
Full resection of a tenosynovial giant cell tumor may lead to adequate bone remodeling of a bony erosion, caused by mechanical pressure, without need of further intervention.
Dr. Maria Tsatlidou, Department of Orthopaedic, St Luke’s Hospital, Panorama, Thessaloniki, Greece, Thessaloniki, Greece. E-mail: maria.tsatlidou@yahoo.com
Abstract
Introduction: The term tenosynovial giant cell tumor encompasses a group of rare soft-tissue tumors. A new classification divides the group in localized and diffuse type, depending on the involvement of the surrounding tissues. Due to the unclear origin and heterogeneity in extend of the diffuse-type giant cell tumors, there is only limited evidence on the tumor-specific treatment. Thus, every case report has an added value toward setting disease-specific guidelines.
Case Report: Presentation of a diffuse type tenosynovial giant cell tumor encircling the first metatarsal. The tumor had mechanically eroded the plantar aspect of the distal metaphysis, with no signs of tumor spread. After an open biopsy, resection of the mass was performed without debriding or resecting the first metatarsal. Repeat imaging postoperatively showed no recurrence at 4-year follow-up and a bony remodeling of the lesion.
Conclusion: Bone remodeling is possible after complete resection of diffuse tenosynovial giant cell tumor when the erosion is caused by mechanical pressure and no intraosseous expansion of the tumor is present.
Keywords: Diffuse-type tenosynovial giant cell tumor, first metatarsal, bony erosion, bone remodeling.
The term tenosynovial giant-cell tumor (TGCT) encompasses a group of soft-tissue tumors that can arise from the synovial lining of the joint, tendon, or bursa. According to the updated 2013 World Health Organization system for the classification of soft-tissue tumors, these can present as either localized-type or diffuse-type, depending on the extent of synovial involvement. Furthermore, both forms can arise intra-articularly or extra-articularly. In diffuse tumors however this origin may not always be clear [1,2]. The incidence of dtGST is 4–8.4 per million person-years. Despite their rarity, they represent the most common soft-tissue tumors of the foot and ankle [3,4]. Historically, a considerable heterogeneity of the relevant terminology has hampered the accumulation of large numbers of cases in patient cohorts and multicenter studies. As a result, in the literature, there is an abundance of case reports with few only large case series. Therefore, decision-making in individual cases follows general oncological principles rather than disease-specific guidelines based on strict recommendations. We present a case of a diffuse type giant cell tumor around the first metatarsal with a bone erosion at the level of the distal metaphysis. Following resection of the tumor without ray amputation, there was evidence of bony remodeling of the metatarsal.
A 44-year-old previously healthy female presented reporting a slowly growing mass at the dorsum of her right midfoot (Fig. 1).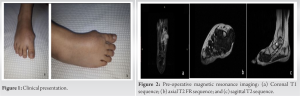 The patient was aware of the presence of the mass for many years; however, it became more symptomatic following a low energy sprain few months before consultation. Still, she was able to ambulate with no aids and wear normal shoes and had no need of analgesics. On clinical examination, the foot was neurovascularly intact with a normal range of motion and muscle power of all the regional joint and muscles, respectively. Skin color and temperature were normal. There was a semirigid palpable mass, relatively mobile over the dorsum of the first metatarsal, extending plantarly to the medial arch. Imaging studies on presentation included plain radiographs and an magnetic resonance imaging of the foot, which revealed a diffuse soft-tissue tumor encircling the first metatarsal and expanding beyond the borders of the regional foot compartments. The tumor had an intermediate to low irregular signal with no zones of necrosis or calcification (Fig. 2). The plantar distal metaphysis of the metatarsal showed an oval radiolucent zone with a concave configuration, whereas the cortex appeared intact (Fig. 3).
