
While both radiofrequency and microwave ablation provide highly effective, minimally invasive pain relief for osteoid osteoma, microwave ablation offers faster and broader tumor necrosis; however, it requires strict procedural precautions to avoid adjacent thermal injury due to its rapid heat generation.
Dr. Dijoe Davis, Department of Orthopaedics, Amala Institute of Medical Sciences, Amalanagar, Thrissur – 680555, Kerala, India. E-mail: dijoedavis@amalaims.org
Abstract
Introduction: Osteoid osteoma is a benign bone tumour that commonly manifests in the lower extremities and causes significant pain. Contemporary treatment for this condition has shifted toward the use of percutaneous ablation techniques. In this study, we aimed to evaluate the efficacy and safety of microwave ablation in patients with osteoid osteoma.
Materials and Methods: This retrospective study analysed 35 patients with osteoid osteoma treated using microwave ablation between June 2019 and June 2025. Patient demographics and clinical characteristics, such as tumour location, pain levels (assessed using the Visual Analogue Scale [VAS]), complications, and hospital stay, were recorded and analysed using descriptive statistics.
Results: The average patient age was 18.08 ± 8.6 years, and the proximal femur was the most commonly affected site (9/35 patients [27%]). Microwave ablation significantly reduced pain in 34 of 35 patients (97.1%), with average VAS scores decreasing from 7.4 ± 0.94 to 1.9 ± 0.7 after the procedure. Complications occurred in 5 of 35 patients (14.3%), and the average hospital stay was 3 days.
Conclusion: Our retrospective analysis showed that microwave ablation helped achieve significant pain reduction in patients with osteoid osteoma. While the procedure demonstrates efficacy, caution is necessary to minimise the risk of thermal injury to surrounding non-target tissues.
Keywords: Bone cancer, osteoid osteoma, radiofrequency ablation, microwave radiation.
Tumour ablation, which employs thermal or chemical agents for tumour eradication, has been in clinical use for approximately a century [1]. Among the various available ablative techniques, including cryoablation, ethanol ablation, laser ablation, and radiofrequency ablation (RFA), microwave ablation is the latest addition to the therapeutic arsenal [2]. The application of microwave radiation, characterised by electromagnetic waves with a minimum frequency of 900 MHz, has evolved since its initial use in radar communication [3]. In particular, Percy Spencer’s discovery of the heating properties of microwaves led to the invention of the microwave oven [4]. The interstitial application of microwave antennas for tumour ablation commenced around 1970, primarily in the context of hepatocellular carcinoma treatment [5]. Osteoid osteoma is a painful benign bone tumour primarily manifesting in the bones of the lower extremities. Osteoid osteoma accounts for 10–14% of all benign bone tumours and 2–3% of primary bone tumours [6]. It was initially described by Bergstrand in 1930 and was further characterised by Jaffe in 1935 [7]. Its hallmark is the presence of a centrally located nidus measuring <1.5 cm. Clinically, this tumour is characterised by nocturnal pain, a symptom that is alleviated by non-steroidal anti-inflammatory drugs [8]. The initial therapeutic approach for osteoid osteoma involved surgical excision of the nidus. Contemporary standards of care have since shifted toward percutaneous ablation, with RFA emerging as a prominent method [9]. However, unlike RFA, microwave ablation (Fig. 1a, b, c) does not require the use of grounding pads and achieves more extensive tumour volume ablation within a condensed timeframe [10].
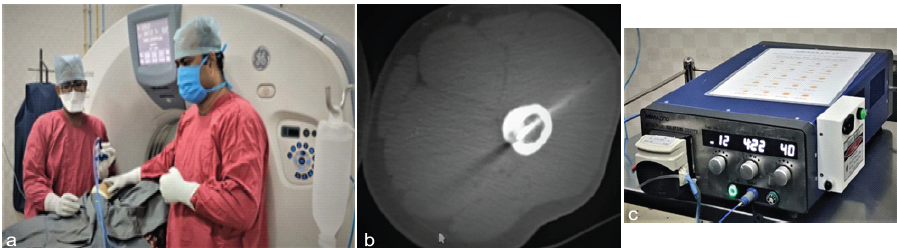
Figure 1: (a) Intraoperative setup for computed tomography (CT)-guided microwave ablation. The patient is positioned within the CT gantry under anesthesia while an interventional radiologist and orthopedic surgeon collaboratively introduce the microwave antenna into the nidus. (b) Intraoperative axial CT image demonstrating the final placement of the microwave antenna, with its tip accurately positioned within the radiolucent nidus before ablation. (c) The microwave ablation generator console. The system allows for precise control of power output and ablation duration, which are tailored to the dimensions of the nidus and its specific anatomical location.
