
Acute neurological deterioration may rarely occur after biopsy of pathological vertebral lesions, and close post-procedural neurological monitoring with urgent repeat imaging and timely decompression when indicated are essential to prevent irreversible neurological deficits.
Dr Jyotishman Barman, Department of Orthopaedics, Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra, India. E-mail: jyotishman.barman0@gmail.com
Abstract
Introduction: Spinal involvement in non-Hodgkin’s lymphoma (NHL) is uncommon and often presents with non-specific clinical and radiological features, frequently mimicking infective or degenerative spinal pathology. Tissue diagnosis using transpedicular biopsy is commonly performed in such cases. However, acute neurological deterioration occurring after biopsy in a pathological vertebra is rare. We report a unique case of acute cauda equina syndrome (CES) developing in close temporal association with transpedicular biopsy of a lumbar vertebral lesion, later diagnosed as NHL.
Case Report: A 60-year-old male presented with low back pain and left-predominant lower limb radiculopathy of 4 weeks’ duration, without any bowel or bladder involvement or neurological deficit. Magnetic resonance imaging (MRI) revealed a pathological lesion involving the L4 vertebra, with differential diagnoses including infection and malignancy. A left-sided L4 transpedicular biopsy was performed under local anaesthesia, following which the patient remained neurologically intact. On the 4th post-biopsy day, the patient developed acute CES characterised by bilateral lower limb weakness, bilateral flail foot, perianal sensory loss, urinary retention, and constipation. Repeat MRI demonstrated significant cauda equina compression. Histopathological examination confirmed NHL. The patient underwent urgent L4–L5 decompression and stabilisation, followed by systemic chemotherapy.
Conclusion: Although transpedicular biopsy is considered a safe diagnostic procedure, acute neurological deterioration may rarely occur in patients with pathological vertebral lesions. A definitive causal relationship between biopsy and neurological deterioration cannot be established from a single case; however, this case highlights the importance of close post-procedural neurological monitoring. Early recognition of CES, urgent repeat imaging, and timely decompression, when indicated, are essential to reduce the risk of irreversible neurological deficits.
Keywords: Cauda equina syndrome, non-Hodgkin’s lymphoma, transpedicular biopsy, lumbar spine, spinal tumors.
Spinal involvement in non-Hodgkin’s lymphoma (NHL) is rare and accounts for a small proportion of extranodal lymphomas, with primary spinal lymphoma being particularly uncommon [1]. Vertebral involvement may occur with or without epidural extension and most frequently affects the thoracic spine, followed by the lumbar region [2]. The clinical presentation is often nonspecific, commonly manifesting as localised back pain or radiculopathy, and may closely mimic infective or degenerative spinal pathology, leading to diagnostic delays [3]. Magnetic resonance imaging (MRI) is the modality of choice for evaluating spinal lesions; however, imaging characteristics of spinal lymphoma are frequently non-specific and may overlap with those of spinal tuberculosis, metastatic disease, or pyogenic spondylodiscitis [4,5]. Several authors have emphasised that MRI alone is often insufficient to establish a definitive diagnosis in spinal lymphoma, particularly in tuberculosis-endemic regions or in patients with a prior history of tuberculosis [6,7]. Consequently, histopathological confirmation remains essential for accurate diagnosis and appropriate treatment planning. Transpedicular biopsy is a widely accepted, minimally invasive technique for obtaining tissue diagnosis in vertebral lesions and is generally considered safe, with a low reported complication rate [8]. Reported complications include bleeding, infection, and rarely neurological injury [9]. Neurological deterioration following transpedicular biopsy is uncommon, and the development of acute cauda equina syndrome (CES) after such a diagnostic procedure is exceptionally rare. CES represents a spinal emergency and requires urgent recognition and intervention to prevent irreversible neurological deficits [10]. Although uncommon, CES has been reported as a presenting or impending manifestation of primary spinal NHL [11]. However, the occurrence of acute CES following a diagnostic spinal biopsy has been scarcely reported in the literature and presents a unique therapeutic dilemma regarding the timing of surgical decompression versus initiation of chemotherapy. While NHL is generally considered a chemosensitive and radiosensitive malignancy, the role of surgical decompression in patients with acute or rapidly progressive neurological deficits remains debated. Several studies have suggested that combined surgical decompression and adjuvant therapy may offer superior neurological recovery in selected patients compared to non-surgical treatment alone [12,13]. We report a rare case of acute CES developing in close temporal association with transpedicular biopsy of an L4 vertebral lesion, subsequently diagnosed as NHL, highlighting the diagnostic challenges, procedural risks, and management considerations associated with this unusual presentation.
