
We must be careful about atypical symptoms that can reveal an osteosarcoma.
Dr. Amine El Khassoui, Department of Pediatric Orthopedic, Mother and Child Unit, University Hospital Mohamed VI of Marrakech, Faculty of Medicine and Pharmacy, Cadi Ayyad University, Marrakech, Morocco. E-mail: a.elkhassoui@uca.ma
Abstract
Introduction: Osteosarcoma is the most common primary malignant bone tumor in childhood distinguished by its clinical aspects, epidemiological features, and radiological and histological findings. Around 10% of patients present with distant metastasis at the most frequent sites, which are lungs and bone. Furthermore, death rates for osteosarcoma have been declining by about 1.3% per year.
Case Report: We report the case of a 12-year-old child who presented to the emergency department with a large thigh hematoma, and after running all the necessary clinical investigations, it turned out to be secondary to femoral osteosarcoma.
Conclusion: In this case, our aim is to highlight the unusual clinical manifestations observed in a child with osteosarcoma, which can lead to a diagnosis delay and the subsequent impact on prognosis.
Keywords: Osteosarcoma, hematoma, swelling, diagnostic delay, fracture.
Bone cancer represents 5% of neoplasms in pediatric and adolescent patients, with osteosarcoma being the most common. Incidence peaks in adolescence, particularly during a growth spurt [1,2]. It can manifest in any bone, but the majority of cases arise from the metaphyses of long bones, with the distal femur affected in 40% of cases [3]. The cardinal symptom is persistent bone pain, often causing nighttime awakening, with or without the swelling [4]. However, patients with osteosarcoma may present a variety of clinical aspects. Non-specific symptoms can lead to a delay in diagnosis and the initiation of an inappropriate treatment. Meanwhile, radiological aspects of highly malignant osteosarcomas can be significant, suggesting the presence of malignancy [5]. To prevent further misdiagnosis and given the difficulties we faced in terms of both clinical aspects and radiological findings, we report the case of a 12-year-old male presenting with atypical symptoms for osteosarcoma.
We present the case of a 12-year-old male with a history of right femur fracture, treated with elastic stable intramedullary nailing (Figs. 1 and 2); 40 days before, he had presented to our department with a swelling of his right thigh which had been evolving for 10 days following a minor trauma (Fig. 3).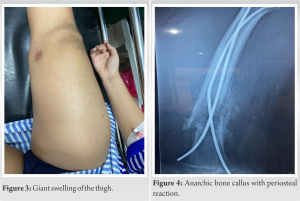
Clinically, the patient was conscious, apyretic, and in a stable condition. The swelling was warm, painful, worsening at night without any signs of inflammation on the anterior compartment of the right thigh resulting in functional impairment of his right lower limb.
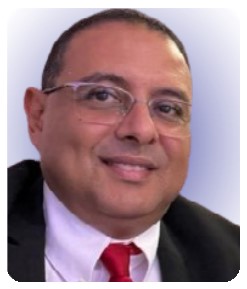
An ultrasound of the soft tissues was initially performed, revealing a large deep intramuscular hematoma in contact with the bone, measuring approximately 12 × 6 cm, with both anechoic and echogenic contents. Front and side radiographs of the right femur showed subtle lytic lesions at the fracture site, suggestive of ongoing bone healing (Fig. 4). A complete blood cell count revealed normocytic normochromic anemia (hemoglobin 8 g/dL), leukocytosis (16,000/mm3), and an elevated C-reactive protein level (43 mg/L). We performed a computed tomography angiography as we suspected a local etiology, but no active bleeding was observed. Initial surgical procedure was carried out, resulting in the evacuation of approximately 800 mL of serohemorrhagic fluid. The bone appeared intact, while there was capillary bleeding in the soft tissues. Within 48 h, there was recurrence of the hematoma, raising suspicions of hemostasis disorders. However, hemostasis tests, coagulation factor assays, and platelet aggregometry revealed no abnormalities. Due to the hematoma’s size increase, a magnetic resonance imaging of the right lower limb was preformed, revealing pathological femoral fracture associated with a large solid-cystic mass suggestive of malignant sarcoma. A second surgical evacuation of the hematoma was performed, as we also proceeded to remove the osteosynthesis material and right distal femur needle biopsy. The histological findings revealed a non-tumoral reactive bone tissue with hemorrhagic areas, trophic muscle fragments, and fibrosis. Further investigations focused on a local etiology due to the persistent hematoma and worsening general conditions. Despite multiple transfusions, the patient continued to have ongoing hemolysis, leading to carry out an arteriogram, which showed no abnormalities. Another surgical hematoma evacuation along with a second needle biopsy was ordered to establish diagnosis, revealing a highly pleomorphic malignant giant cell tumor proliferation with areas of osteogenesis, in addition to numerous cellular abnormalities and atypical mitoses. The diagnosis of high-grade osteosarcoma (grade 4) was confirmed after 1½ months of conducting clinical investigations. Chest computerized tomography and whole-body positron emission tomography were obtained for staging and revealed pulmonary metastasis. Our approach was to treat the patient with pre-operative chemotherapy to facilitate limb salvage operations. However, the patient succumbed to septic shock while undergoing neoadjuvant chemotherapy.