A PubMed search employing the terms “microwave ablation” and “osteoid osteoma” yielded only one previous study [11] with a sample size exceeding 30 patients, thereby underscoring the paucity of robust clinical evidence for this therapeutic modality in the management of osteoid osteoma. Therefore, the aim of this study was to assess the demographics of the patients with osteoid osteoma and to determine the efficacy and safety of microwave ablation in osteoid osteoma through a retrospective analysis of 35 cases encountered at our institution between June 2019 and June 2025. In particular, the study aimed to evaluate the immediate impact of the procedure on pain using the Visual Analogue Scale (VAS), identify any procedural complications, determine the most frequently affected anatomical sites, establish the average patient age, and calculate the average hospital stay.
Study design:
This retrospective analysis included data collected from 35 patients with osteoid osteoma treated using microwave ablation at our institution between June 2019 and June 2025. The sampling technique used was a consecutive sampling technique. The demographic and clinical characteristics of the patients are listed in Table 1.
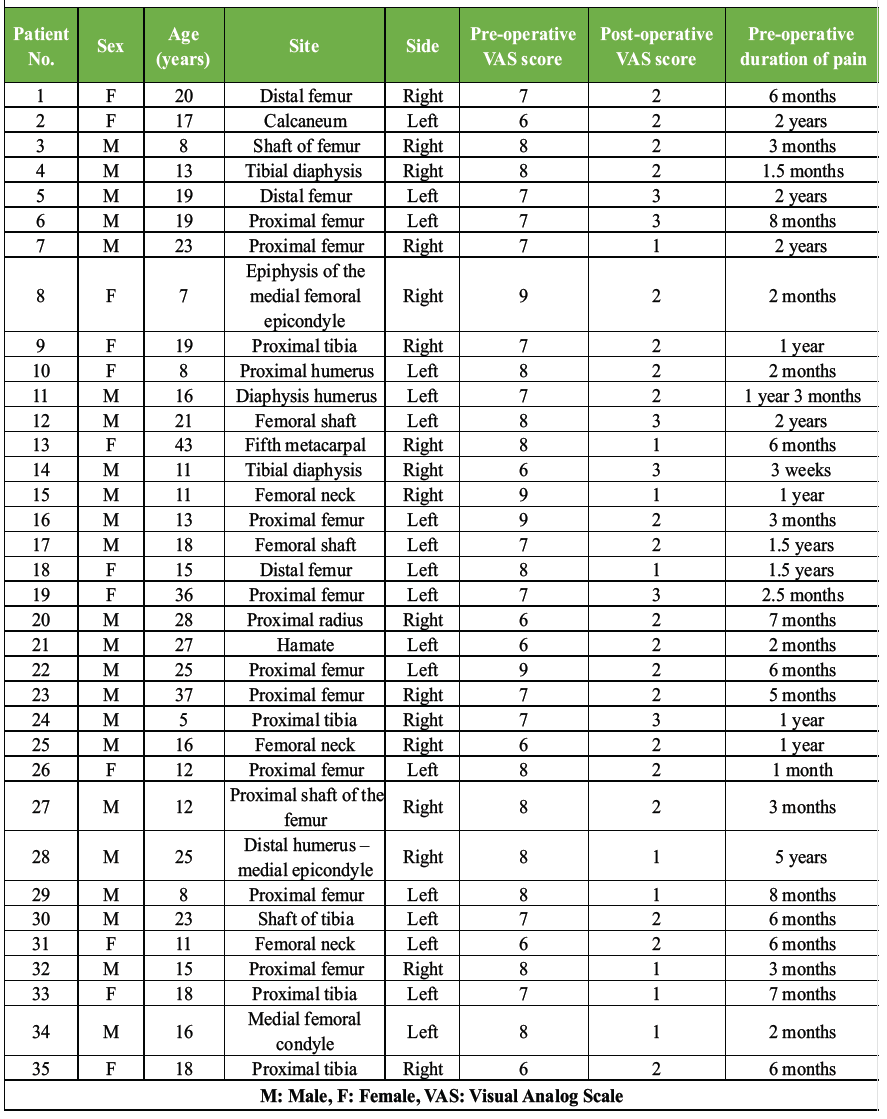
Table 1: Demographic and clinical characteristics of patients undergoing microwave ablation for osteoid osteoma
Patient selection:
Patients with clinically and radiologically diagnosed osteoid osteoma who presented to our institution during the above mentioned period were included in the study.
