
Neglected bilateral clubfoot clubhand deformity is a mesomelic type of dysplasia that is characterized by disproportionate shortness of the middle segment of all limbs and is a form of short-limb dwarfism. We describe a patient with neglected bilateral clubfoot clubhand deformity with findings like bilateral dysplasia of the radius and ulna, bilateral dysplastic tibia and fibula, dysplasia of the elbow and ankle joints
Dr. Aakarsh Aggarwal, Department of Orthopaedics, All India Institute of Medical Sciences Jodhpur - 342005, Rajasthan, India. E-mail: aakarshaggarwal1@gmail.com
Abstract
Introduction: Neglected bilateral clubfoot clubhand deformity is a mesomelic type of dysplasia that is characterized by disproportionate shortness of the middle segment of all limbs and is a form of short-limb dwarfism. Affected individuals are clinically of normal stature with particularly short mesomelic segments with nearly symmetric limb abnormalities.
Case Report: The patient was a 20-year-old male Indian who came to outpatient department for cosmetic purpose. Upper limb abnormalities include short forearm, and elbow joints which are broad and deformed with limited flexion-extension range of motion and decreased pronosupination of the forearms. The hands are normal in appearance. The foot is also affected and deformed. The fibulae are malformed and long in relation to the tibiae. Both bones, tibia, and fibula are dysplastic. The atypical foot deformity seen in this patient is characterized by a severe equinovarus component. He is able to do his activities of daily living and can do activities such as gripping, holding a pen/cup, opening a door, and writing on paper comfortably. He is able to walk normally without any support. This patient has normal stature, normal systemic examination, and normal chromosomes.
Conclusion: The neglected bilateral clubfoot clubhand deformity a type of mesomelic dysplasia was the most likely diagnosis in our patient. Disorders involving Nievergelt syndrome and mesomelic dwarfism were considered but none were likely possibilities. Our patient had the malformed fibulae and tibiae, and the severe equinovarus deformity of the feet. There were triangular shaped ulnae which were deficient distally, and the radii were bowed. Unlike Nievergelt syndrome, our patient did not have a severe deformity of hands and fingers. He is functionally sound and able to do his activities of daily living and can do activities such as gripping, holding a pen/cup, opening a door, and writing on paper comfortably. He is able to walk normally without any support. These features have not been previously described in literature leading to our diagnosis of neglected bilateral clubfoot clubhand deformity.
Keywords: Bilateral clubfoot deformity, bilateral clubhand deformity, mesomelic dysplasia.
Neglected bilateral clubfoot clubhand deformity includes skeletal disorders characterized by short middle segments of the limbs. Along with this feature, the individual disorders in this category demonstrate different patterns of presentation, clinical severity, specific radiologic changes, and associated skeletal manifestations. Affected individuals are clinically of normal stature with particularly short mesomelic segments with nearly symmetric limb abnormalities. Upper limb abnormalities include short forearm, and elbow joints which are broad and deformed with limited flexion-extension range of motion and decreased pronosupination of the forearms. The hands are normal in appearance. In addition, roentgenograms typically showed dysplasia of the elbow joints and dysplastic forearm bones. Clinically, the foot is also affected and deformed. The fibulae are malformed and long in relation to the tibiae. Both bones, tibia, and fibula are dysplastic [1]. The atypical foot deformity seen in this patient is characterized by a severe equinovarus component. Roentgenograms also show dysplasia of the ankle joints and diastasis between the 1st and 2nd ray. Several individuals with Nievergelt syndrome [2], symphalangism, carpal fusion, atypical clubfeet with tarsal fusion, and dislocation of the radial head have been reported under the broad term of Nievergelt-pearlman syndrome [3] and have features similar to the patient described in this report but all these will not be considered here. We report on a patient with neglected bilateral clubfoot clubhand deformity, who exhibits characteristics consistent with mesomelic dysplasia.
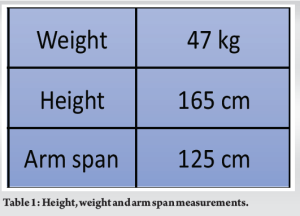
At the first visit, the patient was a 20-year-old male Indian who came to outpatient department for cosmetic purpose. He was born at term by normal spontaneous vertex vaginal delivery. Gestation, labor, and delivery were uneventful. The postnatal course was also uneventful. Developmentally, he achieved all milestones without delay. He had no feeding problems. His general health was good including normal respiratory, cardiac, gastroenterology, and urogenital system. Normal central nervous system and spine on examination. No history of seizure disorder or intensive care unit admission in the past. The family history was unremarkable and there was no evidence of consanguinity. Physical examination was normal with the patient and only complaints of cosmesis and deformity with no functional limitation (Table 1).
He is able to do his activities of daily living and can do activities such as gripping, holding a pen/cup (Fig. 1), opening a door, and writing on paper comfortably. He is able to walk normally without any support (Fig. 2). Due to the deformity of the foot, he bears weight on his first and second toes causing diastasis between the first and second rays of his foot bilaterally.


