google Scholar] [PubMed]
- 2. <li>Schep NW, Van Lieshout EM, Patka P, Vogels LM. Long-term functional and quality of live assessment following post-traumatic distraction osteogenesis of the lower limb. Strategies Trauma Limb Reconstr 2009;4:107-12.</li> [Google Scholar] [PubMed]
- 3. <li>Spiegelberg B, Parratt T, Dheerendra SK, Khan WS, Jennings R, Marsh D. Ilizarov principles of deformity correction. Ann R Coll Surg Engl 2010;92:101-5.</li> [Google Scholar] [PubMed]
- 4. <li>Zhao D, Wang Y, Han D. Periosteal distraction osteogenesis: An effective method for bone regeneration. Biomed Res Int 2016;2016:2075317.</li> [Google Scholar] [PubMed]
- 5. <li>Kenawey M, Krettek C, Liodakis E, Meller R, Hankemeier S. Insufficient bone regenerate after intramedullary femoral lengthening: Risk factors and classification system. Clin Orthop Relat Res 2011;469:264-73.</li> [Google Scholar] [PubMed]
- 6. <li>Cascio BM, Thomas KA, Wilson SC. A mechanical comparison and review of transverse, step-cut, and sigmoid osteotomies. Clin Orthop Relat Res 2003;411:296-304.</li> [Google Scholar] [PubMed]
- 7. <li>Brumat P, Mihalič R, Kovač S, Trebše R. Acute femoral lengthening in adults using step-cut osteotomy, traction table, and proximal femoral locking plate fixation: Surgical technique and report of three cases. Indian J Orthop 2022;56:559-65.</li> [Google Scholar] [PubMed]
- 8. <li>Sabry AO, Galal S, Menshawey R, Menshawey E, Hegazy M, Farahat M, et al. Femoral lengthening in children with congenital femoral deficiency: a systematic review. JBJS Rev. 2024;12(8):</li> [Google Scholar] [PubMed]
- 9. <li>De Bastiani G, Aldegheri R, Renzi-Brivio L, Trivella G. Limb lengthening by callus distraction (callotasis). J Pediatr Orthop 1987;7:129-34.</li> [Google Scholar] [PubMed]
- 10. <li>Pediatric Orthopaedic Society of North America (POSNA). Limb Lengthening Techniques: Study Guide. Oakbrook Terrace, IL: Pediatric Orthopaedic Society of North America. Available from: <a href="https://posna.org/physician-education/study-guide/limb-lengthening-techniques">https://posna.org/physician-education/study-guide/limb-lengthening-techniques</a> [Last accessed on 2025 Nov 25].</li> [Google Scholar] [PubMed]
- 11. <li>Pan Y, Chen Y. Greater trochanteric osteotomy and subtrochanteric osteotomy in primary/revision total hip arthroplasty. Front Surg 2023;10:1103689.</li> [Google Scholar] [PubMed]
- 12. <li>Talwar J, Agarwal S, Agarwal S, Krishna LG, Rustagi A. Step-cut subtrochanteric osteotomy combined with total hip arthroplasty for neglected traumatic hip dislocations. Clin Orthop Surg 2022;14:205-12.</li> [Google Scholar] [PubMed]
- 13. <li>Kılıçoğlu Öİ, Türker M, Akgül T, Yazıcıoğlu Ö. Cementless total hip arthroplasty with modified oblique femoral shortening osteotomy in Crowe type IV congenital hip dislocation. J Arthroplasty 2013;28:117-25 [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Late-onset Legg-Calvé-Perthes Disease Treated with Varus Derotation Femoral Osteotomy: A Case Report
April 1, 2026 Late-onset Legg-Calvé-Perthes Disease Treated with Varus Derotation Femoral Osteotomy: A Case Report August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report
August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report August 1, 2026 Serendipitous Healing of a Congenital Pseudoarthrosis of the Clavicle Following Acute Injury: A Case Report
August 1, 2026 Serendipitous Healing of a Congenital Pseudoarthrosis of the Clavicle Following Acute Injury: A Case Report July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis
July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis