
The learning point of the article is that early pain relief achieved with ultrasound-guided hydrodistension enhances physiotherapy compliance and results in superior short-term functional outcomes compared to manipulation under anaesthesia in patients with adhesive capsulitis.
Dr. Tanishque Sanjay Oberai, Department of Orthopaedics, Mahatma Gandhi Mission, Medical College and Hospital, Gate No. 2, MGM Campus, N-6, CIDCO, Aurangabad - 431-003, Maharashtra, India. E-mail: tanishque1998@gmail.com
Abstract
Introduction: Adhesive capsulitis (frozen shoulder) is a disabling condition characterized by pain and restricted range of motion (ROM). Among various treatment options, manipulation under general anesthesia (MUGA) and ultrasound-guided hydrodistension (USG-HD) with corticosteroid injection are commonly used. This study compares their short-term efficacy and safety.
Materials and Methods: This prospective, comparative, interventional study included 50 patients aged 30–75 years with primary adhesive capsulitis unresponsive to conservative management. Patients were allocated into two groups using alternate assignment (non-randomised). Group A underwent manipulation under anaesthesia (MUA) followed by intra-articular steroid injection, while Group B received USG-HD with steroid injection. Outcomes were assessed using the shoulder pain and disability index (SPADI), pain score, disability scale, and ROM at baseline, post-procedure, and at 1-month follow-up. Statistical analysis was performed with P < 0.05 considered significant.
Results: Both groups showed significant improvement in pain and functional outcomes. However, Group B demonstrated greater reduction in SPADI, pain, and disability scores at 1-month follow-up compared to Group A, with statistically significant differences (P < 0.05). No major complications were noted, and USG-HD was better tolerated.
Discussion: USG-HD provided superior short-term outcomes compared to MUA, likely due to its minimally invasive nature and targeted capsular distension. However, the short follow-up limits assessment of long-term benefits and recurrence.
Conclusion: USG-HD is more effective than MUA for short-term improvement in adhesive capsulitis, but longer follow-up is needed before establishing definitive treatment preference.
Keywords: Adhesive capsulitis, hydrodistension, manipulation under anesthesia.
Adhesive capsulitis, or frozen shoulder (FS), is a condition involving inflammation and fibrosis of the shoulder joint capsule, causing persistent pain and progressive stiffness, often over 2–3 years. It typically affects people over 40, with females being more at risk than males, and it commonly involves the non-dominant shoulder [1]. The condition is associated with diabetes, thyroid disorders, and shoulder immobility.
FS progresses through three stages:
- Freezing stage: Increasing pain and stiffness, particularly at night, lasting 6 weeks to 9 months
- Frozen stage: Pain lessens, but stiffness persists, lasting 2–6 months
- Thawing stage: Gradual recovery of motion and strength over 6 months to 2 years.
Management aims to relieve pain, restore motion, and improve function. Treatments include physical therapy, steroid injections, hydro distention, and, in severe cases, surgical options like manipulation under anaesthesia (MUA). Despite many available interventions, the best approach remains debated. Early diagnosis and timely treatment are critical to minimising the condition’s impact on quality of life.
Types of FS:
- Primary FS (idiopathic adhesive capsulitis)
-
- Definition: Occurs without an identifiable cause.
- Characteristics: gradual onset, classic three-stage progression (freezing, frozen, thawing).
- Risk Factors: Affects individuals aged 40–60, more common in women, and linked to diabetes [2].
- Secondary FS
-
- Definition: Develops due to an underlying condition or injury.
- Types:
-
-
- Post-traumatic: caused by shoulder trauma (e.g., fractures, dislocations, surgeries) with immobilisation.
- Post-surgical: Arises after shoulder surgeries, such as rotator cuff repairs.
- Systemic diseases: Linked to diabetes (alters collagen metabolism), thyroid disorders, and autoimmune conditions (e.g., rheumatoid arthritis, lupus).
-
- Diabetic FS
-
- Definition: A secondary type specifically linked to diabetes.
- Characteristics: More resistant to treatment and may last longer.
- Management: Requires blood glucose control alongside conventional treatments.
- Shoulder impingement syndrome leading to FS
-
- Definition: Progresses from untreated shoulder impingement syndrome.
- Characteristics: Pain during overhead activities, inflammation, and eventual stiffness.
- Post-stroke FS
-
- Definition: Occurs after stroke or central nervous system injury
- Characteristics: Immobilization and reduced arm use lead to stiffness
- Management: Combines neurological and orthopaedic rehabilitation approaches.
Aims:
This study aims to compare the efficacy and safety of two treatments for primary adhesive capsulitis (FS):
- Manipulation under general anesthesia (MUGA) with steroid injection
- Ultrasound-guided hydrodistension (USG-HD) with steroid injection.
The focus is on pain relief, range of motion (ROM) improvement, safety, patient satisfaction, and long-term effectiveness.
Objectives
Primary objectives:
-
- Compare pain relief using the shoulder pain and disability index (SPADI) scale before and after treatment
- Assess ROM improvements using goniometric measurements pre- and post-treatment.
Secondary objectives:
-
- Evaluate safety and monitor for complications (e.g., infection, bleeding, nerve injury)
- Assess patient satisfaction, functional outcomes, and return to daily activities
- Compare long-term outcomes, including recurrence rates and sustained improvement over 1 month.
Study design:
- Type: Comparative, prospective, randomized controlled trial
- Duration: 1 month, including follow-ups.
Participants:
- Inclusion: Adults aged 30–75 with adhesive capsulitis unresponsive to conservative treatment
- Exclusion: Patients with contraindications to anaesthesia/steroids, other shoulder pathologies, or systemic conditions.
Randomisation:
Participants are randomly assigned to:
-
- Group A: MUGA with steroid injection
- Group B: USG-HD with steroid injection.
Interventions:
- Group A (MUA): Shoulder MUA followed by a corticosteroid injection
- Group B (USG HD): USG fluid injection to stretch the joint capsule, with or without steroids.
Outcome measures:
Primary:
-
- Pain relief (SPADI scores)
- ROM (goniometric measurements).
Secondary:
-
- Safety (adverse effects or complications)
- Patient satisfaction (questionnaire on functional improvement and quality of life)
- Long-term outcomes (recurrence and sustained improvements).
Data collection and analysis:
- Data Collection: Baseline demographic, pain, and ROM data; follow-up assessments at immediate post-operative and 1 month.
- Analysis: Statistical comparison of pain and ROM improvements; descriptive statistics for safety and complications.
Ethical considerations:
- Informed consent: Required from all participants
- Ethics approval: Obtained from a review board.
Procedure:
Preparation:
Before the procedure, the patient is typically briefed about what to expect, and any necessary preparations are made. The patient may be given a local anaesthetic or sedative to minimise discomfort during the procedure.
Injection of fluid:
A needle is inserted into the shoulder joint space, usually under ultrasound guidance to ensure precision. A mixture of saline (sterile salt water) and a corticosteroid (such as triamcinolone) is injected into the joint capsule. The amount of fluid injected can vary, but it is typically enough to distend (expand) the capsule.
Distension process:
The injected fluid expands the joint capsule, stretching it beyond its normal capacity. This stretching helps to break up scar tissue and adhesions that have formed within the joint. The pressure created by the fluid can also help to separate the surfaces of the joint, improving ROM.
Post-procedure care:
After the procedure, patients are usually monitored for a short period to ensure there are no immediate complications. They may be advised to rest the shoulder and avoid strenuous activity for a brief period. Physical therapy or exercises to maintain and improve shoulder mobility may be recommended post-procedure.
Complications and side effects:
Pain and discomfort:
Post-procedure pain: Some patients may experience increased pain and discomfort immediately following the procedure. This is usually temporary and can be managed with analgesics.
Infection:
Infection risk: Any procedure involving a needle carries a risk of infection. Proper sterile techniques are crucial to minimise this risk.
Bleeding:
Haematoma: There’s a small risk of bleeding or haematoma formation at the injection site, especially if the patient has bleeding disorders or is on anticoagulants.