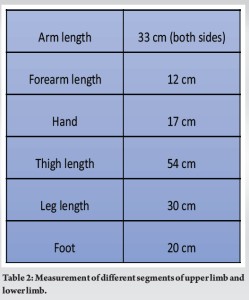
His head and face have normal morphology. Eyes, ears, nose, mouth, and oropharynx were normal. The neck appeared normal in length. The chest, heart, abdomen, and genitalia were normal. The skin was normal. The cranial nerves were grossly intact; there was good control of the trunk and head. Abnormal articulation of the elbows, wrists, and ankles was seen during joints examination. The upper arm was normal (Table 2). The elbow joints were wide with restricted flexion and extension. The forearms were short, broad, and bowed. Pronation and supination were also limited. The hand had normal anatomy with no deformity in the hand and fingers (Fig. 3a).
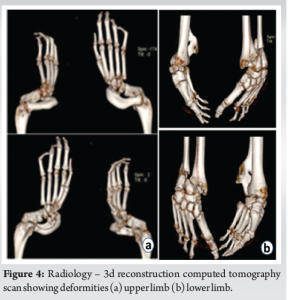
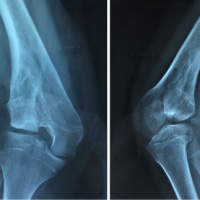
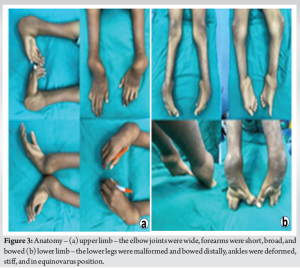 The upper leg was normal. The knee joint was normal with normal flexion and extension. The lower legs were malformed and bowed distally. The ankles on examination were deformed, stiff, and in an equinovarus position. The feet were normal grossly with diastasis between 1st and 2nd ray and in extreme plantar flexion. There was limited dorsiflexion (Fig. 3b). Chromosome analysis with trypsin Giemsa staining was performed on peripheral lymphocyte cultures and demonstrated normal chromosomes. A skeletal survey showed a normal skull and normal chest. The lateral spine showed normal anatomy of the cervical, dorsal, and lumbar spine. The pelvic bones and sacral vertebrae appeared normal. In the upper limbs, the radii were curved and short with radial heads dislocated; the ulnae had thickened proximal ends, short and triangular in shape. Normal carpal bones and metacarpals were seen bilaterally. Radiographs of the lower limbs demonstrated normal femora. The leg demonstrated a distally thickened tibia and malformed fibula (Fig. 4).
The upper leg was normal. The knee joint was normal with normal flexion and extension. The lower legs were malformed and bowed distally. The ankles on examination were deformed, stiff, and in an equinovarus position. The feet were normal grossly with diastasis between 1st and 2nd ray and in extreme plantar flexion. There was limited dorsiflexion (Fig. 3b). Chromosome analysis with trypsin Giemsa staining was performed on peripheral lymphocyte cultures and demonstrated normal chromosomes. A skeletal survey showed a normal skull and normal chest. The lateral spine showed normal anatomy of the cervical, dorsal, and lumbar spine. The pelvic bones and sacral vertebrae appeared normal. In the upper limbs, the radii were curved and short with radial heads dislocated; the ulnae had thickened proximal ends, short and triangular in shape. Normal carpal bones and metacarpals were seen bilaterally. Radiographs of the lower limbs demonstrated normal femora. The leg demonstrated a distally thickened tibia and malformed fibula (Fig. 4).
Both feet showed normal tarsal bones and all five metatarsals were normally developed. First and 2nd rays were splayed. All five toes had normal anatomy with widened web space between 1st and 2nd toes.
The neglected bilateral clubfoot clubhand deformity a type of mesomelic dysplasia [4,5] was the most likely diagnosis in our patient. Disorders involving Nievergelt syndrome and mesomelic dwarfism were considered but none were likely possibilities [6-9]. The patient described by Solonen and Sulamaa [10] shared many characteristics except that his feet valgus deformity, and flexion contracture of the proximal interphalangeal joints of fingers 1–4. Within the hands, there were normal bones and ulnarly deviated wrist, and no synostosis was seen in the tarsal or metatarsal bones. In another report, bilateral flexion deformities of toes 4–5 in affected children were reported by Young and Wood [11]. Our patient had the malformed fibulae and tibiae and the severe equinovarus deformity of the feet. There were triangular shaped ulnae which were deficient distally, and the radii were bowed. The radioulnar synostosis was not present radiographically. Clinically, a limited range of movement of the elbow joints was observed. Unlike Nievergelt syndrome, our patient did not have severe deformity of hands and fingers, although diastasis was present between 1st and 2nd toes. On average, the group of findings seen in this patient most closely resembles the neglected bilateral clubfoot clubhand deformity. As described previously, this patient has normal stature, normal systemic examination, and normal chromosomes. He is functionally sound and able to do his activities of daily living and can do activities such as gripping, holding a pen/cup, opening a door, and writing on paper comfortably. He is able to walk normally without any support. These features have not been previously described in literature leading to our diagnosis of neglected bilateral clubfoot clubhand deformity.
