
Use of real-time navigation for en-bloc excision of subaxial cervical osteochondroma is being reported for the first time through this case report.
Dr. Nishad V Situt, Department of Spine Surgery, Sancheti Institute for Orthopaedics and Rehabilitation, Pune, Maharashtra, India. E-mail: situt.nishad@gmail.com
Abstract
Introduction: Vertebral osteochondroma is a rare entity. It presents with varied complaints ranging from palpable mass to myeloradiculopathy. En bloc excision is the gold standard treatment option for symptomatic patients. Real-time intraoperative navigation has increased the accuracy and safety of tumor excision. We report a case of cervical subaxial osteochondroma with myelo-radiculopathy, treated with excision, and monosegmental fusion under O-arm-based real-time navigation.
Case Report: A 32-year-old male presented with complaints of axial neck pain with the right upper limb radiculopathy for 18 months. On examination, signs of myelopathy were identified without sensory-motor deficit. Magnetic resonance imaging and computed tomography scans were suggestive of solitary C6 osteochondroma compressing spinalcord. O-arm navigated en-bloc tumor excision with C5 hemilaminectomy and monosegmental fusion was done.
Conclusion: The use of O-arm navigation aids in accurate intraoperative en bloc excision without any residual tumor and with better safety.
Keywords: Spinal tumors, O-arm navigation, vertebral osteochondroma, bone tumor
Solitary vertebral osteochondromas are a rare entity with a prevalence of only 1.3–4.1% [1]. Cervical spine and upper dorsal spine are common sites for development of vertebral osteochondroma. It presents with varied complaints, ranging from axial neck pain with palpable mass to myelopathy depending on the level of vertebra involved and amount of cord compression [2]. In literature, multiple treatment options have been discussed from watchful neglect to en bloc excision [3]. Usually, surgical excision is considered the gold standard treatment for the symptomatic ones. O-arm navigation is increasingly being used in the surgical management of such benign tumors in the spine as it assures safety and complete excision of these lesions [4]. We hereby report a first ever documented case of a subaxial solitary cervical osteochondroma managed surgically with O-arm-based real-time navigation-guided excision and monosegmental fixation.
A 32-year-old male presented with complaints of neck pain with the right upper limb radiation visual analog scale (VAS) 9/10 and numbness for 18 months. On examination, the right inverted radial reflex and long tract signs in both lower limbs were positive without sensory motor deficit. Orthogonal radiographs of the cervical spine showed mild-to-moderate disc degenerative changes at multiple levels with maintained cervical lordosis (Fig. 1a and b). 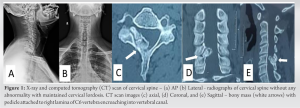 Magnetic resonance imaging cervical spine revealed T1 hypointense and T2 isointense outgrowth arising from C6 right lamina protruding in spinal canal compressing right hemi cord and C6 right nerve root (Fig. 2a, b, c, d).
Magnetic resonance imaging cervical spine revealed T1 hypointense and T2 isointense outgrowth arising from C6 right lamina protruding in spinal canal compressing right hemi cord and C6 right nerve root (Fig. 2a, b, c, d). 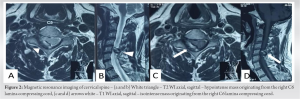 Computed tomography (CT) scan showed a pedunculated bony outgrowth arising from the right C6 lamina extending superiorly within the vertebral canal (Fig. 1c, d, e). Due to worsening myelo-radiculopathy symptoms, the patient underwent posterior cervical C5 and C6 laminectomy with tumor excision and lateral mass stabilization. Surgery was performed in a prone position under neuromonitoring guidance and O-arm navigation assistance (Medtronic, Inc, Minneapolis, Minnesota, U.S.). The posterior cervical approach was used to expose C4 to C6 lamina. The Minimally Invasive Reference Array was then attached to the C4 spinous process, and first O-arm spin was taken. The images were transferred to the stealth station for navigation. Lateral mass screw entry and track was made with navigated probe and tapping instruments. Screw holes were blocked with bone wax; no screws were inserted before tumor excision to prevent disturbance of the screw heads during laminectomy. Site of osteochondroma was located with navigated pedicle sound, which was found to be attached to C6 lamina. (Fig. 3a) Right C5 and C6 lamina was thinned out using a high speed navigated Burr (Medtronic, Inc, Minneapolis, Minnesota, U.S.). After burring the peduncle, the tumor was found to be non-adherent to surrounding neural and bony structures and was excised en bloc.