Joint capsule rupture:
Rupture risk: Although rare, excessive pressure from the injected fluid could theoretically cause a rupture of the joint capsule or other intra-articular structures.
Nerve injury:
Nerve damage: The procedure carries a small risk of nerve injury, which can cause numbness or tingling.
Increased inflammation:
Flare-up: In some cases, the procedure may cause a temporary flare-up of inflammation, leading to worsened symptoms before improvement.
Allergic reactions:
Reaction to medications: Allergic reactions to the corticosteroids or other components of the injection are possible, though rare.
Long-term effects:
Improved ROM:
Positive outcome: Most patients experience a significant improvement in shoulder ROM and pain reduction following HD.
Residual pain:
Chronic pain: Some individuals may continue to experience mild residual pain or stiffness, especially if the condition was severe before the procedure.
Recurrence:
Potential for recurrence: Adhesive capsulitis may recur or persist in some cases, requiring additional treatments or interventions.
The duration of symptoms for adhesive capsulitis varied among patients. The shortest duration recorded was 3 months, with 1 patient, while the most extended duration was 30 months, also with 1 patient. The highest frequencies were observed at 6 months with 9 patients, 12 months with 10 patients, and 24 months with patients. Other notable durations included 4 months with 4 patients, 8 months with seven patients, and 15 months with five patients. Overall, while some patients experienced symptoms for a few months, others endured them for up to two and a half years (Figs. 1, 2, 3; Tables 1 and 2).
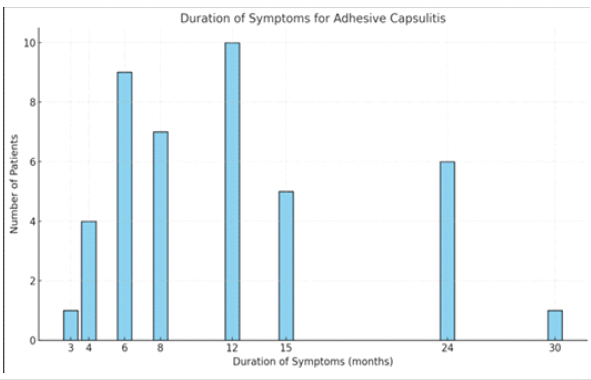
Figure 1: Duration of symptoms among patients with adhesive capsulitis. (This bar graph illustrates the distribution of study participants according to the duration of symptoms (in months) before intervention. The highest number of patients presented at 12 months (n = 10), followed by 6 months (n = 9) and 8 months (n = 7). Other durations included 15 months (n = 5), 4 months (n = 4), and 24 months (n = 6). Fewer patients presented at 3 months and 30 months (n = 1 each), indicating variability in the duration of symptoms before seeking treatment).
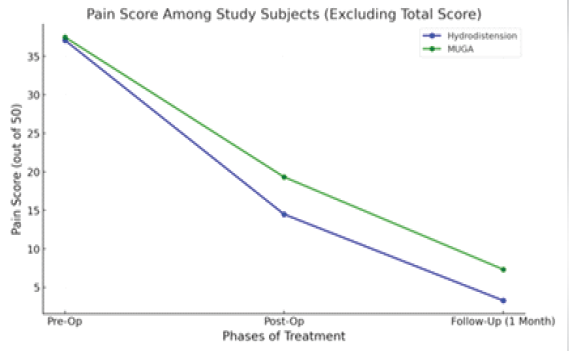
Figure 2: Comparison of pain scores between hydrodistension (HD) and manipulation under anesthesia (MUA) groups. This line graph depicts the comparison of mean pain scores (out of 50) between the HD and manipulation under general anesthesia groups at 3 time points: Pre-operative, post-operative, and at 1-month follow-up. Both groups show a significant reduction in pain scores over time; however, the HD group demonstrates a greater decline in pain scores compared to the MUA group, indicating superior short-term pain relief.
