
Standardised preparation of leukocyte-poor platelet-rich plasma and its targeted multi-site delivery during arthroscopic anterior cruciate ligament reconstruction may enhance early graft healing and functional recovery. The biological effect of platelet-rich plasma depends more on its preparation and delivery technique than on its mere use.
Dr. Avik Kumar Naskar, Department of Orthopaedics, Indira Gandhi Government Medical College and Hospital, Nagpur, Maharashtra, India. E-mail: avik7933@gmail.com
Abstract
Introduction: The role of platelet-rich plasma (PRP) in anterior cruciate ligament (ACL) reconstruction remains controversial due to heterogeneity in preparation and application protocols. This technical note describes a standardised method for preparation of leukocyte-poor (LP) PRP and its multi-site intraoperative application, along with favourable early functional outcomes in 15 cases.
Materials and Methods: LP-PRP was prepared using a double-spin centrifugation technique with deliberate exclusion of the buffy coat to minimise leukocyte content. Approximately 30 mL of autologous blood was processed. PRP was applied at three sites – (1) graft soaking before insertion, (2) injection into femoral and tibial tunnels, and (3) intra-articular injection after graft fixation.
Results: Fifteen patients undergoing arthroscopic ACL reconstruction with hamstring autograft and LP PRP augmentation were evaluated. Early follow-up demonstrated rapid improvement in functional outcomes, with higher Lysholm, International Knee Documentation Committee, and Tegner scores within the initial post-operative period compared to expected recovery timelines. No PRP-related complications were observed.
Conclusion: A reproducible protocol for LP-PRP preparation and multi-site delivery may contribute to enhanced early recovery following ACL reconstruction. Standardisation of this technique may improve consistency of outcomes.
Keywords: Anterior cruciate ligament reconstruction, platelet-rich plasma, arthroscopy, ligament healing, knee injuries.
Anterior cruciate ligament (ACL) reconstruction is widely performed to restore knee stability and function following ligament injury. Despite advances in surgical technique, graft incorporation and ligamentization remain biologically time-dependent processes that can delay functional recovery. Although platelet-rich plasma (PRP) shows promise and is used in various fields, including plastic surgery, dermatology, and the treatment of osteoarthritis (OA), it is not widely used in or alongside the treatment of ACL injuries. PRP has been investigated as a biological adjunct to enhance graft healing through the delivery of concentrated growth factors. However, clinical outcomes remain inconsistent, largely due to variability in preparation methods, leukocyte content, and delivery techniques [1,2]. A meta-analysis by McRobb et al. highlights a significant early increase in the rate of ligamentization and vascularisation when PRP is used following ACL reconstruction, though no significant improvement was found in the later stages of the healing process, with varying post-operative pain and functional outcomes reported [3]. Advantages of PRP augmentation include accelerated graft healing, reduced early post-operative pain and inflammation, improved graft-bone integration, lesser risk of immune reaction and infection due to its autologous nature [4]. Leukocyte-poor (LP)-PRP is believed to provide a more favorable intra-articular environment by minimizing inflammatory cytokines while preserving anabolic effects [5]. Heterogeneity in PRP preparation and delivery remains a major limitation in existing literature. To the best of our knowledge, this is the only report describing a standardized LP-PRP preparation protocol combined with its systematic multi-site intraoperative delivery during arthroscopic ACL reconstruction.
The study was conducted at the Department of Orthopaedics in a tertiary care facility.
Study population:
A total of 15 male and female patients undergoing arthroscopic ACL reconstruction between June 2023 and February 2024 were considered eligible and were included in the study.
Study design:
This is a prospective observational study conducted in the Department of Orthopaedics to study the preparation technique and multi-site application of LP-PRP in detail and evaluate the functional outcome in LP-PRP-augmented ACL reconstruction.
Data source:
The study investigated patients who were operated between June 2023 and February 2024. The Ethics Committee of the Institute approved the study. (Ethics code: IGGMC/Pharm/BORS/2294-95/2024).
Patient preference:
A convenience sample of 15 patients was included in the study. All patients above the age of 18 years who had isolated complete ACL rupture confirmed by magnetic resonance imaging (MRI) (three Tesla magnet strength), with no known allergy to PRP components, undergoing arthroscopic ACL reconstruction between 2023 and 2024 and were willing to participate and provide informed consent were taken into account (Fig. 1). Patients with active infection, partial tears, chronic ACL insufficiency, multi-ligament knee injuries, a history of autoimmune diseases or inflammatory arthritis, bleeding diathesis and those on anticoagulant therapy and systemic illnesses have been excluded from the research.
