
Magnetic resonance imaging is crucial for diagnosing rare cases of shoulder synovial
Dr. S R Hemand, Department of Arthroscopy and Sports Medicine, Sri Ramachandra Institute of Higher Education and Research, Porur, Chennai, Tamil Nadu, India. E-mail: hemandsr3211@gmail.com
Abstract
Introduction: Synovial chondromatosis (SC) is a rare benign disorder of the synovium characterised by cartilaginous metaplasia and intra-articular loose body formation. It commonly affects large joints such as the knee, whereas shoulder involvement is extremely rare and is often misdiagnosed. We present a rare case of shoulder SC in an elderly female, highlighting the diagnostic challenges and arthroscopic surgical management.
Case Report: A 64-year-old female presented with an alleged history of a fall on her outstretched hand 18 months back. Following the trauma, the patient complained of right shoulder pain and later restriction of movement. Examination revealed restriction of movement with crepitus and positive impingement signs. Radiographs were normal. Magnetic resonance imaging (MRI) revealed multiple intra-articular loose bodies with a supraspinatus tear. She underwent arthroscopic rotator cuff repair, loose body removal, and synovectomy. Histopathology confirmed SC. Post-operative rehabilitation led to satisfactory recovery.
Conclusion: This case highlights the occurrence or incidence of SC in long-standing rotator cuff tears and also emphasises the importance of considering SC in the differential diagnosis of chronic shoulder pain, especially when radiographs are inconclusive. MRI plays a pivotal role in early diagnosis, and arthroscopic surgery provides effective management with excellent outcomes.
Keywords: Shoulder joint, synovial chondromatosis, arthroscopy, loose bodies, rotator cuff tear.
Synovial chondromatosis (SC) is an uncommon benign proliferative disorder of the synovium characterised by cartilaginous metaplasia and the formation of multiple intra-articular loose bodies [1]. First described by Reichel in 1900 [2] and later comprehensively defined by Jaffe in 1958, the condition most frequently involves large weight-bearing joints such as the knee and hip, whereas shoulder involvement is relatively rare, accounting for <5% of reported cases [3,4,5]. SC may occur as either a primary idiopathic process or as a secondary phenomenon following pre-existing intra-articular pathology [6,7]. Secondary SC develops in response to chronic mechanical or degenerative joint disorders, including osteoarthritis, trauma, osteonecrosis, inflammatory arthropathy, and rotator cuff disease. In the shoulder joint, persistent rotator cuff insufficiency may alter glenohumeral biomechanics, leading to synovial irritation, chondral degeneration, and subsequent metaplastic transformation of subsynovial mesenchymal cells, ultimately resulting in loose body formation [5]. Clinically, patients with shoulder SC typically present with insidious onset of shoulder pain; swelling; mechanical symptoms such as locking or catching; and progressive restriction of motion. In cases associated with rotator cuff tears, symptoms may overlap with cuff-related shoulder dysfunction, impingement syndrome, or degenerative joint disease, often contributing to delayed or missed diagnosis [5]. Long-standing intra-articular loose bodies may further exacerbate articular cartilage wear and accelerate secondary osteoarthritic changes [3]. Radiological evaluation is essential for diagnosis; however, plain radiographs may be inconclusive in early stages due to the presence of non-calcified cartilaginous loose bodies [8,9]. Magnetic resonance imaging (MRI) is the imaging modality of choice as it enables detection of both mineralised and non-mineralised loose bodies, assessment of synovial proliferation, evaluation of rotator cuff integrity, and identification of associated intra-articular or peri-articular pathology [5,10]. We present a case of SC in an elderly female with a rotator cuff tear managed arthroscopically.