A 60-year-old male presented to the outpatient department with complaints of low back pain and left-predominant lower limb radicular pain of 4 weeks’ duration. The pain was insidious in onset, gradually progressive, and severe enough to restrict mobility, rendering the patient largely bedridden. There was no history of trauma to the spine or lower limbs. At presentation, the patient denied bowel or bladder dysfunction, sensory disturbances, or constitutional symptoms. He had a past history of pulmonary tuberculosis treated 18 years earlier with the completion of anti-tubercular therapy, with residual unilateral lung collapse as a sequela. There was no history of diabetes mellitus or other significant comorbid illness (Fig. 1).
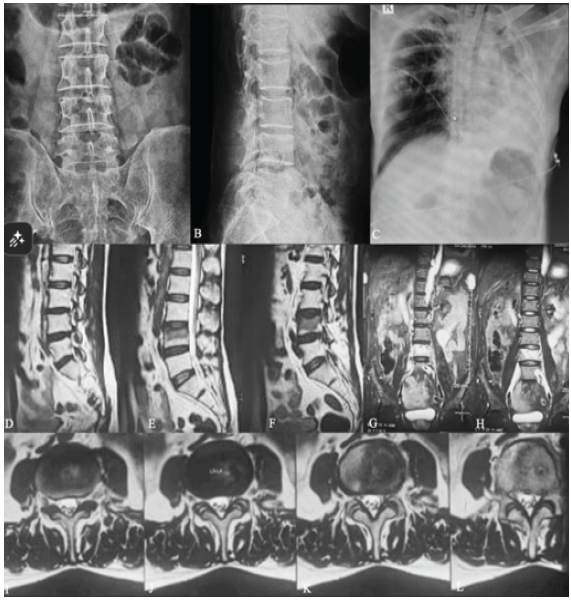
Figure 1: (a) Anteroposterior radiograph of the lumbar spine at presentation showing degenerative changes without obvious gross instability. (b) Lateral radiograph of the lumbar spine demonstrating a partial compression fracture of the L4 vertebral body. (c) Chest radiograph showing left lung collapse, consistent with sequelae of prior pulmonary tuberculosis. (d, e, f) T2-weighted sagittal magnetic resonance imaging (MRI) of the lumbar spine demonstrating partial compression fracture of the L4 vertebral body with associated marrow edema, along with diffuse posterior disc protrusion at the L4–L5 level causing compression of the thecal sac and encroachment of the bilateral neural foramina. A posterior disc bulge at the L3–L4 level causing indentation of the thecal sac is also noted. (g and h) Coronal MRI images showing involvement of the L4 vertebral body with altered marrow signal intensity. (i, j, k, l) Axial MRI sections demonstrating compression of the thecal sac at the L4–L5 level with bilateral neural foraminal narrowing and abutment of the exiting nerve roots, corresponding to the sagittal and coronal findings.
On examination, lumbar spine movements were restricted and painful. The straight leg-raising test was positive at 60° on the right side and 40° on the left side. Neurological examination of both lower limbs revealed no gross motor deficit, normal sensory examination across all dermatomes, and intact deep tendon reflexes. Plantar responses were flexor bilaterally. Bowel and bladder functions were intact, and there were no clinical features suggestive of CES at baseline. An MRI of the lumbar spine demonstrated a pathological lesion involving the L4 vertebral body (Fig. 1), raising suspicion for an infective or neoplastic aetiology. Pre-biopsy assessment was based on clinical examination and MRI findings. Quantitative assessment of dynamic spinal instability using flexion-extension radiographs or a validated spinal instability scoring system was not performed. In view of the patient’s previous history of pulmonary tuberculosis and the overlapping radiological features of infective and neoplastic spinal pathology, tissue diagnosis was considered necessary before definitive treatment planning. A left-sided L4 transpedicular biopsy was performed under local anaesthesia using an 11-gauge Jamshidi needle. Four biopsy cores were obtained; the initial two cores yielded no diagnostic material, while the subsequent two cores yielded soft, friable tissue. Samples were sent for GeneXpert testing, acid–fast bacilli smear, bacterial culture and sensitivity, and histopathological examination. Immediate post-procedure radiographs were satisfactory, and the patient remained neurologically intact following the biopsy (Fig. 2).

