
Singh’s Index and Calcaneal Index, though inexpensive and easy to use, suffer from poor reproducibility and weak correlation with quantitative BMD, limiting their clinical utility. Quantitative ultrasound (QUS) emerges as a more reliable, affordable, and practical alternative for osteoporosis screening, especially in low- and middle-income countries where access to DEXA is restricted.
Dr. Vipin Kumar Mishra, Department of Orthopaedics, Government Medical College, Satna, Madhya Pradesh, India. E-mail: vipin9926@gmail.com
Abstract
Introduction: Osteoporosis is a major global health problem characterised by reduced bone mass and increased fracture risk. Dual-energy X-ray absorptiometry is the gold standard for bone mineral density (BMD) measurement; however, its cost and limited accessibility restrict its use in low- and middle-income countries. Singh’s Index and Calcaneal Index, based on trabecular bone patterns on radiographs, have been proposed as inexpensive alternatives.
Materials and Methods: A prospective study was conducted during an orthopaedic camp in October 2014. A total of 120 skeletally mature patients underwent hip and calcaneal radiographs, which were independently graded by four orthopaedic surgeons using Singh’s and Calcaneal indices. BMD was measured using quantitative ultrasound (QUS) at the femoral neck and calcaneus. Agreement was assessed using weighted Cohen’s kappa statistics, and the correlation between indices and BMD was analysed.
Results: A prospective study was conducted during an orthopaedic camp in October 2014. A total of 120 skeletally mature patients underwent hip and calcaneal radiographs, which were independently graded by four orthopaedic surgeons using Singh’s and Calcaneal indices. BMD was measured using quantitative ultrasound (QUS) at the femoral neck and calcaneus. Agreement was assessed using weighted Cohen’s kappa statistics, and the correlation between indices and BMD was analysed.
Conclusion: Singh’s Index and Calcaneal Index demonstrate poor reproducibility and weak correlation with quantitative BMD. While inexpensive, their subjectivity limits clinical utility. QUS offers a more reliable, affordable alternative for osteoporosis screening in resource-limited settings.
Keywords: Osteoporosis, bone mineral density, dual-energy X-ray absorptiometry, Singh’s Index
Osteoporosis is a systemic skeletal disease characterised by low bone mass and microarchitectural deterioration of bone tissue, leading to increased fragility and fracture risk [1]. It is a major public health problem worldwide, affecting both developed and developing nations [2]. The disease contributes significantly to morbidity, mortality, and healthcare costs. Globally, osteoporosis affects approximately 200 million individuals, with prevalence rising sharply after menopause in women and later in men [3]. In the United States alone, an estimated 44 million people aged 50 and older have low bone mass or osteoporosis, accounting for 55% of this population [4]. Hip and vertebral fractures are particularly devastating, often resulting in chronic pain, disability, and increased mortality [5]. Bone mineral density (BMD) measurement is the single best predictor of fracture risk [5]. Techniques for assessing BMD include dual-energy X-ray absorptiometry (DEXA), quantitative computed tomography, quantitative ultrasound (QUS), and radiographic methods such as Singh’s Index and Calcaneal Index [6]. While DEXA remains the reference standard, its limited availability in low-resource settings necessitates the exploration of alternative methods [6]. Singh’s Index, introduced in 1970, grades trabecular bone patterns in the proximal femur on plain radiographs [1]. Similarly, the Calcaneal Index evaluates trabecular patterns in the calcaneus [7]. Both are inexpensive and widely used, but concerns exist regarding their reliability and correlation with true bone mass [8]. This study aims to evaluate the reproducibility and diagnostic accuracy of Singh’s Index and Calcaneal Index compared with QUS-derived BMD, focusing on intraobserver and interobserver variability.
Study design and setting:
A prospective observational study was conducted at our institute with a study duration of 3 months. Ethical permission was taken from the IEC before the onset of the study (GMC/105/INST/2025). Informed consent was obtained from all participants before their inclusion in the study. The confidentiality of patient data was maintained at all stages of the study, and only aggregate data were reported.
