
Single stage, open retrieval of loose bodies by combined approach with radical synovectomy decreases the incidence of recurrence in extensive synovial chondromatosis.
Dr. Abhishek Kumar Rai, Department of Orthopaedics, Seth GS Medical College and KEM Hospital, Mumbai, Maharashtra, India. E-mail: abhishek110891@gmail.com
Abstract
Introduction: Synovial chondromatosis of the knee is an unusual, rare, benign metaplastic neoplasm of the synovium, characterized by the formation of focal cartilaginous nodules in the synovium. It predominantly involves the anterior compartment of knee and extensive, disseminated involvement is rarely reported. Diagnosis is usually established with clinicoradiological imaging and confirmed by histology. The paucity of literature on the management of synovial chondromatosis puts an orthopedician in dilemma regarding the optimal surgical intervention.
Case Report: We report a case of 50-year-old male who presented with severe pain and swelling in his left knee associated with functional incapacitation. Magnetic resonance imaging demonstrated diffuse proliferation of synovium with mild effusion displaying multiple, disseminated calcific nodules. We managed the case by open removal of loose bodies and radical synovectomy through combined anterior and posterior approach. At 4 years follow-up, there are no clinical or radiological signs of recurrence.
Conclusion: Extensive involvement of the knee with calcific nodules is extremely rare. Treatment is controversial which usually includes removal of loose bodies combined with an open or arthroscopic synovectomy. Our case report recommends single stage, open retrieval of loose bodies combined with radical synovectomy to decrease the incidence of recurrence in extensive synovial chondromatosis. To the best of our knowledge, disseminated synovial chondromatosis of the knee, managed by open, combined approach, has been reported only once in the literature.
Keywords: Synovial chondromatosis, open synovectomy, combined approach, knee joint.
Synovial chondromatosis is an extremely rare, idiopathic, benign disorder of synovium [1]. First described by Leannac, synovial chondromatosis is the result of metaplasia, transforming the subsynovial membrane of joint, bursae, and nerve sheath into hyaline cartilaginous nodule [2]. These cartilaginous nodules often detach to form intra-articular loose bodies. Synovial fluid nourishes the nodules to grow in size. The lesion commonly affects a single joint, knee being the most common followed by hip [3]. Males are commonly affected, predominantly the third to fifth decade of life [3]. Synovial chondromatosis is usually restricted to the anterior compartment of knee which includes anterior fat pad and suprapatellar pouch [4]. Involvement of posterior compartment is a rare entity [4]. Few cases of disseminated generalized synovial chondromatosis have been described in the literature. The disease is characterized by non-specific symptoms of pain, swelling, restricted range of motion, locking, giving away, and crepitus [5]. As the symptoms are non-specific and insidious in onset, the diagnosis is usually delayed. Synovial chondromatosis is diagnosed clinicoradiologically and confirmed after histopathological examination. We report a case of disseminated synovial chondromatosis of knee, managed by open radical synovectomy.
The patient was a 50-year-old man who presented to our outpatient department with the complaints of pain and swelling in the left knee associated with functional incapacity (Fig. 1). The pain was insidious in onset, gradually progressed over a year and aggravated by activities of daily living and relieved by rest. The patient complained of locking experiences of the left knee since the past 3 months. The medical and surgical history is not significant. On examination, the knee was diffusely swollen with restricted range of motion 0° to 110°. The medial and lateral joint line tenderness was positive with patellofem oral joint crepitation. McMurray circumduction test was positive. There was no sagittal or coronal plane instability. The overlying skin over the knee was normal with marked muscle wasting of left thigh. Routine hematological investigations were within normal limits. Radiographs showed multiple, generalized calcified nodules in and around knee joint (Fig. 2).
The pain was insidious in onset, gradually progressed over a year and aggravated by activities of daily living and relieved by rest. The patient complained of locking experiences of the left knee since the past 3 months. The medical and surgical history is not significant. On examination, the knee was diffusely swollen with restricted range of motion 0° to 110°. The medial and lateral joint line tenderness was positive with patellofem oral joint crepitation. McMurray circumduction test was positive. There was no sagittal or coronal plane instability. The overlying skin over the knee was normal with marked muscle wasting of left thigh. Routine hematological investigations were within normal limits. Radiographs showed multiple, generalized calcified nodules in and around knee joint (Fig. 2). Magnetic resonance imaging (MRI) demonstrated diffuse proliferation of synovium with mild effusion displaying multiple nodules with intermediate to high signal intensity suggesting calcific nature (Fig. 3).