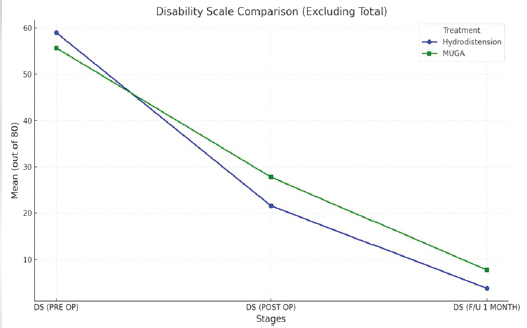
Figure 3: Comparison of disability scores between hydrodistension (HD) and manipulation under anesthesia (MUA) Groups. This line graph illustrates the comparison of mean disability scores (out of 80) between the HD and manipulation under general anesthesia groups at three stages: Pre-operative, post-operative, and 1-month follow-up. Both groups demonstrate a marked reduction in disability scores over time. However, the HD group shows a greater improvement compared to the MUA group at both post-operative and follow-up stages, indicating better short-term functional recovery.
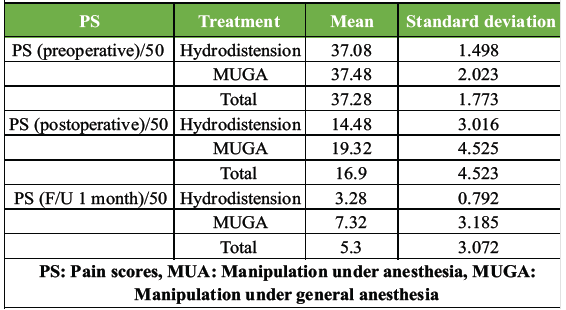
Table 1: Comparison of PS between hydrodistension and MUA groups
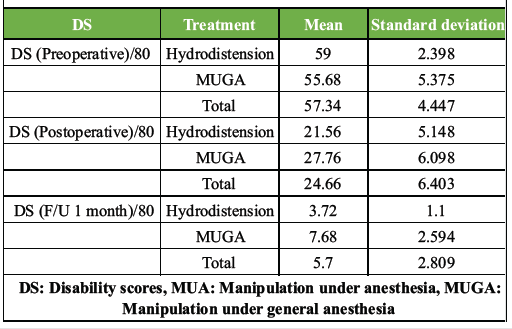
Table 2: Comparison of DS between hydrodistension and MUA groups
The bar graph comparing the SPADI scores for patients undergoing HD and MUGA treatments at different stages: before surgery, after surgery, and at the 1-month follow-up. It illustrates that USG HD led to a more significant reduction in SPADI scores compared to MUGA (Fig. 4).
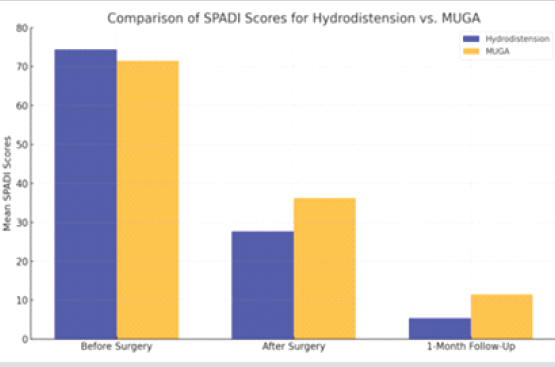
Figure 4: Comparison of shoulder pain and disability index (SPADI) scores between hydrodistension (HD) and manipulation under anesthesia (MUA) Groups. This bar graph compares the mean SPADI scores between the HD and MUGA groups at 3 time points: Before surgery, after surgery, and at 1-month follow-up. Both groups show a significant reduction in SPADI scores over time; however, the HD group demonstrates a greater decrease in scores compared to the MUA group, indicating superior improvement in pain and functional disability in the short term.