A 64-year-old female presented to the outpatient department with complaints of an 18-month history of right shoulder pain following a slip and fall on her outstretched hand. The pain was acute in onset, was described as a dull ache, and was relieved by analgesics. Initially, the patient experienced pain and difficulty with shoulder abduction. Presently, she has had difficulty reaching her back, along with crepitus, for the past 3 months. No constitutional symptoms were present. No other comorbidities were present. Activities of daily living were affected, such as combing hair and lifting weights. The Disabilities of the Arm, Shoulder, and Hand (DASH) score was 65.8%. On clinical examination, tenderness was present over the greater tuberosity and anterior joint line, the active range of motion was restricted, and the passive range of motion was full; however, mechanical blocking was present, and provocative tests such as the drop arm test and test for impingement were positive. These findings suggested an underlying rotator cuff pathology; however, the mechanical symptoms raised suspicion of an intra-articular pathology [5]. Her X-ray radiographs were normal (Fig. 1).
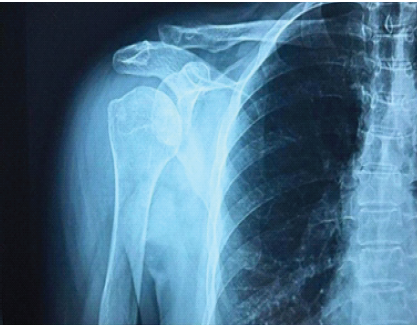
Figure 1: X-ray shoulder anteroposterior view.
An MRI of the right shoulder was done (Figs. 2 and 3), which showed moderate joint effusion with multiple chondral loose bodies, moderate fluid in the subacromial, subdeltoid, and subcoracoid bursae with multiple chondral loose bodies, and a full-thickness tear of the supraspinatus [9].
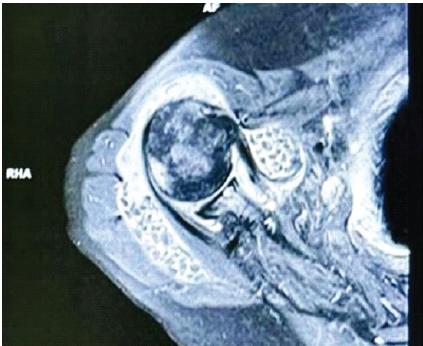
Figure 2: Magnetic resonance imaging T2 axial cut, showing multiple chondral loose bodies and subacromial effusion.

Figure 3: Magnetic resonance imaging T2 coronal cut, showing joint effusion and supraspinatus tear.
The MRI findings were consistent with SC involving both the glenohumeral joint and surrounding bursae, along with a concomitant rotator cuff tear. The presence of loose bodies in multiple compartments emphasised the importance of thorough arthroscopic evaluation to avoid residual disease. Given the patient’s functional limitation, high DASH score, and imaging findings, surgical intervention was planned. Arthroscopic examination of the glenohumeral joint demonstrated (Fig. 4) multiple smooth, pearly white cartilaginous loose bodies of varying sizes scattered within the joint cavity and synovial recesses.
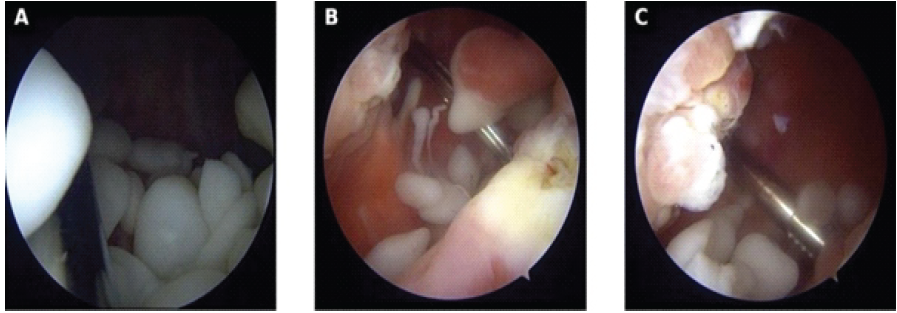
Figure 4: Arthroscopic intra-articular images demonstrating (a) multiple smooth-surfaced pearly white cartilaginous loose bodies of variable size within the joint cavity, without evidence of active villous or nodular synovial proliferation; (b) probing and mobilization of mature osteochondral loose bodies from the surrounding synovial recesses using an arthroscopic shaver, suggestive of detached intra-articular fragments rather than primary synovial metaplastic nodules; and (c) clustering of numerous free-floating rounded loose bodies within the dependent portion of the joint space.