Magnetic resonance imaging (MRI) demonstrated diffuse proliferation of synovium with mild effusion displaying multiple nodules with intermediate to high signal intensity suggesting calcific nature (Fig. 3).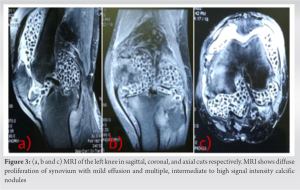 The clinicoradiological correlation suggested the diagnosis of synovial chondromatosis. The management includes removal of loose bodies along with radical excision of hypertrophied synovium. Open or arthroscopic synovectomy is bit controversial. Arthroscopic synovectomy allows the vital structures to be accurately identified and decreases the associated morbidity. Removal of loose bodies in the anterior compartment by arthroscopy is relatively easier. However, arthroscopic radical synovectomy in cases of generalized knee involvement or predominant posterior involvement is technically challenging and carries the risk of damage to the neurovascular structures. Considering the circumferential involvement of knee, we planned a single stage, open radical synovectomy through a combined approach. The patient was positioned laterally under tourniquet. A standard anterior midline approach was used with a median parapatellar approach. Multiple white colored loose bodies were found embedded inside the hypertrophied synovium and few lying loosely in the joint. The synovium was excised and the loose bodies were taken out. After clearing the anterior pathological structures, we took a lazy “S”-shaped incision posteriorly in the popliteal fossa. The clinical picture posteriorly was similar, with hypertrophied synovium and multiple loose bodies. The posterior vital structures were dissected meticulously and the synovium was radically excised (Fig. 4).
The clinicoradiological correlation suggested the diagnosis of synovial chondromatosis. The management includes removal of loose bodies along with radical excision of hypertrophied synovium. Open or arthroscopic synovectomy is bit controversial. Arthroscopic synovectomy allows the vital structures to be accurately identified and decreases the associated morbidity. Removal of loose bodies in the anterior compartment by arthroscopy is relatively easier. However, arthroscopic radical synovectomy in cases of generalized knee involvement or predominant posterior involvement is technically challenging and carries the risk of damage to the neurovascular structures. Considering the circumferential involvement of knee, we planned a single stage, open radical synovectomy through a combined approach. The patient was positioned laterally under tourniquet. A standard anterior midline approach was used with a median parapatellar approach. Multiple white colored loose bodies were found embedded inside the hypertrophied synovium and few lying loosely in the joint. The synovium was excised and the loose bodies were taken out. After clearing the anterior pathological structures, we took a lazy “S”-shaped incision posteriorly in the popliteal fossa. The clinical picture posteriorly was similar, with hypertrophied synovium and multiple loose bodies. The posterior vital structures were dissected meticulously and the synovium was radically excised (Fig. 4). The hypertrophied synovium and the loose bodies were sent for histological confirmation. Histopathological examination revealed well-demarcated, disorganized cartilaginous nodules with hypertrophied synovium permeating in between. The nodules were variable calcified and ossified. The size and shape of cartilaginous nodules varied significantly. The histological findings confirmed the diagnosis of synovial chondromatosis. The patient was mobilized full weight-bearing on a walker for 2 weeks till suture removal. The patient followed the standard physiotherapy protocols for the strengthening of quadriceps and hamstrings and to gain range of motion. Three months after surgery, the patient regained full range of motion with no pain while doing daily activities. The patient was last reviewed at 4 years follow-up with no clinicoradiological signs of recurrence (Fig. 5).
The hypertrophied synovium and the loose bodies were sent for histological confirmation. Histopathological examination revealed well-demarcated, disorganized cartilaginous nodules with hypertrophied synovium permeating in between. The nodules were variable calcified and ossified. The size and shape of cartilaginous nodules varied significantly. The histological findings confirmed the diagnosis of synovial chondromatosis. The patient was mobilized full weight-bearing on a walker for 2 weeks till suture removal. The patient followed the standard physiotherapy protocols for the strengthening of quadriceps and hamstrings and to gain range of motion. Three months after surgery, the patient regained full range of motion with no pain while doing daily activities. The patient was last reviewed at 4 years follow-up with no clinicoradiological signs of recurrence (Fig. 5).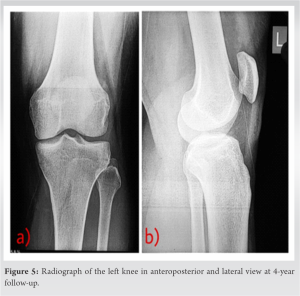
Synovial chondromatosis is a rare, benign condition characterized by the metaplastic transformation of the synovium to cartilaginous nodules [6]. The clinical presentation depends on the extent of synovial involvement. The typical symptoms include pain, swelling, crepitus, and restricted range of motion [6]. Prompt diagnosis and early treatment is crucial as the chronic conditions may lead to degeneration of the knee joint. Although synovial chondromatosis is usually benign, malignant transformation to chondrosarcoma has been reported in the literature [7]. Considering the rare occurrence of this entity, a high index of suspicion is required to diagnose clinically. Standard radiographs typically demonstrate loose bodies, if they are mineralized. They are difficult to be interpreted if the loose bodies are unmineralized. Computed tomography may be required in such cases to detect the ongoing calcification. MRI is the investigation of choice for early detection and to outline the extent of soft-tissue involvement. Treatment of synovial chondromatosis includes retrieval of loose bodies combined either with open or arthroscopic radical synovectomy [7]. The recurrence rate after loose body removal alone is high. Thus, synovectomy has been recommended to avoid recurrence [8]. As per the studies, chemotherapy and radiotherapy have no role in the management. With the recent advancement, arthroscopic removal is the recent most treatment modality to decrease the post-operative morbidity [9]. However, in generalized involvement of the knee, chances of neurovascular injury are more and warrant open retrieval of loose bodies [10]. Singh et al. managed a similar case of a 30-year-old female with extensive synovial chondromatosis of the knee by open synovectomy using combined approach [8]. A thorough search of PubMed suggests that there is fewer than a couple of reports on combined open approach for the management of extensive generalize dsynovial chondromatosis. The limitation of our study is a short follow-up of 4 years to comment on recurrence after the procedure.