High-grade malignant osteosarcomas are aggressive tumors with a high metastatic potential, where even in early stages, pulmonary metastasis may exist [5,6]. Clinical manifestations are generally non-specific, characterized by chronic bone pain, a firm mass with collateral venous circulation or inflammatory signs and sometimes swelling that can increase in response to intralesional hemorrhage [3,4]. Pathological fractures can be an inaugural symptom occurring in 5–10% of patients, but in some cases, aggressive features are subtle, leading to diagnostic difficulties and delays [3,4,7]. Radiological aspects often suggest a rapid and aggressive progression without necessarily indicating its etiology. Osteolytic lesions with cortical destruction, periosteal appositions, are highly suspicious of being associated with a malignant process [8]. This case serves to exemplify the importance of recognizing the unusual clinical features responsible for the delay in diagnosing osteosarcoma, as it took approximately 1½ months to confirm, whether it has an impact on the patient’s outcome. Yao and Lin conducted a study that provided evidence showing that the misdiagnosis of osteosarcoma in children can be related to a seemingly benign symptomatology, such as a motion injury, which often leads to individual delay in seeking medical attention [6]. Other factors include professional delay, represented by atypical radiographic images, the short sensitivity of radiography for early detection of osteosarcomas, and less biopsy needle material, or sampling from a site without tumor cells [6]. We have not found any literature reviews describing similar cases to ours, however, there have been some case reports illustrating how the diverse clinical manifestations can result in diagnostic delays. DePalma et al. reported a case about a 5-year-old female who after suffering a small injury exhibited an antalgic gait and was initially diagnosed with left knee sprain due to her unremarkable X-rays and therefore was treated incorrectly. Persistent pain and further investigations confirmed the primary bone malignancy [9]. Another case also highlights the ambiguity of symptoms, as an 11-year-old girl showed an irreducible shoulder dislocation as an initial symptom. Open reduction was required revealing subperiosteal hemorrhage, an organized hematoma beneath the deltoid musculature, and alterations in the bone tissue, raising suspicions of a bone tumor. The diagnosis of osteosarcoma was established by histologic confirmation [10]. The ambiguity of symptoms of this highly malignant bone tumor as well as patient-related or doctor-related delays can lead to amputation, tumor recurrence, and the appearance of distant metastasis [6]. In our case, the patient was unable to undergo limb salvage surgery, as he passed away during his neoadjuvant chemotherapy. Therefore, the delay in diagnosing pediatric bone tumors which can be attached to various factors, leading surgeons and pathologists to make an incorrect diagnosis, gives rise to controversies surrounding professional errors [11]. The prognosis of osteosarcomas in the pediatric population has improved over the past 40 years, especially with the introduction of chemotherapy, leading to a long-term survival rate ranging from 25–30% to 70–80% [12,13]. Early diagnosis remains crucial for achieving local control and preventing the occurrence of metastasis resulting in poor prognosis, with a 5-year survival rate of approximately 20% [12,13]. However, several studies have reported that the prognosis of osteosarcomas and the presence of metastasis are not related to diagnostic delay [11]. From a different perspective, the finding from a study conducted by Yoshida et al. highlights the importance of consultation within 4 weeks of symptom onset as it can contribute to better prognosis [11]. Others have suggested that a short duration between the onset of symptoms and the confirmation of diagnosis is a factor in poor prognosis and increases the risk of metastasis [12,14]. This has been related to the rapid and aggressive evolution of the tumor, as well as tumor biology [12,14,15]. In other words, the interval between symptomatology and the time required to establish an osteosarcoma diagnosis does not have a significant impact on the disease progression, treatment effectiveness, and prognosis, which is remarkably good and does not seem to influence the patient’s outcome [12]. However, the prognosis for patients with metastatic osteosarcoma remains poor, with a 5-year survival rate of approximately 20% [12].
It is crucial for clinicians to be familiar with the signs and symptoms associated with osteosarcomas to minimize the risk of metastasis, tumor progression, and treatment delays. These tumors occur most often in active adolescents, initial complaints may be attributed to a sports injury or sprain, any deep bone pain, often causing nighttime awakening, or joint pain not responding to conservative therapy within a reasonable time should be investigated thoroughly. However, the time delay may not have a significant impact on the tumor’s subsequent prognosis, and the histological nature remains the principal factor implicated in the unfavorable evolution.