Figure 2: (a) Intraoperative C-arm anteroposterior fluoroscopic image demonstrating the transpedicular approach through the left L4 pedicle for biopsy. (b) Lateral fluoroscopic image confirming appropriate trajectory and depth of the transpedicular biopsy tract within the L4 vertebral body. (c) Intraoperative photograph showing the biopsy specimen obtained, appearing as soft, friable tissue. (d and e) Immediate post-biopsy anteroposterior and lateral radiographs of the lumbar spine demonstrating maintained vertebral alignment with no evidence of acute instability. (f) Histopathological and immunohistochemical findings from transpedicular biopsy of the L4 vertebral body. Tumor cells show diffuse positivity for CD20, BCL6, MUM1, and BCL2, and are immunonegative for CD10, c-MYC, Cyclin D1, CD138, CD5, and TdT. The MIB-1 (Ki-67) labeling index is approximately 45%. These findings are consistent with diffuse large B-cell lymphoma, non-germinal center subtype, as classified by the Hans algorithm. (g) Low-power photomicrograph showing multiple fragmented tissue bits with areas of hemorrhage and crushing artifact. Sheets of histiocytes admixed with lymphoid cells are noted, along with occasional capillaries and a bony fragment showing marrow elements with trilineage hematopoiesis. (h) High-power photomicrograph showing occasional atypical cells with large vesicular nuclei and eosinophilic cytoplasm with areas of karyorrhexis.
Immediate post-biopsy MRI was not performed because the patient had no neurological deterioration immediately after the procedure. Therefore, early post-procedural changes such as epidural haematoma, oedema, subtle progression of epidural disease, or early vertebral collapse could not be assessed at that stage. Advanced vascular imaging or angiographic evaluation was also not performed, as there was no immediate clinical suspicion of vascular injury or active bleeding. On the fourth post-biopsy day, the patient developed acute neurological deterioration, presenting with abdominal distension, urinary retention, constipation, and sudden-onset weakness of both lower limbs. Neurological examination revealed bilateral hip and knee power of grade 3 (Medical Research Council grading) and complete loss of ankle dorsiflexion and plantarflexion bilaterally, consistent with bilateral flail foot. Sensory examination revealed perianal sensory loss, with absent bulbocavernosus reflex and voluntary anal contraction. These findings were consistent with acute CES. An urgent MRI scan demonstrated further collapse of the L4 vertebral body with an associated epidural soft-tissue component causing significant compression of the cauda equina at the L4 level, corresponding clinically with the patient’s rapid neurological decline (Fig. 3).
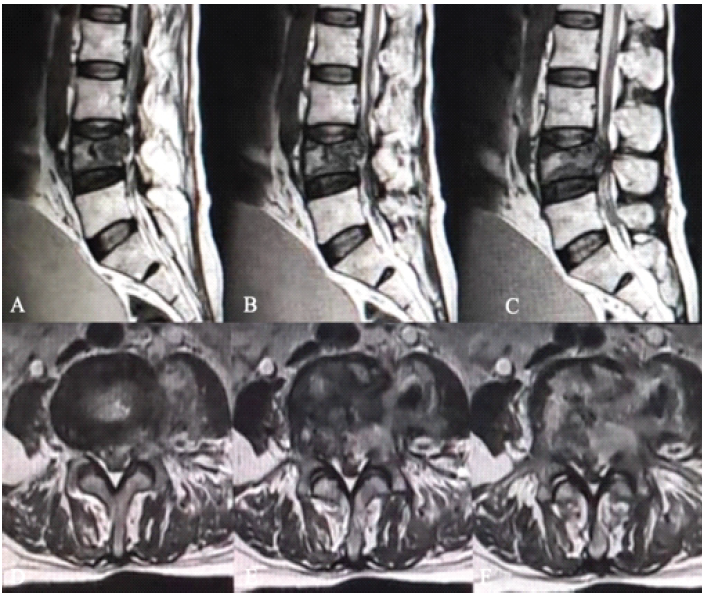
Figure 3: (a, b, c) T2-weighted sagittal magnetic resonance imaging of the lumbar spine obtained after acute neurological deterioration, demonstrating further collapse of the L4 vertebral body with an associated posterior epidural soft-tissue component causing marked indentation of the thecal sac and compression of the cauda equina. (d, e, f) Corresponding axial T2-weighted images at the L4 level showing severe central canal compromise with crowding and compression of the cauda equina nerve roots and near-complete effacement of the surrounding cerebrospinal fluid, correlating with the clinical features of acute cauda equina syndrome.