Data collection:
The patients’ demographic details, anatomical site of the tumour, and VAS scores were recorded. Complications and hospital stay were also documented.
Intervention:
Microwave ablation was performed on all patients using a standard protocol (Fig. 2).
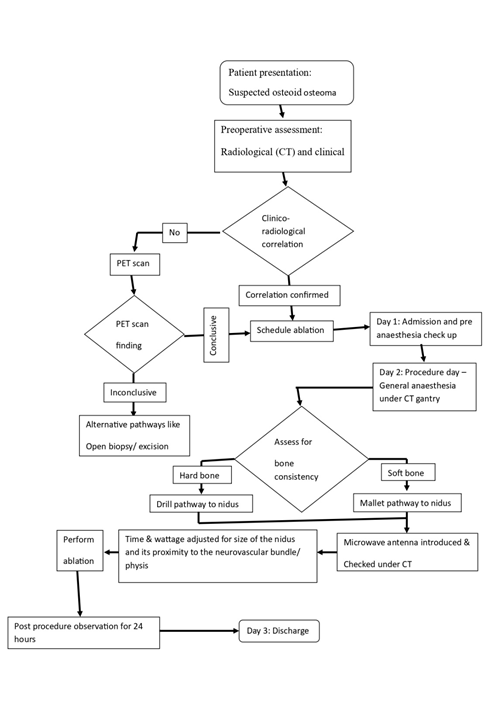
Figure 2: Clinical pathway for microwave ablation of osteoid osteoma in our institute.
The patient was placed supine on the computed tomography (CT) table and administered general anaesthesia. Using CT fluoroscopy and laser guidance, the location of the osteoid osteoma nidus was determined. Thereafter, radiopaque skin markers were placed to assist in trajectory planning, and the corresponding skin entry point was marked. Following sterile preparation and draping, a small skin incision was made at the marked site. Under intermittent CT guidance, a bone access drill was advanced through the cortical bone to gain access to the nidus. A coaxial technique was employed to introduce a microwave ablation antenna directly into the nidus. The ablation parameters, such as power and duration, were selected on the basis of the lesion size and the depth of the antenna tip relative to the centre of the nidus.
Outcome measures:
The primary outcome was the immediate post-procedural change in pain assessed using the VAS. Secondary outcomes, including complications, anatomical distribution, average patient age, and average hospital stay, were documented using a standardised form and analysed using descriptive statistical methods. Of note, because the nidus size for all clinically diagnosed osteoid osteomas in our cohort was uniformly less than 1.5 cm, tumour size was not included as an independent comparative variable.
Data analysis:
Descriptive statistics were employed to analyse the demographic and clinical characteristics. Complications and outcomes were reported as frequencies and percentages.
Ethical considerations:
This study was a retrospective evaluation of existing clinical data. Because the research did not involve prospective interventions, alter established clinical treatment pathways, or introduce new therapeutic strategies, formal Institutional Ethics Committee approval was not required. All procedures performed were part of the routine standard of care. The study adhered to the ethical principles outlined in the Declaration of Helsinki, and all patient data were strictly anonymised to maintain confidentiality.
Patient demographics:
The study included 35 patients with osteoid osteoma, with an average age of 18.08 ± 8.6 years. The proximal femur was the most commonly affected site (9/35 patients [27%]).
Assessment:
An analysis of the VAS scores revealed a marked alleviation of pain immediately after microwave ablation in the majority of patients (34/35 [97.1%]). The average pre-procedural pain score of 7.4 ± 0.94 decreased to an average score of 1.9 ± 0.7 within 1 week after the procedure. Notably, only one patient reported enduring pain beyond the immediate post-procedural period.