The patient was aware of the presence of the mass for many years; however, it became more symptomatic following a low energy sprain few months before consultation. Still, she was able to ambulate with no aids and wear normal shoes and had no need of analgesics. On clinical examination, the foot was neurovascularly intact with a normal range of motion and muscle power of all the regional joint and muscles, respectively. Skin color and temperature were normal. There was a semirigid palpable mass, relatively mobile over the dorsum of the first metatarsal, extending plantarly to the medial arch. Imaging studies on presentation included plain radiographs and an magnetic resonance imaging of the foot, which revealed a diffuse soft-tissue tumor encircling the first metatarsal and expanding beyond the borders of the regional foot compartments. The tumor had an intermediate to low irregular signal with no zones of necrosis or calcification (Fig. 2). The plantar distal metaphysis of the metatarsal showed an oval radiolucent zone with a concave configuration, whereas the cortex appeared intact (Fig. 3). 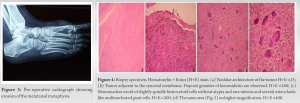 Additional tests and imaging were ordered, which included a full body Tc99 bone scan. This showed an increased uptake on the medial midfoot region with no signs from the rest of the skeleton. A multidisciplinary team including an oncologist, a musculoskeletal radiologist, and an orthopedic surgeon specializing in foot and ankle surgery convened to decide upon the treatment plan. An open biopsy was performed in the first instance. On pathology, the tumor had a multinodular architecture. It consisted of mononuclear ovoid or slightly spindle histiocytoid cells without atypia and rare mitosis, and several osteoclastic – like multinucleated giant cells. There were areas adjacent to the synovial membrane without penetrating it. Foci of deposit of hemosiderin granules and areas of fibrosis with hyalinization also observed (Fig. 4). The above findings established the diagnosis of a diffuse type tenosynovial giant cell tumor. The definitive management was an open excision of the tumor through a longitudinal dorsomedial approach. Intraoperatively, the tumor had a nodular appearance. It encircled the first metatarsal involving the extensor hallucis longus tendon which was resected. It spared the extensor hallucis brevis muscle belly and tendon. The medial-plantar distal metaphysis was pressured by the tumor creating a smooth and convex impression. The cortex was smooth and intact, without signs of a macroscopic erosion and tumor infiltration.
Additional tests and imaging were ordered, which included a full body Tc99 bone scan. This showed an increased uptake on the medial midfoot region with no signs from the rest of the skeleton. A multidisciplinary team including an oncologist, a musculoskeletal radiologist, and an orthopedic surgeon specializing in foot and ankle surgery convened to decide upon the treatment plan. An open biopsy was performed in the first instance. On pathology, the tumor had a multinodular architecture. It consisted of mononuclear ovoid or slightly spindle histiocytoid cells without atypia and rare mitosis, and several osteoclastic – like multinucleated giant cells. There were areas adjacent to the synovial membrane without penetrating it. Foci of deposit of hemosiderin granules and areas of fibrosis with hyalinization also observed (Fig. 4). The above findings established the diagnosis of a diffuse type tenosynovial giant cell tumor. The definitive management was an open excision of the tumor through a longitudinal dorsomedial approach. Intraoperatively, the tumor had a nodular appearance. It encircled the first metatarsal involving the extensor hallucis longus tendon which was resected. It spared the extensor hallucis brevis muscle belly and tendon. The medial-plantar distal metaphysis was pressured by the tumor creating a smooth and convex impression. The cortex was smooth and intact, without signs of a macroscopic erosion and tumor infiltration.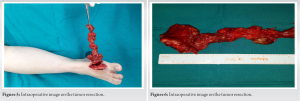 A decision was made not to amputate the first ray, but instead resect the tumor in wide margin regarding the surrounding soft tissues. The part of the tumor in contact with the bone was carefully resected with respect to the adjacent periosteal border of the metatarsal. The tumor was excised en bloc and sent for biopsy, which confirmed the primary diagnosis (Fig. 5 and 6). As there was no evidence of bone involvement other than the erosion that was caused by mechanical pressure, the metatarsal was left intact. The patient’s post-operative course was uneventful. She was allowed to fully weight bear after wound healing. She was reviewed clinically on an annual basis with X-rays of the affected foot.
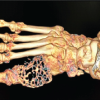
A decision was made not to amputate the first ray, but instead resect the tumor in wide margin regarding the surrounding soft tissues. The part of the tumor in contact with the bone was carefully resected with respect to the adjacent periosteal border of the metatarsal. The tumor was excised en bloc and sent for biopsy, which confirmed the primary diagnosis (Fig. 5 and 6). As there was no evidence of bone involvement other than the erosion that was caused by mechanical pressure, the metatarsal was left intact. The patient’s post-operative course was uneventful. She was allowed to fully weight bear after wound healing. She was reviewed clinically on an annual basis with X-rays of the affected foot. She resumed full activities and was able to actively dorsiflex the great toe with a power of 4/5 and walk with no aids. In repeat imaging 3 year post-operative, there were signs of remodeling of the distal metaphysis of the first metatarsal, as shown in comparative oblique views (Fig. 7). A foot computed tomography was ordered to confirm the finding (Fig. 8). Five years post-operative, the patient shows no signs of recurrence.