Computed tomography (CT) scan showed a pedunculated bony outgrowth arising from the right C6 lamina extending superiorly within the vertebral canal (Fig. 1c, d, e). Due to worsening myelo-radiculopathy symptoms, the patient underwent posterior cervical C5 and C6 laminectomy with tumor excision and lateral mass stabilization. Surgery was performed in a prone position under neuromonitoring guidance and O-arm navigation assistance (Medtronic, Inc, Minneapolis, Minnesota, U.S.). The posterior cervical approach was used to expose C4 to C6 lamina. The Minimally Invasive Reference Array was then attached to the C4 spinous process, and first O-arm spin was taken. The images were transferred to the stealth station for navigation. Lateral mass screw entry and track was made with navigated probe and tapping instruments. Screw holes were blocked with bone wax; no screws were inserted before tumor excision to prevent disturbance of the screw heads during laminectomy. Site of osteochondroma was located with navigated pedicle sound, which was found to be attached to C6 lamina. (Fig. 3a) Right C5 and C6 lamina was thinned out using a high speed navigated Burr (Medtronic, Inc, Minneapolis, Minnesota, U.S.). After burring the peduncle, the tumor was found to be non-adherent to surrounding neural and bony structures and was excised en bloc.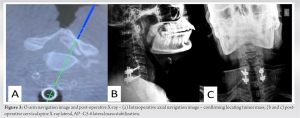 The excised tumor had smooth surface, hard consistency, and dimensions of 2 × 1.6 × 0.8 cm (Fig. 4a).
The excised tumor had smooth surface, hard consistency, and dimensions of 2 × 1.6 × 0.8 cm (Fig. 4a).  The lateral mass screws were then inserted at C5, C6 levels bilaterally without any interference of neuromonitoring signals. The post excision O-arm CT scan revealed gross complete excision of the tumor mass with satisfactory positioning of lateral mass screws (Fig. 5a, b, c).
The lateral mass screws were then inserted at C5, C6 levels bilaterally without any interference of neuromonitoring signals. The post excision O-arm CT scan revealed gross complete excision of the tumor mass with satisfactory positioning of lateral mass screws (Fig. 5a, b, c). 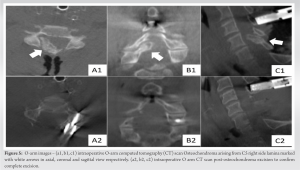 The patient was extubated successfully without any residual neurological compromise. Post-operative radiograph showed C5-6 lateral mass fixation with acceptable implant position. (Fig. 3b and c) Histopathology examination showed mature trabecular bone mixed with fragments of mature cartilage, with chondrocytes in lacunae confirming the diagnosis of osteochondroma. (Fig. 4a and c) Post-operative course was uneventful and symptoms improved (VAS 2/10) without any neurological deficit. On 2-year follow-up, the patient was asymptomatic with orthogonal radiographs showing satisfactory position of lateral mass and without any local recurrence.
The patient was extubated successfully without any residual neurological compromise. Post-operative radiograph showed C5-6 lateral mass fixation with acceptable implant position. (Fig. 3b and c) Histopathology examination showed mature trabecular bone mixed with fragments of mature cartilage, with chondrocytes in lacunae confirming the diagnosis of osteochondroma. (Fig. 4a and c) Post-operative course was uneventful and symptoms improved (VAS 2/10) without any neurological deficit. On 2-year follow-up, the patient was asymptomatic with orthogonal radiographs showing satisfactory position of lateral mass and without any local recurrence.
Vertebral osteochondromas are rare, that is, only 1.3–4.1% of solitary osteochondromas arise in the spine, where they constitute up to 0.4% of intraspinal tumors [1]. Yakkanti et al. did a review of case reports of cervical osteochondroma published from 2003 to 2018 and observed that cervical spine was the most common site of vertebral osteochondroma; with lamina (19.4%) being the most common site of origin followed by pedicle (8.3%) [2]. Similar findings were also reported by Lotfinia et al. with axial spine being the most common site followed by subaxial spine in vertebral osteochondroma. The cervical spine gets typically more affected due to its greater mobility, microfracture and displacement of portions of epiphyseal growth plate [5]. Sciubba et al. published the largest series of vertebral osteochondroma with 27 cases and observed that most of the vertebral osteochondromas were originating from the mobile spine as compared to sacrum. They reported thoracic spine to be the most commonly involved region [6]. Cervical osteochondroma growing within the vertebral canal is a rare occurrence. Most of the vertebral osteochondromas are asymptomatic as it grows outside the vertebral canal. Sciubba et al. observed that 74% of their patients had complaints of axial pain and 15% had myelopathy signs and symptoms [6]. Patients may present with oncological pain due to pressure on the adjoining structures if growth is outside the vertebral canal [3]. However, this was in contrast to our case where the osteochondroma was arising from C6 right side lamina, which was encroaching the vertebral canal and compressing the spinal cord, which is a rare site for this tumor. The most common site is from the posterior element, growing outside the canal, and hence less frequently causing myelopathic symptoms [7]. As most tumors are asymptomatic and are diagnosed accidentally, they are followed up closely with watchful neglect [8]. For the symptomatic tumors with myelopathy and/or radiculopathy, surgical excision is usually indicated. Osteochondromas originating in the posterior element are excised (intralesional/en bloc) with laminectomy with or without fusion using the posterior approach [3]. Complete excision of intralesional tumors has low rate of local recurrences. However, recurrences after en bloc resection also have been reported [6]. O-arm guided navigation is increasingly being utilized in benign spinal tumors for ensuring gross complete excision of these tumors and accurate screw placement [4]. Two cases of O-arm navigation guided excision, that is, one in C2 vertebrae and one in thoracic spine report the following advantages: (1) Accurate localization of the lesions, (2) ensuring gross complete excision intraoperatively, and lastly (3) accurate implant placement whenever stabilization is warranted [9,10]. We report the first case of a subaxial cervical vertebral osteochondroma treated with O-arm navigation-guided en bloc excision with excellent outcome and no recurrence in 2-year follow-up.