Complications:
Complications were noted in five patients and included delayed wound healing, fracture, and nerve palsy.
Hospital stay:
The average hospital stay for all patients was 3 days.
While RFA (introduced in the 1990s) has traditionally been regarded as the gold standard for osteoid osteoma treatment, microwave ablation has recently gained prominence as the treatment of choice [12]. The introduction of microwave ablation in India, notably at Tata Memorial Hospital in 2015, marked a significant shift in the therapeutic landscape [12,13]. A study conducted by Reis et al. demonstrated that microwave ablation achieved a technical success rate of 100%, surpassing the 83% success rate observed with RFA. In RFA, the impedance challenges posed by charred tissue hinder energy propagation. However, microwave ablation, which operates on the principle of water molecule agitation, results in reduced tissue charring and a diminished heat sink effect that enhances the efficacy of tumour ablation [14]. These findings underscore the evolving role of microwave ablation as a potentially superior alternative to RFA in the management of osteoid osteoma. Many studies have consistently documented the efficacy of osteoid osteoma management using microwave ablation, with success rates ranging from 92.3% to 100% [14,15,16]. Because the primary therapeutic objective is the targeted necrosis of the nidus rather than volumetric tumour reduction, clinical success is primarily dictated by symptom resolution. Our study demonstrated an efficacy of 97.1% for microwave ablation. Persistent post-procedural pain was observed in only one patient. Notably, this patient presented a unique case of osteoid osteoma recurrence despite undergoing prior microwave ablation at a different centre. A follow-up positron emission tomographic scan conducted 1 month after the current treatment indicated no activity at the nidus. Subsequently, the patient’s pain alleviated spontaneously. Our literature review also highlighted a significant gap in understanding the efficacy of microwave ablation in recurrent osteoid osteoma, thereby emphasising the need for further investigation to address this potential limitation. According to a systematic review conducted by Cazzato et al., the incidence of complications in percutaneous microwave ablation for bone tumours was approximately 4% [16]. In one of the most extensive case series studies on microwave ablation for osteoid osteoma by Rinzler et al., the observed complication rate was 17% [15]. In our study, the overall complication rate was 14.3%, including cases of delayed wound healing. Notably, the risk of thermal injury to surrounding tissues remains a clinical concern, primarily due to the fixed length of the microwave antenna’s active heating element. Specifically, the availability of only a 1.5-cm heating tip posed challenges, particularly when applied to regions such as the forearm or smaller bones. To enhance the safety and precision of the procedure, microwave antennas featuring variable lengths for the heating tip need to be developed, as these could offer a more tailored and secure approach to such anatomical sites.
- Microwave ablation can be used for precisely ablating the tumor nidus, resulting in a notable decrease in pain and the prevention of recurrence
- However, precautions must be taken to prevent thermal injuries to the surrounding tissues caused by the microwave antenna’s heating component
- Our study highlights the efficacy and safety of microwave ablation for osteoid osteoma while also emphasising its clinical relevance.
Microwave ablation is a highly efficacious alternative to traditional RFA for osteoid osteomas, achieving near-universal immediate pain reduction. However, because current microwave antennas utilise a fixed 1.5-cm heating element, clinicians must exercise extreme caution and employ rigorous pre-operative trajectory planning when treating lesions in compact anatomical regions to avoid thermal injury.