Generalized synovial chondromatosis of knee is an extremely rare entity. Open retrieval of loose bodies combined with synovectomy helps in better eradication of the disease with less chances of recurrence. Our case report recommends a single stage, combined anterior and posterior approach to be preferred in extensive synovial chondromatosis.
Extensive synovial chondromatosis of knee is rare in literature. Single stage, open or arthroscopic removal of loose bodies is the preferred management modality.
References
- 1.Filho JS, Garms E, De Carvalho RT, Sayum J, Matsuda MM, Cohen M. Synovial chondromatosis of the knee: Case report. Rev Bras Ortop 2015;46:605-6. [Google Scholar | PubMed]
- 2.Dorfmann H, De Bie B, Bonvarlet JP, Boyer T. Arthroscopic treatment of synovial chondromatosis of the knee. Arthroscopy 1989;5:48-51 [Google Scholar | PubMed]
- 3.Jesalpura JP, Chung HW, Patnaik S, Choi HW, Kim JI, Nha KW. Arthroscopic treatment of localized synovial chondromatosis of the posterior knee joint. Orthopedics 2010;33:49. [Google Scholar | PubMed]
- 4.Coolican MR, Dandy DJ. Arthroscopic management of synovial chondromatosis of the knee. Findings and results in 18 cases. J Bone Joint Surg Br 1989;71:498-500. [Google Scholar | PubMed]
- 5.Wengle LJ, Hauer TM, Chang JS, Theodoropoulos J. Systematic arthroscopic treatment of synovial chondromatosis of the knee. Arthrosc Tech 2021;10:e2265-70. [Google Scholar | PubMed]
- 6.Lasmar NP, Vieira RB, Rosa JD, Lasmar RC, Scarpa AC. Synovial chondromatosis. Rev Bras Ortop 2015;45:490-2. [Google Scholar | PubMed]
- 7.Neumann JA, Garrigues GE, Brigman BE, Eward WC. Synovial chondromatosis. JBJS Rev 2016;4:e2. [Google Scholar | PubMed]
- 8.Singh S, Neelakandan K, Sood C, Krishnan J. Disseminated synovial chondromatosis of the knee treated by open radical synovectomy using combined anterior and posterior approaches. J Clin Orthop Trauma 2014;5:157-60. [Google Scholar | PubMed]
- 9.Fuerst M, Zustin J, Lohmann C, Rüther W. Synovial chondromatosis. Orthopade 2009;38:511-9. [Google Scholar | PubMed]
- 10.Vališ P, Vyskočil R. Generalised form of synovial chondromatosis of the knee joint. Acta Chir Orthop Traumatol Cech 2016;83:198-201. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2025 Surgical Management of Knee Synovial Chondromatosis through Posterior Open Synovectomy: A Unique Case Report
October 1, 2025 Surgical Management of Knee Synovial Chondromatosis through Posterior Open Synovectomy: A Unique Case Report August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report
August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report June 1, 2026 Secondary Synovial Chondromatosis of the Shoulder Associated with Rotator Cuff Tear: Diagnostic Challenge and Arthroscopic Management – A Case Report
June 1, 2026 Secondary Synovial Chondromatosis of the Shoulder Associated with Rotator Cuff Tear: Diagnostic Challenge and Arthroscopic Management – A Case Report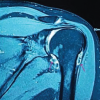 April 1, 2026 Understanding Synovial Chondromatosis: A Rare Cause of Shoulder Impingement
April 1, 2026 Understanding Synovial Chondromatosis: A Rare Cause of Shoulder Impingement