Solitary cervical osteochondroma although rare can present as cervical myeloradiculopathy. The use of O-arm navigation aids in accurate intraoperative en bloc excision without any residual tumor and better safety.
Vertebral osteochondroma is a very rare type of tumor with lesion growing within vertebral canal causing myelopathy is even a rarer presentation. The use of an O-arm with real-time navigation for excision of a subaxial cervical spine osteochondroma is being reported for the first time through this case report.
References
- 1.Sekharappa V, Amritanand R, Krishnan V, David KS. Symptomatic solitary osteochondroma of the subaxial cervical spine in a 52-year-old patient. Asian Spine J 2014;8:84-8. [Google Scholar | PubMed]
- 2.Yakkanti R, Onyekwelu I, Carreon LY, Dimar JR 2nd. Solitary osteochondroma of the spine-A case series: Review of solitary osteochondroma with myelopathic symptoms. Glob Spine J 2018;8:323-39. [Google Scholar | PubMed]
- 3.Fowler J, Takayanagi A, Siddiqi I, Ghanchi H, Siddiqi J, Veeravagu A, et al. Cervical osteochondroma: Surgical planning. Spinal Cord Ser Cases 2020;6:44. [Google Scholar | PubMed]
- 4.Nasser R, Drazin D, Nakhla J, Al-Khouja L, Brien E, Baron EM, et al. Resection of spinal column tumors utilizing image-guided navigation: A multicenter analysis. Neurosurg Focus 2016;41:E15. [Google Scholar | PubMed]
- 5.Lotfinia I, Vahedi A, Aeinfar K, Tubbs RS, Vahedi P. Cervical osteochondroma with neurological symptoms: Literature review and a case report. Spinal Cord Ser Cases 2017;3:16038. [Google Scholar | PubMed]
- 6.Sciubba DM, Macki M, Bydon M, Germscheid NM, Wolinsky JP, Boriani S, et al. Long-term outcomes in primary spinal osteochondroma: A multicenter study of 27 patients. J Neurosurg Spine 2015;22:582-8. [Google Scholar | PubMed]
- 7.Chang DG, Park JB. Osteochondroma arising from the transverse process of the lower cervical spine in an elderly patient. World Neurosurg 2019;130:450-3. [Google Scholar | PubMed]
- 8.Veeravagu A, Li A, Shuer LM, Desai AM. Cervical osteochondroma causing myelopathy in adults: Management considerations and literature review. World Neurosurg 2017;97:752.e5-752.e13. [Google Scholar | PubMed]
- 9.Hagiwara K, Wada K, Tamaki R, Inoue T, Okazaki K. Osteochondroma of the C2 vertebral body totally resected using an intraoperative O-arm navigation system: A case report. Spine Surg Relat Res 2020;4:380-3. [Google Scholar | PubMed]
- 10.Pham MH, Cohen J, Tuchman A, Commins D, Acosta FL. Large solitary osteochondroma of the thoracic spine: Case report and review of the literature. Surg Neurol Int 2016;7 Suppl 13:S323-7. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Acute Cauda Equina Syndrome Following Transpedicular Biopsy of a Lumbar Vertebral Lesion: A Case Report of Spinal Non-Hodgkin’s Lymphoma
July 1, 2026 Acute Cauda Equina Syndrome Following Transpedicular Biopsy of a Lumbar Vertebral Lesion: A Case Report of Spinal Non-Hodgkin’s Lymphoma May 1, 2026 Removal of Hartshill Rectangle and Wires with Revision Pedicle Screw Fixation: Technical Challenges, Safety Considerations, and Clinical Outcomes in Complex Spinal Reconstruction – A Case Report
May 1, 2026 Removal of Hartshill Rectangle and Wires with Revision Pedicle Screw Fixation: Technical Challenges, Safety Considerations, and Clinical Outcomes in Complex Spinal Reconstruction – A Case Report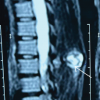 April 1, 2026 Osteochondroma of Dorsal Spine: A Rare Clinical Entity
April 1, 2026 Osteochondroma of Dorsal Spine: A Rare Clinical Entity February 1, 2026 Isolated Osteochondromas of the Inner and Outer Tables of the Ilium: A Report of two Rare Cases
February 1, 2026 Isolated Osteochondromas of the Inner and Outer Tables of the Ilium: A Report of two Rare Cases