References
- 1. Halsted WS. I. The results of operations for the cure of cancer of the breast performed at the Johns Hopkins Hospital from June, 1889, to January, 1894. Ann Surg 1894;20:497-555. [Google Scholar] [PubMed]
- 2. Simon CJ, Dupuy DE, Mayo-Smith WW. Microwave ablation: Principles and applications. Radiographics 2005;25 Suppl 1:S69-83. [Google Scholar] [PubMed]
- 3. Shibata T, Iimuro Y, Yamamoto Y, Maetani Y, Ametani F, Itoh K, et al. Small hepatocellular carcinoma: Comparison of radio-frequency ablation and percutaneous microwave coagulation therapy. Radiology 2002;223:331-7. [Google Scholar] [PubMed]
- 4. Osepchuk JM. The history of the microwave oven: A critical review. In: 2009 IEEE MTT-S International Microwave Symposium Digest. Boston, MA, USA: IEEE; 2009. p. 1397-400. Available from: https://ieeexplore.ieee.org/document/5165967 [Last accessed on 2026 April 3]Ryan TP, Turner PF, Hamilton B. Interstitial microwave transition from hyperthermia to ablation: Historical perspectives and current trends in thermal therapy. Int J Hyperthermia 2010;26:415-33. [Google Scholar] [PubMed]
- 5. Zhang Y, Rosenberg AE. Bone-forming tumors. Surg Pathol Clin 2017;10:513-35. [Google Scholar] [PubMed]
- 6. Lee EH, Shafi M, Hui JH. Osteoid osteoma: A current review. J Pediatr Orthop 2006;26:695-700. [Google Scholar] [PubMed]
- 7. Boscainos PJ, Cousins GR, Kulshreshtha R, Oliver TB, Papagelopoulos PJ. Osteoid osteoma. Orthopedics 2013;36:792-800. [Google Scholar] [PubMed]
- 8. Miyazaki M, Arai Y, Myoui A, Gobara H, Sone M, Rosenthal DI, et al. Phase I/II multi-institutional study of percutaneous radiofrequency ablation for painful osteoid osteoma (JIVROSG-0704). Cardiovasc Intervent Radiol 2016;39:1464-70. [Google Scholar] [PubMed]
- 9. Skinner MG, Iizuka MN, Kolios MC, Sherar MD. A theoretical comparison of energy sources–microwave, ultrasound and laser–for interstitial thermal therapy. Phys Med Biol 1998;43:3535-47. [Google Scholar] [PubMed]
- 10. Mutlu IN, Cingoz M, Guzelbey T, Cingoz E, Kilickesmez O. Percutaneous CT-guided microwave ablation for the treatment of osteoid osteomas: A single center experience. Acad Radiol 2024;31:3725-31. [Google Scholar] [PubMed]
- 11. Tepelenis K, Skandalakis GP, Papathanakos G, Kefala MA, Kitsouli A, Barbouti A, et al. Osteoid osteoma: An updated review of epidemiology, pathogenesis, clinical presentation, radiological features, and treatment option. In Vivo 2021;35:1929-38. [Google Scholar] [PubMed]
- 12. Gala KB, Shetty NS, Patel P, Kulkarni SS. Microwave ablation: How we do it? Indian J Radiol Imaging 2020;30:206-13. [Google Scholar] [PubMed]
- 13. Reis J, Chang Y, Sharma AK. Radiofrequency ablation vs microwave ablation for osteoid osteomas: Long-term results. Skeletal Radiol 2020;49:1995-2000. [Google Scholar] [PubMed]
- 14. Rinzler ES, Shivaram GM, Shaw DW, Monroe EJ, Koo KS. Microwave ablation of osteoid osteoma: Initial experience and efficacy. Pediatr Radiol 2019;49:566-70. [Google Scholar] [PubMed]
- 15. Cazzato RL, De Rubeis G, De Marini P, Dalili D, Koch G, Auloge P, et al. Percutaneous microwave ablation of bone tumors: A systematic review. Eur Radiol 2021;31:3530-41. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2025 Patellar Osteoid Osteoma: A Rare Cause for Anterior Knee Pain
May 1, 2025 Patellar Osteoid Osteoma: A Rare Cause for Anterior Knee Pain October 10, 2022 Intra-articular osteoid osteoma of the hip mimicking as monoarthritis-A case report
October 10, 2022 Intra-articular osteoid osteoma of the hip mimicking as monoarthritis-A case report May 10, 2021 Femur Neck Osteoid Osteoma Managed with Radiofrequency Ablation – A Case Report
May 10, 2021 Femur Neck Osteoid Osteoma Managed with Radiofrequency Ablation – A Case Report August 1, 2026 O-arm Navigation-assisted Excision of Cervical Osteoid Osteoma Adjacent to the Vertebral Artery: Technical Note and Case Report
August 1, 2026 O-arm Navigation-assisted Excision of Cervical Osteoid Osteoma Adjacent to the Vertebral Artery: Technical Note and Case Report