She resumed full activities and was able to actively dorsiflex the great toe with a power of 4/5 and walk with no aids. In repeat imaging 3 year post-operative, there were signs of remodeling of the distal metaphysis of the first metatarsal, as shown in comparative oblique views (Fig. 7). A foot computed tomography was ordered to confirm the finding (Fig. 8). Five years post-operative, the patient shows no signs of recurrence.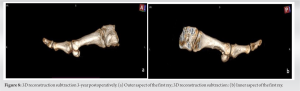
A bony GST affecting the first metatarsal is quite rare. In a series of 18 patients with GCT of the foot and ankle, the authors report no case of involvement of the first metatarsal [5]. In our case, a decision was made to spare the first metatarsal from resection, despite the bony erosion. The pre-operative imaging characteristics and intraoperative imaging findings suggested that the lesion was caused by chronic mechanical pressure from the tumor and not from infiltration by the tumor per se. Other space-occupying lesions, such as rheumatoid nodules and aortic aneurysms have also demonstrated such a behavior on adjacent bone [6]. In these cases, bony erosion seems to be the result of bone resorption from biomechanical pressure, rather than bone destruction [7]. An alternative to the interoperative management would have been to add a core biopsy of the first metatarsal. After oncologic consultation and in accordance to general oncological principles dictated by the current literature open biopsy is preferable for musculoskeletal tumors and is shown to be more accurate compared to ultrasound guided fine needle and core biopsy [8]. In addition to this, due to the encircling nature of the primary tumor, there were concerns that this could create an iatrogenic path for local spread. The remodeling of the first metatarsal and absence of findings suggestive of a local recurrence eventually justified the choice to preserve the first ray. In any case, a ray amputation remains an option in the event of late recurrence involving the metatarsal. The incidence of such ray amputations in bony GCT tumors of the foot and ankle is reported to be as low as 11% [5]. Following oncologic consultation and in line with current literature, adjuvant therapy was not implemented in this case. Lately, targeted immunological therapies have been added to several treatment protocols. This came as a result of the identification of a common chromosomal abnormality in some of the tumor cells which leads to an over expression of colony-stimulating factor 1. Other adjuncts to operative intervention include external beam radiation therapy [9] and isotopic synovectomy [10,11,12]. At present, such a combined treatment, regime is mainly implemented in short-term recurrent disease [12] and its efficacy is yet to be validated [2,12]. Recurrence rate of dt GCT remains considerably high. More than half of the recurrences occur in the first 2-year postoperatively, with an overall rate of 7% within the first 5 years [13]. In our case, the patient shows no signs of recurrence at the latest follow-up, 4 years postoperatively. She is scheduled for her final 5-year post-operative review in 2 months, after which time, she will be discharged.
The current case suggests that bone remodeling in the vicinity of diffuse type giant cell tumors is possible following a complete resection of the mass, provided that the erosion is caused by chronic mechanical pressure and there is no intraosseous expansion of the tumor.
The term diffuse type tenosynovial giant cell tumor indicate involvement of multiple tissues. The presence of bone lesions could raise concerns regarding the treatment options and the level of surgical intervention. If tumor spread in the adjacent bone is precluded, full resection of the tumor is shown to be adequate treatment, leading to bone remodeling in case of bony erosion caused by mechanical pressure.