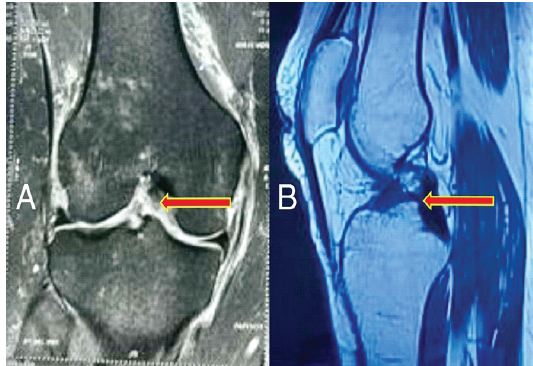
Figure 1: Pre-operative magnetic resonance imaging; (a) coronal and (b) sagittal magnetic resonance images showing disruption of the anterior cruciate ligament (arrows). There is a visible discontinuity and abnormal signal intensity of the anterior cruciate ligament consistent with tear.
Data collection:
Before surgery, a detailed medical history of all the patients was noted, and physical examination of the knee and the lower extremity was done. MRI was done to confirm the diagnosis and rule out associated conditions. Postoperatively, baseline functional outcome measures, including the International Knee Documentation Committee (IKDC) and Lysholm scores, Tegner activity scale and Visual Analogue Scale (VAS), were recorded, and knee range of motion (ROM) was measured with a goniometer.
Technique:
All the patients were operated on under spinal anaesthesia with a tourniquet pressure of 350 mmHg and using the inside-out technique (Fig. 2). Arthroscopic ACL reconstruction using an autogenous quadrupled hamstring graft was done (Fig. 3). An endobutton was used at the femoral tunnel, and a bio-screw of diameter one millimetre more than the graft thickness was used at the tibial tunnel. Freshly prepared PRP from the patient’s own venous blood was used to soak the graft before insertion and injected in both the tibial and femoral tunnels using a spinal needle under arthroscopic vision at the end of the surgery.
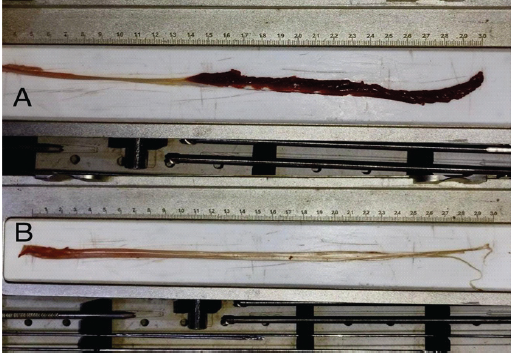
Figure 2: Harvesting and preparation of semitendinosus graft; (a) stripped semitendinosus muscle with attached tendon following harvest. (b) Residual muscle fibers meticulously removed from the tendon using a blade with a tilted head to obtain a clean graft suitable for reconstruction.
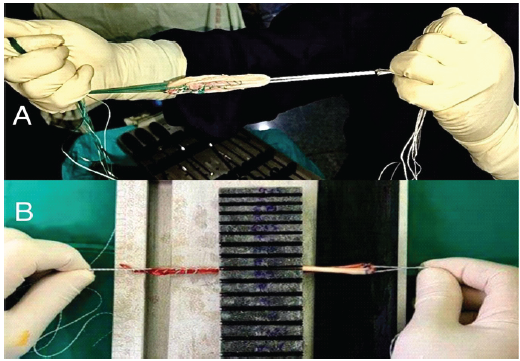
Figure 3: Intraoperative images demonstrating graft preparation for arthroscopic anterior cruciate ligament reconstruction; (a) four-stranded hamstring autograft following ‘whip-stitching’ of the free ends. (b) Measurement of graft diameter using a sizing block before insertion.