Microbiological investigations, including GeneXpert, acid–fast bacilli smear, and bacterial cultures, were negative. Histopathological examination of the biopsy specimen revealed a round blue cell tumour. On immunohistochemical analysis, the tumour cells showed diffuse positivity for CD20, BCL6, MUM1, and BCL2 and were immunonegative for CD10, c-MYC, Cyclin D1, CD138, CD5, and TdT. The MIB-1 (Ki-67) labelling index was approximately 45%. These findings were diagnostic of diffuse large B-cell lymphoma, non-germinal centre subtype, as classified by the Hans algorithm (Fig. 2). In view of the rapidly progressive neurological deficits and established CES, the patient underwent urgent L4–L5 decompression and stabilisation (Fig. 4).
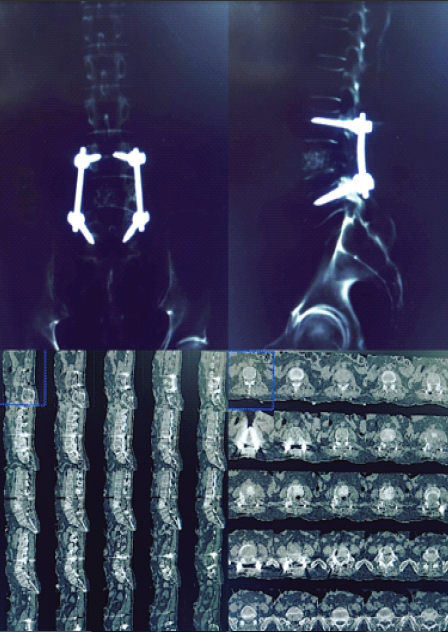
Figure 4: Postoperative computed tomography (CT) scan of the lumbosacral spine following posterior decompression and instrumented stabilization. (a) Coronal CT image demonstrating posterior pedicle screw–rod construct spanning L3 to L5. (b) Lateral CT reconstruction showing appropriate alignment of the instrumentation with restoration of spinal stability. (c) Sagittal CT reconstructions confirming satisfactory pedicle screw trajectory and rod placement across the L3–L5 levels. (d) Axial CT sections demonstrating appropriate pedicle screw positioning within the vertebral pedicles without evidence of cortical breach or implant malposition.
Following surgical recovery, the patient was started on systemic chemotherapy with a rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisolone-based regimen under the care of the oncology team. Postoperatively, the patient was managed with neurological monitoring, bladder care, limb physiotherapy, assisted mobilisation as tolerated, and supportive rehabilitation. Serial clinical neurological examinations were performed during follow-up; however, neurological recovery was not quantified using standardised neurological or disability scoring systems such as the ASIA impairment scale, Oswestry Disability Index, or Japanese Orthopaedic Association score. Formal quality-of-life assessment was also not performed. The patient completed chemotherapy and was kept on regular oncological follow-up. Despite treatment, the disease progressed, and the patient expired in January 2026, approximately 1 year after initiation of chemotherapy.
Spinal involvement in NHL is uncommon and often presents a diagnostic challenge due to its nonspecific clinical and radiological features. Vertebral lymphoma may closely mimic spinal infections, particularly tuberculosis, or degenerative spinal pathology, especially in patients with a prior history of pulmonary tuberculosis [2,3,6]. As seen in the present case, back pain with radiculopathy in the absence of neurological deficit can delay suspicion of an underlying malignant process, making histopathological confirmation essential for definitive diagnosis. MRI is the investigation of choice for evaluating spinal lesions; however, imaging findings in spinal lymphoma are frequently non-specific and may overlap with those of spinal tuberculosis, metastatic disease, or pyogenic spondylodiscitis [4,5]. Several authors have emphasised that MRI alone is often insufficient to establish a definitive diagnosis of spinal lymphoma, particularly in tuberculosis-endemic regions, necessitating tissue diagnosis [6,7]. Consequently, transpedicular biopsy is widely employed as a minimally invasive and generally safe diagnostic procedure for vertebral lesions, with a low reported complication rate [8,9]. Neurological deterioration following transpedicular biopsy is rare, and the development of acute CES after such a procedure is exceptionally uncommon. In the present case, the patient remained neurologically intact immediately following biopsy and developed acute CES on the 4th post-procedure day. Although a direct causal relationship cannot be definitively established, possible mechanisms include post-biopsy haemorrhage, tumour oedema, pathological vertebral collapse, or progression of epidural disease leading to acute neural compression. This temporal association highlights the importance of close neurological monitoring following spinal biopsy, particularly in pathological vertebrae [8,9]. Several limitations of the present case must be acknowledged. First, this report represents a single-patient observation and therefore cannot be generalised to all patients with spinal NHL or pathological vertebral lesions undergoing biopsy. Second, although acute CES developed in close temporal association with transpedicular biopsy, a definitive causal relationship between the biopsy procedure and neurological deterioration cannot be established. The exact mechanism remains speculative, as histological confirmation of post-biopsy haemorrhage, oedema, vascular injury, or acute tumour progression at the