
Osteochondroma is the most common benign tumor of the bone, Surgical excision of osteochondroma arising from the scapula using muscle splitting in line with muscle fibers yielded good clinical outcomes.
Dr. Laila M Alsabbagh, Department of Orthopedic, College of Medicine, King Saud University, Riyadh, Saudi Arabia. E-mail: Lailamalsabbagh@gmail.com
Abstract
Introduction: Osteochondromas are the most common benign lesions of the bone. They usually affect flat bones such as the scapula.
Case Report: We report a case of a left-handed 22-year-old male with no previous medical history, who came to the orthopedic outpatient clinic complaining of pain in the right shoulder, snapping, poor cosmetic look, and limited range of motion. Magnetic resonance imaging revealed an osteochondroma of the scapula. The tumor was surgically excised using a muscle splitting technique in line with the muscle fibers. Histopathological evaluation of the excised tumor confirmed the diagnosis of an osteochondroma.
Conclusion: Surgical excision of the osteochondroma using muscle splitting in line with the muscle fibers gave good results in terms of patient satisfaction and cosmetic appearance. Delayed diagnosis and management may increase the risk of symptoms such as snapping or winging of the scapula.
Keywords: Osteochondroma, snapping, winging, benign lesions, scapula, pain.
Osteochondromas are benign lesions originating from the metaphyseal aspect of the bone [1]. They are the most common benign lesion affecting the bone (35–46%) [2]. The most common bones to be affected are long bones (e.g., the femur, proximal humerus, and tibia). It affects flat bones such as the scapula, in only 3–4% of cases [3]. Most osteochondromas are solitary exostoses, but they could be part of syndrome such as the hereditary multiple exostosis syndrome, an autosomal dominant disorder that is defined as the formation of multiple cartilaginous osteochondromas in immature bones [4,5]. Osteochondromas affecting the scapula can be located ventrally or dorsally [6].
These lesions are usually asymptomatic, but may cause pain, snapping of the scapula, and in some cases, winging of the scapula due to mass effect [6]. The following case describes excision of a ventral osteochondroma causing shoulder and neck pain and snapping scapula syndrome, using a minimal incision technique.
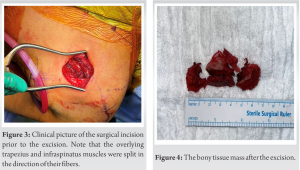
We report a case of a left-handed 22-year-old male with no prior medical history who attended our institution’s orthopedic surgery outpatient clinics complaining of the right shoulder pain, snapping, poor cosmetic appearance, and limited range of motion (ROM). At the time of consult, he was a student and was interested in volleyball. Symptoms began 2 years earlier. Asymmetry of the shoulders was noticed by his relatives. Pain and limitation in ROM restricted his participation in sports. On examination, asymmetrical appearance of scapulae was noted, with prominence of the right scapula, resembling winging of the scapula. No tenderness was elicited. ROM was restricted by at least 20° in internal and external rotation, and abduction, and by 30° in forward flexion of the right shoulder when compared to left. Integrity of rotator cuff tendons as well as biceps were preserved with respect to their testing. Ipsilateral elbow, wrist, and hand examinations were unremarkable. Neurovascular examination was unremarkable. No apparent abnormalities were detected on plain radiographs and further advanced imaging with computed tomography scan was performed. A right ventral bony mass was detected measuring 1.8 × 2 cm (Fig. 1). 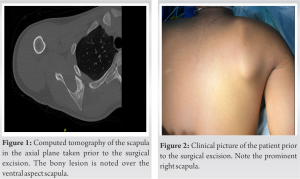
 Analgesia was prescribed for the patient as required and was referred to physical therapy. Pre-operative magnetic resonance imaging also done to delineate the mass and its cartilaginous cap. On follow-up at 3 months, the patient’s symptoms had not improved, and surgical intervention was advised. He underwent minimally invasive open surgical excision. Patient was discharged on post-operative day one and was then followed up at 2 and 6 months. The diagnosis of osteochondroma was confirmed by histopathology (Fig. 6).