Preparation of LP-PRP:
Approximately 30 mL of autologous venous blood was collected from the patients in citrate-containing glass tubes. A standardised double-spin centrifugation protocol was employed, consistent with established PRP preparation techniques [6]. A first spin (soft spin) was carried out at the rate of 2000 rpm for 15 min, then the upper plasma was carefully aspirated under sterile conditions with strict avoidance of the lowermost red blood cells and the buffy coat to ensure leukocyte depletion. A second spin (hard spin) was conducted at 3500 rpm for another 10 min. A temperature of 20°C was consistently maintained during the centrifugation for optimal platelet activation [7]. Platelet-poor plasma at the top was discarded, and the platelet pellet was resuspended to obtain LP-PRP (Fig. 4). This technique yielded a high platelet concentration with minimal leukocyte contamination. Calcium chloride was finally added to this solution in order for the platelets to release growth factors, initiating a cascade that promotes cellular chemotaxis and matrix deposition [8].
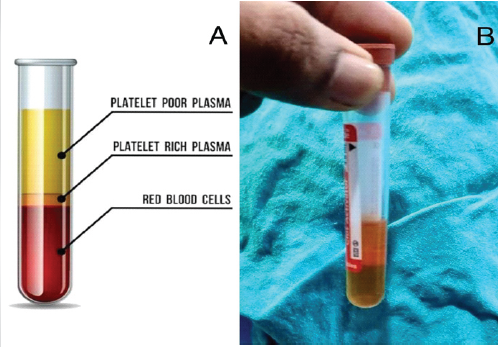
Figure 4: Representative illustration and clinical photograph demonstrating separation of platelet-rich plasma following centrifugation; (a) schematic depiction of the three distinct layers: Platelet-poor plasma (upper layer), platelet-rich plasma (middle layer), and red blood cells (bottom layer). (b) Actual centrifuged sample with visible stratification, highlighting the PRP layer used for therapeutic application.
Application of LP-PRP:
LP-PRP was applied using a standardised multi-site protocol, based on principles of targeted biological augmentation [9]:
- Graft soaking: The hamstring graft was soaked in freshly prepared LP-PRP for 10 min prior to its insertion to facilitate growth factor absorption.
- Tunnel injection: LP-PRP was injected into the femoral socket and tibial tunnel around the graft after fixation, targeting the bone-tendon interface to enhance healing.
- Intra-articular injection: Residual PRP was injected around the intra-articular segment of the graft at the conclusion of the procedure to promote synovial and intra-articular healing.
This approach ensured comprehensive exposure of the graft and surrounding tissues to biological augmentation (Fig. 5).
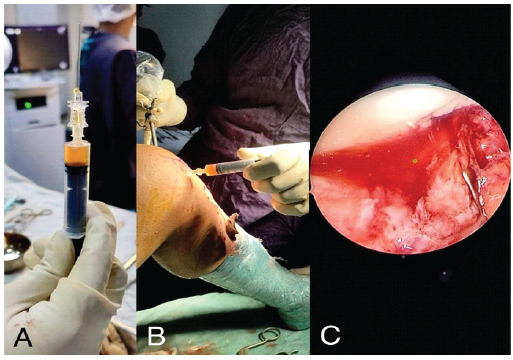
Figure 5: Leukocyte-poor platelet-rich plasma preparation and administration during anterior cruciate ligament reconstruction; (a) Prepared leukocyte-poor platelet-rich plasma (LP-PRP) in syringe following double-centrifugation. (b) Peri-articular injection of LP-PRP around the graft at the operative site. (c) Arthroscopic view demonstrating intra-articular LP-PRP delivery into the femoral and tibial tunnels and around the graft to enhance biological healing.
Rehabilitation:
During the initial period (0–6 weeks), focus was on pain management, early mobilisation and gentle ROM exercises with weight-bearing per tolerance of the patient. Over the next 6–12 weeks, strengthening of quadriceps, hamstrings, and calf muscles was encouraged through open and closed kinetic chain movements. Proprioceptive training and functional exercises were done to enhance balance, coordination and neuromuscular control. After 12 weeks, sport-specific exercises and drills were encouraged for a safe return to pre-injury activity levels.
Follow-up protocol:
IKDC, Lysholm, and Tegner scores for primary functional outcome were assessed at 4 and 8 weeks and 6 months postoperatively. Secondary outcomes like graft incorporation and healing were evaluated by clinical examination and VAS scoring to understand the long-term efficacy and safety of LP-PRP augmentation.
Statistical analysis:
Descriptive statistical analysis was performed. Continuous variables were expressed as mean ± standard deviation. Changes in functional scores over time were assessed; however, no comparative statistical inference was intended due to the observational nature of the study.