Components of the SPADI (Fig. 5):
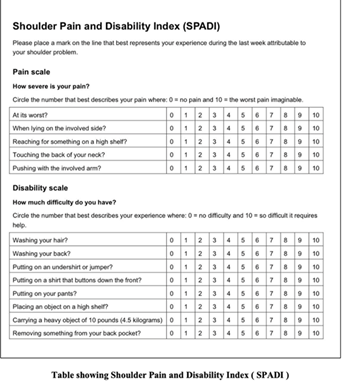
Figure 5: Shoulder pain and disability index (SPADI) questionnaire. This figure shows the SPADI, a validated patient-reported outcome measure used to assess shoulder pain and functional disability. It consists of two components: a pain subscale (5 items) and a disability subscale (8 items), each scored on a scale from 0 to 10. The total score is calculated out of 100 (or subdivided as 50 for pain and 80 for disability in this study), with higher scores indicating greater pain and disability. This tool was used to evaluate treatment outcomes at baseline, post-procedure, and at 1-month follow-up.
Pain subscale:
This part of the questionnaire assesses the intensity of shoulder pain. It typically consists of 5 items where the respondent rates their pain severity during various activities (e.g., lying, lifting, at night) on a scale from 0 (no pain) to 10 (worst pain imaginable).
Disability subscale:
This section evaluates the extent to which shoulder pain interferes with daily activities and functional tasks. It also includes eight items where the respondent rates the difficulty they experience in performing different activities (e.g., washing back, dressing, carrying a bag) on a scale from 0 (no difficulty) to 10 (unable to do).
How it is used:
- Scoring: Scores for each subscale are calculated by summing the responses. The total SPADI score is derived from the sum of the pain and disability subscale scores. Each subscale score can range from 0 to 50, with higher scores indicating more severe pain and disability.
- Interpretation: A higher SPADI score indicates greater shoulder pain and disability. Clinically, changes in SPADI scores over time can help monitor treatment progress or effectiveness.
- Utility: The SPADI is useful for assessing a wide range of shoulder conditions, including rotator cuff tears, shoulder impingement syndrome, osteoarthritis, and shoulder instability.
Advantages:
- Patient-reported: It relies on patient self-reporting, making it suitable for assessing subjective experiences of pain and disability.
- Sensitive to change: It is sensitive to changes in pain and functional status, making it useful for evaluating treatment outcomes.
- Easy to administer: It is relatively quick and straightforward to administer, making it practical for routine clinical use.
Limitations:
- Subjective: Scores may be influenced by individual perceptions and interpretations of pain and disability.
- Specific to shoulder: It is specific to shoulder-related conditions and may not be applicable to other joints or areas of the body.
Overall, the SPADI provides valuable information about the impact of shoulder pain on daily life and helps guide treatment decisions and outcomes assessment in clinical practice.
Hydro distension was introduced by Andren and Lundberg in 1965 as a method to expand the glenohumeral joint capsule for adhesive joints [2]. Involves injecting saline, steroids, anaesthetic, and contrast agents under imaging guidance. Effective in reducing disability scores and improving pain and function compared to MUA. MUA tears the thickened joint capsule and contracted ligaments. However, it can cause capsular tears, labral injuries, and joint damage. Risks include fractures, dislocations, and nerve injuries if not carefully performed. Long-term improvements in pain and ROM were observed in some studies, especially when performed after failed conservative treatment. Comparative results (HD vs. MUA): HD showed superior pain and disability relief at 1-month follow-up compared to MUA. In our study, disability scores for shoulder adhesive capsulitis patients were assessed before the procedure, after the procedure, and 1 month post-operation. Patients underwent either MUGA or USG HD. Mean pain scores post-HD (3.28) were significantly lower than post-MUA (7.32). The mean disability scores decreased from 59.00 to 3.72 for the HD group and from 55.68 to 7.68 for the MUGA group. USG HD led to greater improvement compared to MUGA (F = 13.511, P = 0.001). SPADI scores indicated greater improvement with HD (mean score reduction to 5.38) than MUA (11.45). Watson et al. found significant improvements in functional outcomes at 3 months, 1 year, and 2 years post-treatment. The SPADI scores at 3 months showed improvements in external rotation (−0.21), shoulder abduction (−0.37), and hand behind back (−0.26). At 1 year, improvements were −0.19, −0.28, and −0.27, respectively. At 2 years, the scores were −0.23, −0.21, and −0.14, respectively. The SDI scores also showed significant improvements at 3 months and up to 2 years [3]. In this study, pain and SPADI scores for patients with shoulder adhesive capsulitis were analysed