Participants:
- Inclusion criteria: Patients aged ≥18 years, skeletally mature.
- Exclusion criteria: Lower limb amputees, skeletally immature individuals, patients with liver, thyroid, or parathyroid diseases, chronic corticosteroid or anticonvulsant use, prolonged alcohol intake, or drug abuse.
Sample size:
A total of 139 patients were initially enrolled; after applying exclusion criteria, 120 patients were included. The mean age was 46.2 years (range 23–59).
Radiographic evaluation:
- Hip radiographs: Anteroposterior view of right hip
- Calcaneal radiographs: Lateral view of right calcaneus.
- Indices applied:
- Singh’s Index (Grades I–VI): Based on trabecular patterns in the proximal femur
- Calcaneal Index (Grades I–V): Based on trabecular patterns in the calcaneus.
Four orthopaedic surgeons, each with ≥2 years of postgraduate experience, independently graded radiographs using reference charts.
BMD measurement:
QUS was performed at the right femoral neck and calcaneus. BMD was expressed as T-scores.
Observer variability:
- Intraobserver agreement: Each surgeon regraded radiographs at 1, 2, and 3 months.
- Interobserver agreement: Comparison across surgeons at each time point.
- Statistical analysis: Weighted Cohen’s kappa statistics.
Interpretation of Kappa values:
- Poor: 0.00–0.20
- Fair: 0.21–0.40
- Moderate: 0.41–0.60
- Substantial: 0.61–0.80
- Almost perfect: 0.81–1.00.
Correlation analysis:
Correlation between Singh’s Index, Calcaneal Index, and QUS-derived BMD was calculated using Pearson and Spearman coefficients.
Demographic characteristics:
Out of 139 patients initially enrolled, 120 met the inclusion criteria and were analyzed. The mean age was 46.2 years (range 23–59 years). The majority of participants were female, and postmenopausal women formed a significant proportion of the study population. This demographic distribution reflects the higher prevalence of osteoporosis among women, particularly after menopause.
BMD (QUS findings):
QUS measurements revealed a wide distribution of T-scores across the study population:
- Normal bone density (T-score ≥−1): 38 patients (31.7%)
- Osteopenia (T-score between −1 and −2.5): 52 patients (43.3%)
- Osteoporosis (T-score ≤−2.5): 30 patients (25%).
This distribution highlights the significant burden of low bone mass in the study population, with nearly 70% of patients demonstrating osteopenia or osteoporosis.
Both indices show clustering in intermediate grades (III–V), reflecting moderate trabecular loss consistent with osteopenia. Severe trabecular loss (Grade I–II) was less common but present in 17% of Singh’s Index cases and 23% of Calcaneal Index cases. Normal trabecular patterns were observed in 18% (Singh) and 22% (Calcaneal), highlighting variability between sites as shown in Table 1.
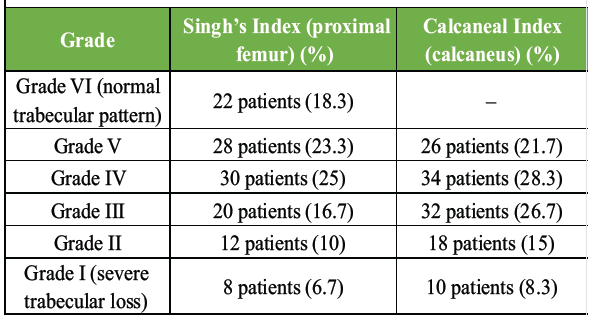
Table 1: Distribution of Singh’s Index and Calcaneal Index grading
Intraobserver agreement was consistently higher, indicating that individual observers were relatively reliable when grading radiographs over time. Interobserver agreement was weaker, reflecting significant variability between different observers in applying grading criteria. Both indices demonstrated subjectivity, with Singh’s Index showing slightly better intraobserver consistency but poor reproducibility across observers, as shown in Table 2.