Analgesia was prescribed for the patient as required and was referred to physical therapy. Pre-operative magnetic resonance imaging also done to delineate the mass and its cartilaginous cap. On follow-up at 3 months, the patient’s symptoms had not improved, and surgical intervention was advised. He underwent minimally invasive open surgical excision. Patient was discharged on post-operative day one and was then followed up at 2 and 6 months. The diagnosis of osteochondroma was confirmed by histopathology (Fig. 6).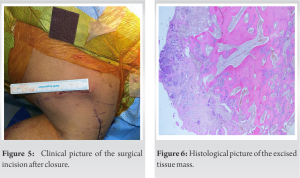
The patient was placed in prone position after general anesthesia and intubation. The entire left upper limb and the ipsilateral thoracic back up to the spinous process was subjected to asepsis and antisepsis. The hand was inserted through the square drape which covered all sides of the scapula and it was placed over his back in the chicken wing position. The medial border of the scapula was prominent and the edge of the ventral scapular osteochondroma was palpable (Fig. 2). Marking of the osteochondroma was done over the middle part of medial border of the scapula. A 5 cm skin incision was made directly over the medial border of the scapula. The following were done sequentially: Fat was dissected, the trapezius fascia was exposed and incised with a snip, and the trapezius muscle was split in line with its fibers (Fig. 3). The infraspinatus fascia was incised with a snip and the muscle was split in line with its fibers. The medial border of the scapula was exposed and the osteochondroma was adequately visualized. Using an osteotome, the osteochondroma was excised in line with the ventral surface of scapula (Fig. 3). Complete osteotomy was done. No sharp edges were noted from the bed of the osteochondroma. The osteochondroma specimen was sent for histopathology. Thorough irrigation of the wound was done with normal saline. Bone wax was applied over the bed of the osteochondroma to minimize the risk of recurrence. Closure of fascia and then the subcutaneous tissue was done. Meticulous hemostasis applied throughout the procedure. Skin was closed with absorbable sutures in subcuticular fashion and a dressing applied (Fig. 4). Arm sling was applied for pain control for the first 3 days and then active ROM exercises were started under supervision of a physiotherapist.
Outcome
During serial follow-up, the wound healed uneventfully. The patient’s last visit to the clinic was 6-week postoperatively. The patient reported resolution of the pain and crepitations. On examination, the patient demonstrated full shoulder ROM. The patient was advised to undergo strengthening exercises and follow-up to observe any signs or symptoms of recurrence.
Osteochondroma is the most common benign bone lesion, commonly involving the distal femur, proximal tibia, and proximal humerus, accounting for more than 90% of cases [7]. Involvement of the scapula in osteochondroma is relatively rare, comprising 3–4.6% of cases; however, it accounts for almost half of all cases of benign scapular lesions [3]. Most scapular osteochondromas are found in the ventral region of the scapula, accounting for 63% of all cases [8].
The majority of osteochondroma lesions are asymptomatic. Symptomatic cases are commonly related to the site and size of the lesion; the most common symptoms are pain and cosmetic deformity [9]. Likewise, scapular osteochondroma especially ventral osteochondroma of scapula is usually asymptomatic. When symptomatic, patients may complain of chronic pain, shoulder snapping, and winging deformity; in this case, the patient had pain that affected his daily activities and had winging of the scapula [10]. Furthermore, such lesions in flat bones have a significant risk of malignant transformation [9], and surgical excision is the only effective treatment in such cases.
There has been no consensus regarding the best surgical technique for ventral scapula osteochondroma excision, and a few different techniques have been described in the literature. They can be divided into three main groups: muscle-sparing, muscle detachment, and endoscopic-assisted techniques [11]. For this case, we used a muscle-sparing technique. Aalderink et al. described arthroscopic excision in the prone position with the arm internally rotated to the lumbar spine. This technique had excellent outcomes in terms of complete excision, absence of winging, and resolution of snapping. However, this technique is not preferable in potentially malignant lesions due to the risk of spillage into the joint, which decreases the likelihood of limb salvage [12]. The risk of malignant transformation has been estimated at 1–2%, with increasing risk if multiple areas are involved [13].
For this case, we positioned the patient prone with his arm internally rotated such that the ventral aspect of the scapula can be accessed with a minor incision of approximately 5 cm over the medial aspect of the scapula, minimal snip to the trapezius fascia and to the infraspinatus fascia, and with splitting inline fibers of both muscles. We believe this technique would result in a better cosmetic appearance, with a relatively small scar, less risk of tumor spillage in case of malignancy, and equal functional outcome of previously described techniques [3,9,12].