References
- 1.Somerhausen NS, van den Rijn M. Tenosynovial giant cell tumor, diffuse type. In: Fletcher CD, Bridge JA, Hogendoorn PC, Mertens F, editors. World Health Organization Classification of Tumors. Pathology and Genetics of Tumors of Soft Tissue and Bone. 4th ed. Lyon: IARC Press; 2013. p. 102-3. [Google Scholar | PubMed]
- 2.Fraser EJ, Sullivan M, Maclean F, Nesbitt A. Tenosynovial giant-cell tumors of the foot and ankle: A critical analysis review. JBJS Rev 2017;5: 01874474-201701000-00001. [Google Scholar | PubMed]
- 3.Chou LB, Ho YY, Malawer MM. Tumors of the foot and ankle: Experience with 153 cases. Foot Ankle Int 2009;30:836-41. [Google Scholar | PubMed]
- 4.Toepfer A, Harrasser N, Recker M, Lenze U, Pohlig F, Gerdesmeyer L, et al. Distribution patterns of foot and ankle tumors: A university tumor institute experience. BMC Cancer 2018;18:735. [Google Scholar | PubMed]
- 5.Rajani R, Schaefer L, Scarborough MT, Gibbs CP. Giant cell tumors of the foot and ankle bones: High recurrence rates after surgical treatment. J Foot Ankle Surg 2015;54:1141-5. [Google Scholar | PubMed]
- 6.Aydogan M, Karatoprak O, Mirzanli C, Ozturk C, Tezer M, Hamzaoglu A. Severe erosion of lumbar vertebral body because of a chronic ruptured abdominal aortic aneurysm. Spine J 2008;8:394-6. [Google Scholar | PubMed]
- 7.Monsees B, Murphy WA. Pressure erosions: A pattern of bone resorption in rheumatoid arthritis. Arthritis Rheum 1985;28:820-4. [Google Scholar | PubMed]
- 8.Traina F, Errani C, Toscano A, Pungetti C, Fabbri D, Mazzotti A, et al. Current concepts in the biopsy of musculoskeletal tumors: AAOS exhibit selection. J Bone Joint Surg Am 2015;97:e7. [Google Scholar | PubMed]
- 9.Lee M, Mahroof S, Pringle J, Short SC, Briggs TW, Cannon SR. Diffuse pigmented villonodular synovitis of the foot and ankle treated with surgery and radiotherapy. Int Orthop 2005;29:403-5. [Google Scholar | PubMed]
- 10.Bickels J, Isaakov J, Kollender Y, Meller I. Unacceptable complications following intra-articular injection of yttrium 90 in the ankle joint for diffuse pigmented villonodular synovitis. J Bone Joint Surg Am 2008;90:326-8. [Google Scholar | PubMed]
- 11.Shabat S, Kollender Y, Merimsky O, Isakov J, Flusser G, Nyska M, et al. The use of surgery and yttrium 90 in the management of extensive and diffuse pigmented villonodular synovitis of large joints. Rheumatology (Oxford) 2002;41:1113-8. [Google Scholar | PubMed]
- 12.Mastboom MJ, Palmerini E, Verspoor FG, Rueten-Budde AJ, Stacchiotti S, Staals EL, et al. Surgical outcomes of patients with diffuse-type tenosynovial giant-cell tumours: An international, retrospective, cohort study. Lancet Oncol 2019;20:877-6. [Google Scholar | PubMed]
- 13.Siegel M, Bode L, Südkamp N, Kühle J, Zwingmann J, Schmal H, et al. Treatment, recurrence rates and follow-up of tenosynovial giant cell tumor (TGCT) of the foot and ankle-a systematic review and meta-analysis. PLoS One 2021;16:e0260795. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 A Rare Case of Giant Cell Tumor of the First Metatarsal: En Bloc Resection and Fibular Autograft Reconstruction
June 1, 2026 A Rare Case of Giant Cell Tumor of the First Metatarsal: En Bloc Resection and Fibular Autograft Reconstruction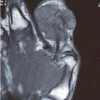 January 1, 2026 Tenosynovial Giant Cell Tumor of the Thumb with Bony Erosion – A Case Report on Surgical Excision with Adjuvant Chemical Cauterization
January 1, 2026 Tenosynovial Giant Cell Tumor of the Thumb with Bony Erosion – A Case Report on Surgical Excision with Adjuvant Chemical Cauterization September 1, 2024 Giant Cell Tumor of First Metatarsal: A Rare Case Report with Literature Review
September 1, 2024 Giant Cell Tumor of First Metatarsal: A Rare Case Report with Literature Review February 10, 2023 First Metatarsal Bilateral Stress Fracture: A Case Report
February 10, 2023 First Metatarsal Bilateral Stress Fracture: A Case Report