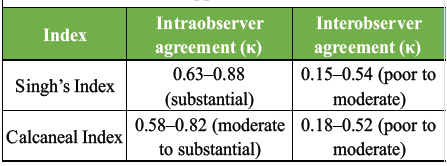
Table 2: Intraobserver and interobserver agreement (Kappa values)
Correlation between indices and QUS-derived BMD:
Correlation analysis revealed weak associations:
- Singh’s Index versus QUS BMD: Pearson r = 0.28 (P > 0.05)
- Calcaneal Index versus QUS BMD: Pearson r = 0.32 (P > 0.05).
Neither index demonstrated a statistically significant correlation with quantitative BMD. Patients with similar Singh or Calcaneal grades often had markedly different QUS T-scores, highlighting the limited diagnostic accuracy of these indices.
Osteoporosis is a silent disease until fractures occur, making early detection critical. While DEXA is the gold standard for BMD measurement, its limited availability in low- and middle-income countries has prompted interest in inexpensive radiographic indices such as Singh’s Index and Calcaneal Index. Previous studies have reported that Singh’s Index and Calcaneal Index are viable alternatives for assessing bone health, particularly in settings lacking access to DEXA or QUS scans [9]. Our study found poor interobserver agreement and weak correlation with QUS-derived BMD, consistent with much of the literature. In our study, intraobserver agreement was substantial (κ = 0.63–0.88), but interobserver agreement was poor to moderate (κ = 0.15–0.54). This reflects the subjective nature of trabecular grading. As per the study done by Cockshott and Park, the interobserver agreement was lower for Singh’s Index than for the Calcaneal Index, possibly because of the influence of femoral rotation in radiographs [10]. The Calcaneal Index evaluates trabecular patterns in the calcaneus, another site rich in cancellous bone. Govindharaaju et al. (2023) found a weak correlation between Singh’s and calcaneal indices in patients with fragility fractures, reinforcing concerns about their diagnostic accuracy [11]. Our study demonstrated weak correlations between both indices and QUS-derived BMD (Pearson r = 0.28–0.32, P > 0.05). This aligns with findings by Soontrapa and Soontrapa (2005), who reported poor reliability and diagnostic value of Singh’s Index in screening femoral neck osteoporosis [12]. The primary advantage of Singh’s and calcaneal indices is cost-effectiveness and accessibility. In resource-limited settings, where DEXA is unavailable, these indices may provide a rough qualitative estimate of bone loss. However, their limitations are significant, as grading depends heavily on observer interpretation. Patients with similar grades often have different densitometry results. Positioning, film type, and exposure parameters affect it. QUS offers a promising alternative. It is portable, inexpensive, radiation-free, and provides objective BMD values. Studies have shown QUS to correlate reasonably well with DEXA, particularly at the calcaneus. In our study, QUS provided reproducible results, underscoring its potential as a screening tool in resource-limited settings. Given the poor reproducibility and weak correlation of Singh’s and Calcaneal indices with quantitative BMD, reliance on these methods alone is not advisable. However, in settings where DEXA is unavailable, they may serve as preliminary screening tools, provided their limitations are acknowledged. Integration of QUS into screening programmes could significantly improve diagnostic accuracy and reduce fracture risk through earlier intervention. Further research should focus on large-scale validation of QUS against DEXA in diverse populations and development of standardised radiographic grading protocols to reduce subjectivity.
Our study reinforces the limited reliability of Singh’s and Calcaneal indices in assessing osteoporosis. While inexpensive, their subjectivity and poor correlation with quantitative BMD undermine clinical utility. QUS emerges as a more reliable, affordable alternative, particularly in resource-limited settings.