A total of 15 patients, which included eight females and seven males, were included in the study. The mean age of the study population was 29.26 ± 8.25 years, and the time taken to return to pre-injury activities was 5.33 ± 0.83 months. While the mean IKDC score increased from 53.86 ± 0.63 in the immediate post-operative period to 66.73 ± 1.48 at 6 months after surgery, the mean Lysholm score increased from 62.06 ± 1.33 to 83.67 ± 1.83, the mean Tegner activity scores increased from 3.40 ± 0.5 to 4.73 ± 0.7, and the mean VAS score also increased from 5.26 ± 0.7 to 1.60 ± 0.63 during the same period (Table 1).
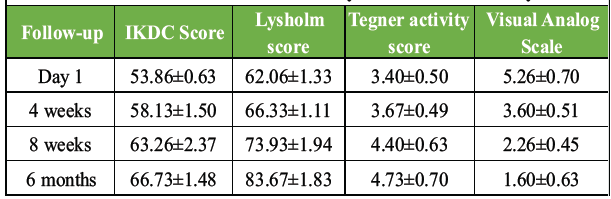
Table 1: Functional outcome scores at different stages of follow-up; Postoperatively the IKDC, Lysholm, Tegner activity and, Visual Analog Scale scores all showed steady improvement with time. All the patients were satisfied with their recovery and functional ability
The mean time taken to achieve 90° knee flexion and full knee extension was 23.27 ± 1.09 and 41.86 ± 1.5 days, respectively (Table 2).
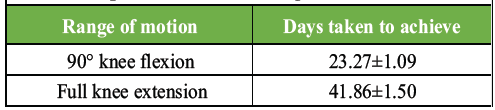
Table 2: Knee range of motion achieved versus days taken from surgery; satisfactory knee movements were seen early into the recovery period highlighting the combined importance of preparation, delivery and clinical effectiveness of leukocyte-poor platelet-rich plasma in arthroscopic anterior cruciate ligament reconstruction
These findings are consistent with previous reports suggesting improved early recovery with biological augmentation [4,10]. No complications such as infection, excessive inflammation, or adverse reactions attributable to PRP were observed (Fig. 6 and 7).

Figure 6: Clinical photos of the suture site and range of motion of the operated knee; Suture site in the (a) immediate post-operative period and (b) at 6 months follow-up. No wound-related complications were observed. Normal knee range of motion showing full (c) extension and (d) flexion at 6 months after surgery.

Figure 7: Post-operative X-rays of the knee at 6 months; (a) anteroposterior and (b) lateral X-rays of the knee at 6 months follow-up showing an interference screw within the proximal tibial tunnel and an endobutton on the femoral cortex. Joint space is well-maintained, and there is no evidence of any hardware-related complication.
The clinical efficacy of PRP in ACL reconstruction remains debated, with systematic reviews reporting mixed outcomes [2]. A major limitation in existing studies is the lack of standardisation in PRP preparation and application protocols. The present technique emphasises two key factors – first, leukocyte modulation. LP-PRP reduces leukocyte-associated inflammatory cytokines, which may otherwise contribute to synovial irritation and delayed recovery in intra-articular applications [11]. Second, multi-site delivery. Unlike single-site applications used in many studies, targeted delivery at the graft surface, graft–bone interface, and intra-articular space may enhance biological effectiveness by maximising tissue exposure [12]. The early functional improvement observed in this cohort supports the hypothesis that PRP may primarily influence early phases of graft healing, including angiogenesis and cellular proliferation [3]. Ji et al. in their study also observed significant improvement in the IKDC score after 3 months from surgery, which shows that PRP had an effect on long-term improvement of knee health [13]. Chen et al. observed significant improvement in IKDC scores during the first 3 months after surgery, but not so much after 6 and 12 months [14]. On the contrary, Sözkesen et al. in their comparative study found no significant difference in the mean score with the use of PRP [15]. Kumar et al. found significantly better mean Lysholm scores at 6 and 12 weeks after surgery in patients augmented with PRP [16]. Higher mean Tegner scores were observed in the current study at 8 weeks after surgery, which were contrary to the findings of Sözkesen et al. and Gong et al. [15,17]. Yin et al. in their study on rabbit knee OA concluded that leukocytes in the PRP may deliver increased levels of pro-inflammatory cytokines like the nuclear factor kappa B signalling pathway, reducing the beneficial effects of growth factors on arthritic cartilages [18]. Pham, in his 2025 study, reiterated that LR-PRP contains higher levels of white blood cells and proinflammatory cytokines, while LP-PRP has minimal leukocyte content and promotes anti-inflammatory and anabolic responses [19]. Valentí Azcárate et al. in their comparative study of 150 knees have shown that swelling and inflammatory parameters significantly improved within 24 h of arthroscopic ACL reconstruction in patients augmented with LP-PRP [20]. They used a single-spin centrifugation technique, which is in contrast to the current study, where double centrifugation was performed. The findings of this study suggest that the variability in outcomes reported with LP-PRP may be attributable not only to its biological properties but also to differences in preparation and delivery techniques. By adopting a standardised protocol for the preparation of LP-PRP and ensuring its targeted multi-site application, consistent biological augmentation can be achieved at critical zones of graft healing. The encouraging early functional recovery observed in this series supports the premise that meticulous technique may enhance the clinical effectiveness of LP-PRP.