compressive site was not available. Pre-biopsy dynamic spinal instability was not quantitatively assessed using flexion-extension radiographs or a validated spinal instability scoring system. Occult mechanical instability in the pathological L4 vertebra may have contributed to subsequent vertebral collapse and neurological compromise. Immediate post-biopsy MRI was also not performed, limiting the ability to identify early epidural haematoma, oedema, subtle tumour progression, or early vertebral collapse. In addition, advanced vascular imaging or angiographic studies were not conducted; therefore, occult vascular injury or bleeding could not be conclusively excluded. The present report also does not allow comparison between transpedicular biopsy and alternative diagnostic techniques such as computed tomography-guided percutaneous biopsy or open biopsy. The diagnostic approach and management decisions reflect a single-centre experience and may not be universally reproducible. Functional neurological recovery after decompression was assessed clinically but was not quantified using standardised neurological or disability scoring systems. Similarly, post-operative rehabilitation outcomes, long-term oncological response, and quality-of-life measures were not comprehensively analysed. Since the patient expired approximately 1 year after initiation of chemotherapy, the long-term effectiveness of combined surgical and oncological management could not be adequately evaluated. The patient’s prior history of pulmonary tuberculosis may also have influenced the initial diagnostic pathway and introduced a potential diagnostic bias toward infective pathology. Nevertheless, negative microbiological investigations and subsequent histopathological and immunohistochemical confirmation established the final diagnosis of diffuse large B-cell lymphoma. Whether earlier decompression before the development of complete CES could have altered neurological or survival outcomes remains uncertain and cannot be concluded from this single case. Larger studies or additional comparable reports are required before evidence-based recommendations regarding monitoring protocols after biopsy of pathological vertebral lesions can be made. CES itself represents a neurosurgical emergency requiring urgent recognition and intervention to prevent irreversible neurological deficits [10]. While CES has been described as a presenting or impending feature of primary spinal lymphoma, as reported by Adhikari et al. [11], the occurrence of acute CES following a diagnostic transpedicular biopsy has been scarcely documented. This distinction is clinically important, as it underscores the rarity and novelty of the present case. The optimal management of spinal NHL with acute neurological compromise remains debated. Although lymphoma is generally chemosensitive and radiosensitive, several studies have demonstrated improved neurological outcomes with surgical decompression in patients presenting with severe or rapidly progressive neurological deficits [12,13]. Peng et al. reported better neurological recovery in selected patients treated with combined surgical decompression and adjuvant therapy compared to non-surgical treatment alone [12]. In the present case, the rapid progression to complete CES necessitated urgent decompression and stabilisation despite the underlying oncological diagnosis to prevent permanent neurological injury and to allow safe initiation of definitive chemotherapy. This case emphasises several important clinical considerations. Spinal lymphoma should be included in the differential diagnosis of pathological vertebral lesions, even in patients with a strong clinical history suggestive of infection. Although transpedicular biopsy is generally considered safe, clinicians should remain vigilant for delayed neurological deterioration in patients with pathological vertebral lesions, especially when vertebral collapse, epidural disease, or occult instability may be present. Finally, management of acute neurological compromise in spinal lymphoma requires a multidisciplinary approach, balancing timely surgical decompression with subsequent oncological treatment.
Acute CES occurring after transpedicular biopsy in a patient with spinal NHL is exceptionally rare and clinically devastating. Although a definitive causal relationship between the biopsy procedure and neurological deterioration cannot be established from a single case, this report highlights the importance of maintaining a high index of suspicion for delayed neurological deterioration after diagnostic spinal procedures, particularly in pathological vertebral lesions. Prompt recognition, urgent repeat imaging, and timely surgical decompression, when indicated, combined with appropriate oncological management, are essential to reduce the risk of irreversible neurological deficits.