Osteochondromas are considered common benign lesions, but rarely affect the scapula. When they do, the ventral aspect of the scapula is most commonly affected. Usually, they are asymptomatic but can cause pain, restrict the ROM, and cause a cosmetic deformity.
Surgical excision of osteochondroma arising from the scapula using muscle splitting in line with muscle fibers yielded good clinical outcomes in terms of patient satisfaction and cosmetic appearance.
References
- 1.Rameez R, Ul-Hassan M, Kotwal HA, Kangoo KA, Nazir A. Painful Pseudowinging and snapping of scapula due to subscapular osteochondroma: A case report. J Orthop Case Rep 2016;6:96-9. [Google Scholar | PubMed]
- 2.Unni KK, Inwards CY, Dahlin DC. Dhalin’s Bone Tumors: General Aspects and Data on 10,165 Cases. Philadelphia, PA: Lippincott Williams and Wilkins; 2010. [Google Scholar | PubMed]
- 3.Frost NL, Parada SA, Manoso MW, Arrington E, Benfanti P. Scapular osteochondromas treated with surgical excision. Orthopedics 2010;33:804. [Google Scholar | PubMed]
- 4.Heck RK. Benign bone tumours and non-neoplastic conditions simulating bone tumours. In: Campbell Orthopaedics. 11th ed. United States: Mosby; 2007. p. 860. [Google Scholar | PubMed]
- 5.Pérez D, Cano JR, Caballero J, López L. Minimally-invasive resection of a scapular osteochondroma. Interact Cardiovasc Thorac Surg 2011;13:468-70. [Google Scholar | PubMed]
- 6.Nekkanti S, Moogali A, Meka A, Nair M. An unusual presentation of osteochondroma on the dorsal surface of the scapula: A review of two patients. J Orthop Case Rep 2018;8:38-41. [Google Scholar | PubMed]
- 7.Clarke DO, Crichlow A, Christmas M, Vaughan K, Mullings S, Neil I, et al. The unusual osteochondroma: A case of snapping scapula syndrome and review of the literature. Orthop Traumatol Surg Res 2017;103:1295-8. [Google Scholar | PubMed]
- 8.Stevens J, Stirling P, Patton JT. Trapezius-sparing approach to osteochondromas on the ventral surface of the scapula. Tech Shoulder Elbow Surg 2018;19:124-8. [Google Scholar | PubMed]
- 9.Ogawa K, Inokuchi W. Solitary osteochondroma of the ventral scapula associated with large bursa formation and pseudowinging of the scapula: A case report and literature review. Case Rep Orthop 2018;2018:5145642. [Google Scholar | PubMed]
- 10.Ammar A, Abcha O, Zaier A, Bouhajja L, Farah F, Smida M, et al. An unusual cause of shoulder pain: Osteochondroma of ventral scapula (a case report). Pan Afr Med J 2021;39:88. [Google Scholar | PubMed]
- 11.De Haan LJ, Somford MP, van den Borne MP. Surgical treatment of scapular osteochondroma. MOJ Orthop Rheumatol 2017;7:1-3. [Google Scholar | PubMed]
- 12.arthroscopic excision using prone positioning. Am J Orthop (Belle Mead NJ) 2010;39:E11-4. [Google Scholar | PubMed]
- 13.Pawar E, Modi N, Yadav AK, Mhatre J, Khemkar S, Mishra S. A solitary ventral scapular osteochondroma causing pseudo-winging of scapula: A case report. J Orthop Case Rep 2021;11:82-5. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor
July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor February 1, 2026 Symptomatic Ventromedial Scapular Osteochondroma Presenting with Restriction of Shoulder Movements: A Case Report
February 1, 2026 Symptomatic Ventromedial Scapular Osteochondroma Presenting with Restriction of Shoulder Movements: A Case Report December 1, 2025 A Heavy Burden on the Back: Surgical Excision of a Massive Scapular Osteochondroma – A Case Report
December 1, 2025 A Heavy Burden on the Back: Surgical Excision of a Massive Scapular Osteochondroma – A Case Report August 6, 2024 Dorsal Scapular Osteochondroma in a Young Male: A Case Report and Literature Review
August 6, 2024 Dorsal Scapular Osteochondroma in a Young Male: A Case Report and Literature Review