The fragments appeared well-formed and rounded, suggestive of mature osteochondral loose bodies in a mechanically altered intra-articular environment, with no significant active synovial proliferation noted. Systematic probing and retrieval enabled the removal of numerous free-floating nodules. During joint irrigation (Fig. 5), profuse extrusion of several discrete loose bodies through the arthroscopic portal was observed, indicating a high intra-articular loose body load consistent with secondary SC associated with underlying rotator cuff pathology.
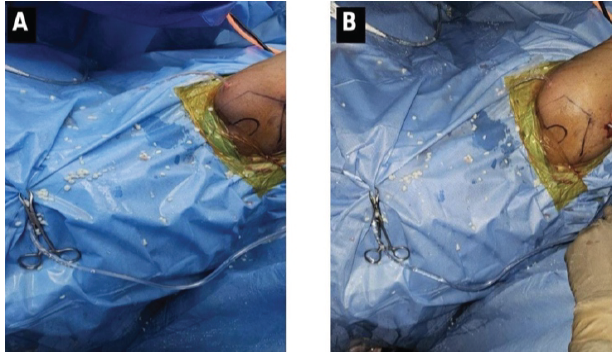
Figure-5: Arthroscopic irrigation demonstrating extrusion of multiple loose bodies through the portal.
The patient was treated with right shoulder arthroscopic (1) rotator cuff repair (2), multiple loose body removals (3), and synovectomy. Arthroscopy allowed complete visualisation of the glenohumeral joint, subacromial space, and surrounding bursae, facilitating comprehensive removal of loose bodies and hypertrophic synovium. Rotator cuff repair done, rotator cuff fixed to the humeral head using one 5.5 mm double-loaded anchor (medial row) and one 5.5 mm knotless anchor (lateral row), integrity checked and found to be satisfactory. Loose bodies along with synovial tissue were sent for biopsy, culture, and Gene Xpert. Synovial fluid was sent for synovial fluid analysis. This step was crucial in excluding infectious and inflammatory aetiologies, particularly tuberculosis, which can mimic synovial proliferative disorders in endemic regions. In the immediate post-operative period, the patient was managed with a protective rehabilitation protocol due to concomitant arthroscopic rotator cuff repair. Shoulder range-of-motion exercises were restricted to protect tendon healing and minimise mechanical stress at the repair site; otherwise, early mobilisation would have been initiated from the day of surgery. During this phase, distal joint mobility was maintained through active-assisted elbow movements, active wrist and finger exercises, and gentle cervical range-of-motion exercises to preserve circulation, prevent stiffness, and support early functional recovery while safeguarding the repaired rotator cuff. Histopathological examination revealed (Fig. 6) multiple well-circumscribed lobulated nodules of mature hyaline cartilage within synovial tissue, showing a relatively hypocellular chondroid matrix with features of matrix maturation, smooth rounded peripheral contours with concentric lamination, and absence of cytological atypia or mitotic activity, findings consistent with secondary SC and excluding malignant transformation [2].
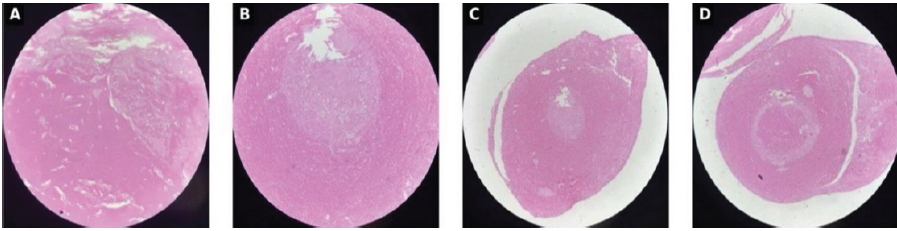
Figure-6:Histopathological examination showing lobulated hyaline cartilage nodules consistent with synovial chondromatosis.