Advantages of the study:
Unlike most studies that focus primarily on the efficacy of PRP, the current study highlights a standardised preparation protocol of LP-PRP, its targeted multi-site delivery in arthroscopic ACL reconstruction, and the early favourable functional outcomes of the patients.
Limitations of the study:
Limitations include small sample size, absence of a control group, and lack of long-term follow-up. However, the objective of this report is to describe a reproducible and clinically standardised technique providing a practical framework for future clinical application and research rather than establish definitive efficacy.
A standardised protocol for preparation of LP-PRP and its targeted multi-site application during arthroscopic ACL reconstruction is safe, reproducible, and clinically feasible. This approach ensures optimal biological delivery at critical healing interfaces and is associated with encouraging early functional recovery. These findings emphasise that the technique of LP-PRP preparation and application may play a pivotal role in influencing clinical outcomes with biological augmentation.
Standardisation of PRP preparation and targeted delivery is essential for optimising outcomes in ACL reconstruction. Multi-site application of LP-PRP may enhance early functional recovery and represents a practical adjunct to routine surgical practice.
References
- 1. Figueroa D, Figueroa F, Calvo R, Vaisman A, Ahumada X, Arellano S. Platelet-rich plasma use in anterior cruciate ligament surgery: Systematic review of the literature. Arthroscopy 2015;31:981-8. [Google Scholar] [PubMed]
- 2. Andriolo L, Di Matteo B, Kon E, Filardo G, Venieri G, Marcacci M. PRP augmentation for ACL reconstruction. Biomed Res Int 2015;2015:371746. [Google Scholar] [PubMed]
- 3. McRobb CM, Kamil KH, Ahmed I, Dhaif F, Metcalfe A. Influence of platelet-rich plasma (PRP) analogues on healing and clinical outcomes following anterior cruciate ligament (ACL) reconstructive surgery: A systematic review. Eur J Orthop Surg Traumatol 2023;33:225-53. [Google Scholar] [PubMed]
- 4. Zhu Y, Yuan M, Meng HY, Wang AY, Guo QY, Wang Y, et al. Basic science and clinical application of platelet-rich plasma for cartilage defects and osteoarthritis: A review. Osteoarthritis Cartilage 2013;21:1627-37. [Google Scholar] [PubMed]
- 5. Lana JF, Huber SC, Purita J, Tambeli CH, Santos GS, Paulus C, et al. Leukocyte-rich PRP versus leukocyte-poor PRP – The role of monocyte/macrophage function in the healing cascade. J Clin Orthop Trauma 2019;10 Suppl 1:S7-12. [Google Scholar] [PubMed]
- 6. Radice F, Yáñez R, Gutiérrez V, Rosales J, Pinedo M, Coda S. Comparison of magnetic resonance imaging findings in anterior cruciate ligament grafts with and without autologous platelet-derived growth factors. Arthroscopy 2010;26:50-7. [Google Scholar] [PubMed]
- 7. Maurer-Spurej E, Pfeiler G, Maurer N, Lindner H, Glatter O, Devine DV. Room temperature activates human blood platelets. Lab Invest 2001;81:581-92. [Google Scholar] [PubMed]
- 8. Marx RE. Platelet-rich plasma: Evidence to support its use. J Oral Maxillofac Surg 2004;62:489-96. [Google Scholar] [PubMed]
- 9. Vogrin M, Rupreht M, Dinevski D, Hašpl M, Kuhta M, Jevsek M, et al. Effects of a platelet gel on early graft revascularization after anterior cruciate ligament reconstruction: A prospective, randomized, double-blind, clinical trial. Eur Surg Res 2010;45:77-85. [Google Scholar] [PubMed]
- 10. Cavanaugh JT, Powers M. ACL rehabilitation progression: Where are we now? Curr Rev Musculoskelet Med 2017;10:289-96. [Google Scholar] [PubMed]