Quantitative Ultrasound (QUS) of the calcaneus provides a significantly more reliable, objective, and accurate evaluation for osteoporosis pre-screening than the radiographic Singh’s Index and Calcaneal Index. While both radiographic indices offer a cost-effective alternative for structural screening in extreme resource-poor settings, they suffer from high observer subjectivity and poor correlation with true bone mineral density
References
- 1. Sølling AS, Langdahl BL, Cosman F. Recent advances in osteoporosis therapeutics. Annu Rev Med 2026;77:433-48. [Google Scholar] [PubMed]
- 2. Gregson CL, Armstrong DJ, Avgerinou C, Bowden J, Cooper C, Douglas L, et al. The 2024 UK clinical guideline for the prevention and treatment of osteoporosis. Arch Osteoporos 2025;20:119. [Google Scholar] [PubMed]
- 3. Zhang X, Liang Y, Zhang F, Liu X. Osteoporosis: Molecular pathogenesis and therapeutic interventions. Mol Biomed 2025;6:98. [Google Scholar] [PubMed]
- 4. Luo J, Li L, Shi W, Xu K, Shen Y, Dai B. Oxidative stress and inflammation: Roles in osteoporosis. Front Immunol 2025;16:1611932. [Google Scholar] [PubMed]
- 5. Wilson BM, Wilson AB, Kraemer M, Bowker R, Patel AL, Sumner DR. Bone mineral density deficits in individuals born preterm persist through young adulthood: A systematic review and meta-analysis of DXA studies. Bone 2025;198:117519. [Google Scholar] [PubMed]
- 6. Nehls F, Schläppi M, Madjdpour C, Meier C, Wahl P. Blood loss in primary total hip arthroplasty occurs mainly postoperatively, but current formulas for calculating blood loss are inaccurate: A retrospective study of 208 cases. Arch Orthop Trauma Surg 2025;145:283. [Google Scholar] [PubMed]
- 7. Cai S, Gao J, Li C, Lu F, Hu D, Luo X, et al. Association of body mass index and bone mineral density in postmenopausal women: A systematic review and meta-analysis. Ann Med 2025;57:2561227. [Google Scholar] [PubMed]
- 8. Singh M, Nagrath AR, Maini PS. Changes in trabecular pattern of the upper end of the femur as an index of osteoporosis. J Bone Joint Surg Am 1970;52:457-67. [Google Scholar] [PubMed]
- 9. Jhamaria NL, Lal KB, Udawat M, Banerji P, Kabra SG. The trabecular pattern of the calcaneum as an index of osteoporosis. J Bone Joint Surg Br 1983;65:195-8. [Google Scholar] [PubMed]
- 10. Cockshott WP, Park WM. Observer variation in skeletal radiology. Skeletal Radiol 1983;10:86. [Google Scholar] [PubMed]
- 11. Govindharaaju R, Mathew J, Joseph D, Akshay Kumar NS, Vignesh R. Correlation of singh’s index with the calcaneal index in the assessment of osteoporosis in patients with distal radius fragility fractures. Int J Med Pharm Res 2025;6:633-43. [Google Scholar] [PubMed]
- 12. Soontrapa S, Soontrapa S. Modified Singh index in diagnosing femoral neck osteoporosis. J Med Assoc Thai 2011;94 Suppl 5:S79-83. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Assessment of Osteoporotic Fracture Risk in Patients above 50 Years Using Quantitative Ultrasonography and Fracture Risk Assessment Tool: A Cross-sectional Study
July 1, 2026 Assessment of Osteoporotic Fracture Risk in Patients above 50 Years Using Quantitative Ultrasonography and Fracture Risk Assessment Tool: A Cross-sectional Study March 1, 2026 Risk Factors for Osteoporotic Vertebral Fractures in Postmenopausal Women: A Cross-Sectional Study
March 1, 2026 Risk Factors for Osteoporotic Vertebral Fractures in Postmenopausal Women: A Cross-Sectional Study December 1, 2025 Utilization of Quantitative Ultrasound Methods for Bone Mass Density Measurement in General Population – An Observational Study
December 1, 2025 Utilization of Quantitative Ultrasound Methods for Bone Mass Density Measurement in General Population – An Observational Study August 1, 2026 Radiological Outcomes of Reamed Short Proximal Femoral Nailing in Intertrochanteric Fractures in Patients Aged 50 Years and Above
August 1, 2026 Radiological Outcomes of Reamed Short Proximal Femoral Nailing in Intertrochanteric Fractures in Patients Aged 50 Years and Above