The present case is a neglected bilateral clubfoot clubhand deformity which is a type of mesomelic dysplasia. Disorders involving Nievergelt syndrome and mesomelic dwarfism were considered but none were likely possibilities. Our patient had the malformed fibulae and tibiae, and the severe equinovarus deformity of the feet. There were triangular shaped ulnae which were deficient distally, and the radii were bowed. Unlike Nievergelt syndrome, our patient did not have a severe deformity of the hands and fingers. He is functionally sound and able to do his activities of daily living comfortably. He is able to walk normally without any support. These features have not been previously described in literature leading to our diagnosis of neglected bilateral clubfoot clubhand deformity.
The neglected bilateral clubfoot clubhand deformity is a type of mesomelic dysplasia and is an uncommon case. The patient had deformities of bilateral upper and lower limbs but he is able to do his activities of daily living and is able to walk normally without any support. This patient has normal stature, normal systemic examination, and normal chromosomes.
References
- 1.Plauchu H, Maisonneuve D, Floret D. Le nanisme acro-coxo-mésomélique: Variété nouvelle de nanisme récessif autosomique [Acro-coxo-mesomelic dwarfism: A new variety of autosomal recessive dwarfism]. Ann Genet 1984;27:83-7. [French] [Google Scholar | PubMed]
- 2.Hess OM, Goebel NH, Streuli R. Familiärer mesomeler Kleinwuchs (Nievergelt-Syndrom) [Familial mesomelial dwarfism (Nievergelt syndrome)]. Schweiz Med Wochenschr 1978;108:1202-6. [German] [Google Scholar | PubMed]
- 3.Murakami Y. Nievergelt-pearlman syndrome with impairment of hearing. Report of three cases in a family. J Bone Joint Surg Br 1975;57:367-72. [Google Scholar | PubMed]
- 4.Kaitila I, Leisti JT, Rimoin DL. Mesomelic skeletal dysplasias. Clin Orthop Relat Res 1976;114:94-106. [Google Scholar | PubMed]
- 5.Blockey NJ, Lawrie IH. An unusual symmetrical distal limb deformity in siblings. J Bone Joint Surg Br 1963;45:745-7. [Google Scholar | PubMed]
- 6.Petrella R, Ludman MD, Rabinowitz JG, Gilbert F, Hirschhorn K. Mesomelic dysplasia with absence of fibulae and hexadactyly: Nievergelt syndrome or new syndrome? Am J Med Genet 1990;37:10-4. [Google Scholar | PubMed]
- 7.Carter AR, Currey HL. Dyschondrosteosis (mesomelic dwarfism)--A family study. Br J Radiol 1974;47:634-40. [Google Scholar | PubMed]
- 8.Kaufmann HJ. Mesomelic dwarfism. Seinin Roentgenol 1973;8:226. [Google Scholar | PubMed]
- 9.Langer LO Jr. Mesomelic dwarfism of the hypoplastic ulna, fibula, mandible type. Radiology 1967;89:654-60. [Google Scholar | PubMed]
- 10.Solonen KA, Sulamaa M. Nievergelt syndrome and its treatment: A case report. Ann Chir Gynaecol Fenn 1958;47:142-7. [Google Scholar | PubMed]
- 11.Young LW, Wood BP. Nievergelt syndrome (mesomelic dwarfism-type Nievergelt). Birth Defects Orig Artic Ser 1974;10:81-6. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 November 10, 2021 Reconstruction of limb deformity occurring after infantile meningococcal infection: a case report
November 10, 2021 Reconstruction of limb deformity occurring after infantile meningococcal infection: a case report January 1, 2026 The Importance of Closed Reduction and Internal Fixation done with Intramedullary Implants in Pathological Fractures – A Case Series
January 1, 2026 The Importance of Closed Reduction and Internal Fixation done with Intramedullary Implants in Pathological Fractures – A Case Series June 1, 2026 Reliability of Singh’s Index and Calcaneal Index in Assessing Osteoporosis Compared with Quantitative Ultrasound Bone Mineral Density
June 1, 2026 Reliability of Singh’s Index and Calcaneal Index in Assessing Osteoporosis Compared with Quantitative Ultrasound Bone Mineral Density March 2, 2019 Chronic Systemic Metal Ion Toxicity from Wear on a Revised Cobalt-chromium Trunnion
March 2, 2019 Chronic Systemic Metal Ion Toxicity from Wear on a Revised Cobalt-chromium Trunnion