- 11. Zhang Y, Xiao Z, Fan Z, Zhang Y, Xu J, Wang K. The impact of platelet-rich plasma injection on anterior cruciate ligament reconstruction: A systematic review and meta-analysis. Front Bioeng Biotechnol 2025;13:1625271. [Google Scholar] [PubMed]
- 12. Riboh JC, Saltzman BM, Yanke AB, Fortier L, Cole BJ. Effect of leukocyte concentration on the efficacy of platelet-rich plasma in the treatment of knee osteoarthritis. Am J Sports Med 2016;44:792-800. [Google Scholar] [PubMed]
- 13. Ji Q, Yang Y, Chen H, Geng W, Dong H, Yu Q. Clinical evaluations of anterior cruciate ligament reconstruction with platelet rich plasma. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2017;31:410-6. [Google Scholar] [PubMed]
- 14. Chen J, Wan Y, Lin Y, Jiang H. The application of platelet-rich plasma for skin graft enrichment: a meta-analysis. International Wound Journal. 2020;17(6):1650-1658. doi:10.1111/iwj.13445. PMID: 32633467. PMCID:PMC7948779. [Google Scholar] [PubMed] [CrossRef]
- 15. Sözkesen S, Karahan HG, Kurtulmus A, Kayali C, Altay T. PRP on preventıon of tunnel enlargement in ACL reconstructıon. Ortop Traumatol Rehabil 2018;20:285-91. [Google Scholar] [PubMed]
- 16. Kumar A, Kushwaha NS, Kumar D, Singh A, Gupta V, Kumar S. Prospective comparison of functional and radiological outcomes of arthroscopic anterior cruciate ligament reconstruction by hamstring graft alone and platelet-rich plasma added to the hamstring graft. Cureus 2022;14:e23017. [Google Scholar] [PubMed]
- 17. Gong H, Huang B, Zheng Z, Fu L, Chen L. Clinical use of platelet-rich plasma to promote tendon-bone healing and graft maturation in anterior cruciate ligament reconstruction-a randomized controlled study. Indian J Orthop 2022;56:805-11. [Google Scholar] [PubMed]
- 18. Yin WJ, Xu HT, Sheng JG, An ZQ, Guo SC, Xie XT, et al. Advantages of pure platelet-rich plasma compared with leukocyte- and platelet-rich plasma in treating rabbit knee osteoarthritis. Med Sci Monit 2016;22:1280-90. [Google Scholar] [PubMed]
- 19. Pham GM. Biologic augmentation in anterior cruciate ligament reconstruction and beyond: A review of PRP and BMAC. J Clin Med 2025;14:6959. [Google Scholar] [PubMed]
- 20. Valentí Azcárate A, Lamo-Espinosa J, Aquerreta Beola JD, Hernandez Gonzalez M, Mora Gasque G, Valentí Nin JR. Comparison between two different platelet-rich plasma preparations and control applied during anterior cruciate ligament reconstruction. Is there any evidence to support their use? Injury 2014;45 Suppl 4:S36-41. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2025 A Comparative Study to Assess Functional Outcomes and Proprioception in Remnant-Preserving versus Standard Anterior Cruciate Ligament Reconstruction
April 1, 2025 A Comparative Study to Assess Functional Outcomes and Proprioception in Remnant-Preserving versus Standard Anterior Cruciate Ligament Reconstruction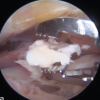 August 1, 2026 Isolated Calcific Deposition in the Subacromial Bursa: A Rare Case Report and Arthroscopic Management
August 1, 2026 Isolated Calcific Deposition in the Subacromial Bursa: A Rare Case Report and Arthroscopic Management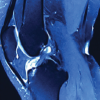 August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain
August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain August 1, 2026 Platelet-Rich Plasma Augmentation of Osteosynthesis in Femoral Neck Fractures: A Prospective Comparative Study Demonstrating Accelerated Union and Improved Function
August 1, 2026 Platelet-Rich Plasma Augmentation of Osteosynthesis in Femoral Neck Fractures: A Prospective Comparative Study Demonstrating Accelerated Union and Improved Function