After 14 days, shoulder range-of-motion exercises started as tolerable; shoulder isometrics and neck stretches are advised. At 1-month post-operative follow-up, the DASH score was 53%, with shoulder abduction up to 90°. At the 3-month post-operative review, full shoulder range of motion was achieved, and the DASH score was 17.3%. At the 1-year post-operative review, there were no symptoms of disease recurrence.
SC is aetiologically classified into primary (idiopathic metaplastic) and secondary forms, with the latter occurring in association with pre-existing joint abnormalities, including trauma, degenerative joint disease, inflammatory arthropathy, osteonecrosis, and rotator cuff pathology [6,7]. In older individuals, secondary SC represents the more plausible pathogenic mechanism due to chronic mechanical and degenerative alterations within the joint environment. The present case illustrates a typical evolution of secondary disease, wherein a preceding traumatic episode was followed by persistent shoulder pain and subsequent progressive restriction of motion. Rotator cuff insufficiency is known to disrupt normal glenohumeral force coupling and joint kinematics, resulting in repetitive synovial irritation, chondral wear, and eventual chondroid metaplasia [1,6,7]. Over time, these metaplastic foci may detach to form multiple intra-articular loose bodies, producing mechanical symptoms and accelerating secondary degenerative changes. This pathomechanical sequence provides a rational explanation for the delayed onset of stiffness and functional limitation observed in our patient. Diagnosis of shoulder SC is frequently challenging due to its non-specific clinical presentation and overlap with more prevalent conditions such as rotator cuff tear, arthropathy, or adhesive capsulitis [5]. Conventional radiographs may remain normal in early stages because non-mineralised cartilaginous loose bodies are radiolucent [9]. This limitation was evident in the present case, where plain radiography failed to demonstrate pathology despite persistent symptoms. MRI, therefore, assumes critical diagnostic importance, enabling accurate visualisation of both calcified and non-calcified loose bodies, synovial proliferation, and coexisting intra-articular lesions. MRI thus serves not only as a diagnostic tool but also as a pre-operative roadmap, facilitating comprehensive surgical planning. Surgical management remains the definitive treatment, with the principal objectives being complete loose body removal, synovectomy, and simultaneous correction of associated structural pathology [11,12]. Arthroscopic intervention has emerged as the preferred treatment modality in shoulder SC due to its superior visualisation of both glenohumeral and subacromial compartments, ability to achieve thorough clearance of loose bodies, and facilitation of concurrent rotator cuff repair when indicated. Furthermore, the minimally invasive nature of arthroscopy contributes to reduced post-operative morbidity, earlier initiation of rehabilitation, and improved functional recovery. Similar favourable surgical outcomes following operative management of synovial osteochondromatosis have been previously reported in the literature [11]. SC of the shoulder is rare; however, case reports by Milgram and Boyd describe its occurrence in young, active individuals, typically as primary disease in otherwise normal joints [6]. In contrast, our case demonstrates SC arising in a neglected rotator cuff tear, suggesting a rare secondary aetiology due to chronic mechanical insult and synovial irritation. This underscores the importance of timely management of rotator cuff pathology to prevent such atypical intra-articular sequelae. Primary SC is associated with a relatively higher risk of recurrence due to the continued synovial metaplastic activity, even after the removal of loose bodies, whereas secondary SC is associated with comparatively lower rates of recurrence, provided the intra-articular loose bodies are adequately removed, and the underlying cause of joint pathology is appropriately addressed [7]. Recognition of this rare yet treatable condition is essential to prevent prolonged disability and progression of secondary degenerative joint changes.
Limitations and follow-up:
Our case report is limited by a short follow-up period, and a longer follow-up is required to properly assess the outcomes, including recurrence and the rare possibility of malignant transformation. Unlike primary SC, which has a greater propensity for recurrence due to persistent synovial metaplastic activity, secondary SC, as in our case, has a comparatively lower risk of recurrence, especially when the associated mechanical pathology, i.e., the rotator cuff tear, has been properly managed. However, a longer follow-up is advised to detect early signs of recurrence, particularly in cases of extensive synovial involvement and in elderly patients [2,6].