Many factors can be related to the evolution of osteosarcoma; an aggressive type or a delay in diagnosis may lead to poor prognosis.
References
- 1.Parkin DM, Stiller CA, Nectoux J. International variations in the incidence of childhood bone tumours. Int J Cancer 1993;53:371-6. [Google Scholar | PubMed]
- 2.Arndt CA, Crist WM. Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-52. [Google Scholar | PubMed]
- 3.Dahan M, Anract P, Babinet A, Larousserie F, Biau D. Proximal femoral osteosarcoma: Diagnostic challenges translate into delayed and inappropriate management. Orthop Traumatol Surg Res 2017;103:1011-5. [Google Scholar | PubMed]
- 4.Fletcher CD, Unni KK, Mertens F. Pathology and Genetics of Tumors of Soft Tissue and Bone. Lyon: International Agency for Research on Cancer; 2002. p. 376-419. [Google Scholar | PubMed]
- 5.Hauptmann K, Melcher I, Schaser KD. Differenzialdiagnose intramedullärer Osteosarkome. Pathologe 2008;29:240-4. [Google Scholar | PubMed]
- 6.Yao Y, Lin F. Misdiagnosis and Mistreatment for Osteosarcoma: Analysis of Cause and its Strategy. Osteosarcoma. London: InTech; 2012. p. 86-92. [Google Scholar | PubMed]
- 7.Demiroz S, Oktem F, Celik A, Erdogan O, Ozkan K, Gurkan V. Evaluation of patients with pathological fractures treated by standard trauma principles but neglecting the underlying malign bone disease. Injury 2022;53:3736-41. [Google Scholar | PubMed]
- 8.Ndour O, Alumeti DM, Fall M, Fall AF, Diouf C, Ndoye NA, et al. Epidiological, diagnosis and therapeutic aspects of osteosarcoma in university hospital of Aristide le Dantec, Dakar: About 16 cases. Pan Afr Med J 2013;14:104. [Google Scholar | PubMed]
- 9.DePalma M, Gupta S, Nguyen J, Talwar D, Arkader A, Wells L. Do not miss the tumor: A novel presentation of osteosarcoma. Case Rep Pediatr 2021;2021:5531238. [Google Scholar | PubMed]
- 10.Chun DI, Yoo JH. A case of irreducible shoulder dislocation as an initial manifestation of osteosarcoma of the proximal humerus. Eur J Orthop Surg Traumatol 2011;21:341-4. [Google Scholar | PubMed]
- 11.Yoshida S, Celaire J, Pace C, Taylor C, Kaneuchi Y, Evans S, et al. Delay in diagnosis of primary osteosarcoma of bone in children: Have we improved in the last 15 years and what is the impact of delay on diagnosis? J Bone Oncol 2021;28:100359. [Google Scholar | PubMed]
- 12.Ferrari A, Lo Vullo S, Giardiello D, Veneroni L, Magni C, Clerici CA, et al. The sooner the better? How symptom interval correlates with outcome in children and adolescents with solid tumors: Regression tree analysis of the findings of a prospective study. Pediatr Blood Cancer 2016;63:479-85. [Google Scholar | PubMed]
- 13.Goedhart LM, Gerbers JG, Ploegmakers JJ, Jutte PC. Delay in diagnosis and its effect on clinical outcome in high-grade sarcoma of bone: A referral oncological centre study. Orthop Surg 2016;8:122-8. [Google Scholar | PubMed]
- 14.Bacci G, Ferrari S, Longhi A, Forni C, Zavatta M, Versari M, et al. High-grade osteosarcoma of the extremity: Differences between localized and metastatic tumors at presentation. J Pediatr Hematol Oncol 2002;24:27-30. [Google Scholar | PubMed]
- 15.Goyal S, Roscoe J, Ryder WD, Gattamaneni HR, Eden TO. Symptom interval in young people with bone cancer. Eur J Cancer 2004;40:2280-6. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Novel Technique for Fracture Non-Union in Children – A Case Report
April 1, 2026 Novel Technique for Fracture Non-Union in Children – A Case Report January 1, 2026 Lumbar Hyperextension Fracture after Direct Anterior Total Hip Arthroplasty
January 1, 2026 Lumbar Hyperextension Fracture after Direct Anterior Total Hip Arthroplasty January 1, 2026 Enhancing Functional Outcomes in Distal End Radius Fracture Rehabilitation
January 1, 2026 Enhancing Functional Outcomes in Distal End Radius Fracture Rehabilitation December 1, 2025 Fixation of Distal Fibula Fractures Associated with Extra-articular Distal One-third Tibia Fractures – Is It Necessary?
December 1, 2025 Fixation of Distal Fibula Fractures Associated with Extra-articular Distal One-third Tibia Fractures – Is It Necessary?