Transpedicular biopsy is generally considered safe; however, patients with pathological vertebral lesions should be closely monitored for delayed neurological deterioration. New-onset lower limb weakness, worsening radiculopathy, saddle anaesthesia, urinary retention, constipation, or loss of anal tone after biopsy should prompt urgent neurological assessment and repeat imaging. Early recognition of evolving cauda equina syndrome and timely decompression, when indicated, may help prevent permanent neurological deficits.
References
- 1. Freeman C, Berg JW, Cutler SJ. Occurrence and prognosis of extranodal lymphomas. Cancer 1972;29:252-60. [Google Scholar] [PubMed]
- 2. Becker S, Babisch J, Venbrocks R, Katenkamp D, Wurdinger S. Primary non-Hodgkin lymphoma of the spine. Arch Orthop Trauma Surg 1998;117:399-401. [Google Scholar] [PubMed]
- 3. Lyons MK, O’Neill BP, Marsh WR, Kurtin PJ. Primary spinal epidural lymphoma: Clinical features, management, and prognosis. Neurosurgery 1992;30:456-61. [Google Scholar] [PubMed]
- 4. Mulligan ME, McRae GA, Murphey MD. Imaging features of primary lymphoma of bone. AJR Am J Roentgenol 1999;173:1691-7. [Google Scholar] [PubMed]
- 5. Boukobza M, Mazel C, Touboul E. Primary vertebral and spinal epidural non-Hodgkin’s lymphoma with spinal cord compression. Neuroradiology 1996;38:333-7. [Google Scholar] [PubMed]
- 6. Jain AK. Tuberculosis of the spine: A fresh look at an old disease. J Bone Joint Surg Br 2010;92:905-13. [Google Scholar] [PubMed]
- 7. Bhojraj SY, Nene AM. Lumbar spinal tumours: Diagnostic difficulties and surgical strategies. Spine (Phila., Pa. 1976) 2002;27:E410-5. [Google Scholar] [PubMed]
- 8. Lis E, Bilsky MH, Pisinski L, Boland P, Healey JH, O’Malley B, et al. Percutaneous CT-guided biopsy of osseous lesions of the spine in patients with known or suspected malignancy. AJNR Am J Neuroradiol 2004;25:1583-8. [Google Scholar] [PubMed]
- 9. Kornblum MB, Wesolowski DP, Fischgrund JS, Herkowitz HN. Computed tomography-guided biopsy of the spine. A review of 103 patients. Spine (Phila., Pa., 1976) 1998;23:81-5. [Google Scholar] [PubMed]
- 10. Gleave JR, Macfarlane R. Cauda equina syndrome: What is the relationship between timing of surgery and outcome? Br J Neurosurg 2002;16:325-8. [Google Scholar] [PubMed]
- 11. Adhikari P, Khadka S, Regmi PR, Shrestha A, Panta BR, Bhandari S, et al. Primary spinal non-Hodgkin lymphoma presenting as impending cauda equina syndrome: A case report. Ann Med Surg (Lond) 2022;83:104696. [Google Scholar] [PubMed]
- 12. Peng X, Wang Y, Chen Y, Chen L, He A, Liao W, et al. Primary non-Hodgkin’s lymphoma of the spine with neurologic compression treated by radiotherapy and chemotherapy alone or combined with surgical decompression. Oncol Rep 2009;21:1269-5. [Google Scholar] [PubMed]
- 13. Rathmell AJ, Gospodarowicz MK, Sutcliffe SB. Localised spinal epidural lymphoma: management and outcome. J Clin Oncol 1992;10:1502-9. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Adolescent Cauda Equina Secondary to Traumatic Lumbar Disc Herniation: A Rare Case Report with Review of Literature
August 1, 2026 Adolescent Cauda Equina Secondary to Traumatic Lumbar Disc Herniation: A Rare Case Report with Review of Literature June 1, 2026 Cauda Equina Syndrome Following Posterior Interbody Cage Migration after TLIF: A Rare Case Report
June 1, 2026 Cauda Equina Syndrome Following Posterior Interbody Cage Migration after TLIF: A Rare Case Report March 1, 2026 Acute Cauda Equina Syndrome Due to Primary Lumbar Spinal Hydatid Cyst: A Rare Case
March 1, 2026 Acute Cauda Equina Syndrome Due to Primary Lumbar Spinal Hydatid Cyst: A Rare Case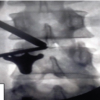 January 1, 2026 Outcomes of Unilateral Biportal Endoscopic Surgery for Prolapsed Intervertebral Disc: A Single-center Study
January 1, 2026 Outcomes of Unilateral Biportal Endoscopic Surgery for Prolapsed Intervertebral Disc: A Single-center Study