Secondary SC of the shoulder is a rare sequela of underlying intra-articular pathology, such as rotator cuff injury, and may present with persistent pain, mechanical symptoms, and normal early radiographs, leading to diagnostic delays. MRI is essential for early detection and assessment of associated structural lesions. Arthroscopic loose body removal with synovectomy and concurrent treatment of rotator cuff pathology provides effective symptom relief, facilitates early rehabilitation, and represents the preferred management strategy to prevent progressive degenerative joint changes.
Shoulder SC, though rare, should be suspected in patients with persistent shoulder pain and mechanical symptoms even when radiographs are normal. MRI is crucial for diagnosis, and arthroscopic surgery provides definitive treatment with excellent outcomes.
References
- 1. Maurice H, Crone M, Watt I. Synovial chondromatosis. J Bone Joint Surg Br 1988;70:807-11. [Google Scholar] [PubMed]
- 2. Reichel H. On a peculiar cartilaginous neoplasm in joints. Arch Klin Chir 1900;62:779-84. [Google Scholar] [PubMed]
- 3. Bloom R, Pattinson J. Synovial chondromatosis of the shoulder. J Bone Joint Surg Br 1965;47:229-33. [Google Scholar] [PubMed]
- 4. Bhamra JS, Kulkarni R, Tambe AD. Primary synovial chondromatosis of the shoulder. Orthop Rev (Pavia) 2012;4:e30. [Google Scholar] [PubMed]
- 5. Neumann JA, Garrigues GE, Brigman BE, Eward WC. Synovial chondromatosis of the shoulder. J Shoulder Elbow Surg 2014;23:e179-88. [Google Scholar] [PubMed]
- 6. Milgram JW. Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;59:792-801. [Google Scholar] [PubMed]
- 7. Villacin AB, Brigham LN, Bullough PG. Primary and secondary synovial chondrometaplasia: Histopathologic and clinicoradiologic differences. Hum Pathol 1979;10:439-51. [Google Scholar] [PubMed]
- 8. Lim SJ, Chung HW, Choi YL, Park YS, Moon YW, Seo JG. Operative treatment of primary synovial osteochondromatosis of the hip. J Bone Joint Surg Am 2006;88:2456-64. [Google Scholar] [PubMed]
- 9. Murphey MD, Vidal JA, Fanburg-Smith JC, Gajewski DA. Imaging of synovial chondromatosis with radiologic-pathologic correlation. Radiographics 2007;27:1465-88. [Google Scholar] [PubMed]
- 10. Wagner ER, Houdek MT, Schleck CD, Harmsen WS, Sanchez-Sotelo J, Cofield RH, et al. Arthroscopic management of synovial chondromatosis of the shoulder. Arthroscopy 2017;33:912-9. [Google Scholar] [PubMed]
- 11. Ogilvie-Harris DJ, Saleh K. Synovial chondromatosis: Treatment by arthroscopy. Arthroscopy 1994;10:166-70. [Google Scholar] [PubMed]
- 12. Davis RI, Hamilton A, Biggart JD. Primary synovial chondromatosis: A clinicopathologic review and assessment of malignant potential. Hum Pathol 1998;29:683-8. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report
August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report October 1, 2025 Non-calcified Synovial Chondromatosis Masquerading as a Posterior Knee Cyst: A Diagnostic Challenge
October 1, 2025 Non-calcified Synovial Chondromatosis Masquerading as a Posterior Knee Cyst: A Diagnostic Challenge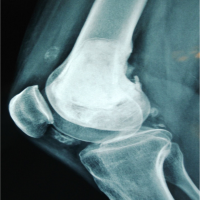 September 1, 2024 Giant Cell Tumor as a Rare Cause of Loose Bodies in the Knee Joint – A Case Report
September 1, 2024 Giant Cell Tumor as a Rare Cause of Loose Bodies in the Knee Joint – A Case Report January 10, 2021 Diagnosis and Arthroscopic Treatment of Synovial Chondromatosis of Glenohumeral Joint: A Case Report
January 10, 2021 Diagnosis and Arthroscopic Treatment of Synovial Chondromatosis of Glenohumeral Joint: A Case Report