before the procedure, after the procedure, and 1 month post-operation. Patients underwent either MUGA or USG HD. In 2018, Saltychev et al. conducted a meta-analysis to evaluate the overall effectiveness of hydrodilatation in the treatment of FS syndrome. They synthesised existing evidence and concluded on its efficacy based on the collective findings of relevant studies up to that point [4]. Surgeons always faced the challenge of potential complications associated with MUA for FS syndrome, including humeral shaft fractures, glenoid fractures, rotator cuff tears, shoulder dislocations, and nerve traction injuries [5,6]. Tsvieli et al. addressed these risks by applying their method based on understanding Codman’s paradox, which involves minimising rotational forces on the humerus during MUA. Their technique involved elevating the arm in the scapular plane with a short lever arm, followed by lowering the externally rotated arm without rotation, thereby reducing torque on the humerus [7]. USG HD has been employed using both anterior and posterior approaches in clinical practice. Evidence suggests that the anterior approach may offer superior efficacy compared to the traditional posterior method. This approach is believed to facilitate more effective distribution of the injected mixture into affected areas, potentially enhancing distention and addressing concurrent conditions like biceps tenosynovitis, which commonly co-occurs. In addition, the anterior approach is noted for its technical advantages in obese patients, allowing direct patient interaction and evaluation of pain-related facial expressions during the procedure [8]. Furthermore, it is suggested that the anterior approach may aid in releasing adhesions between the intracapsular portion of the long head of the biceps tendon and the superior border of the subscapularis tendon [2]. Early initiation of physiotherapy plays a crucial role in the management of adhesive capsulitis. A combination of stretching exercises, manual therapy, and strengthening protocols has been shown to significantly improve functional outcomes. Adjunctive modalities such as superficial heat and therapeutic ultrasound may provide temporary symptomatic relief; however, their long-term benefits remain limited. Patient education and self-directed home exercise programmes are equally important, as they enhance adherence to therapy and contribute to sustained functional recovery. Additional observations suggest that the timing of intervention is an important determinant of outcomes, with MUA considered most effective when performed between 6 and 9 months after symptom onset, potentially reducing recurrence rates [9,10]. However, variability in treatment protocols and clinical outcomes across studies highlights the need for standardised management strategies. Combined interventions, such as HD with corticosteroid injection, have shown promising results, although evidence regarding their superiority remains inconsistent. USG procedures offer distinct advantages due to their high precision, enabling accurate localisation and targeted intra-articular delivery of anti-inflammatory agents. This not only ensures effective capsular distension but also allows real-time, on-table assessment of ROM. USG-guided intra-articular steroid injections provide rapid pain relief, which is a key factor in improving patient compliance with physiotherapy. Furthermore, these procedures are associated with lower recurrence rates, particularly in the case of HD. In the present study, patients undergoing MUA did not experience immediate pain relief, which significantly limited their ability to participate in early post-operative physiotherapy due to pain and discomfort. This may have contributed to relatively poorer short-term functional outcomes. In contrast, patients treated with USG-guided HD experienced earlier pain relief, likely due to precise corticosteroid delivery and effective capsular stretching. This facilitated better engagement in physiotherapy, resulting in improved ROM and functional recovery. Therefore, the superior short-term outcomes observed with USG-guided interventions can be attributed to their precision, early analgesic effect, and enhanced rehabilitation compliance.
Adhesive capsulitis, or FS, is a condition marked by pain, stiffness, and functional impairment. This study compared two treatment methods:
- MUGA with steroid injection
- USG hydro distention with steroid injection.
- Both treatments significantly improved pain, mobility, and functional outcomes, measured using the PADI scale.
- MUA with steroid injection: Provided rapid pain relief and immediate improvement in shoulder ROM by mechanically releasing adhesions. However, some patients experienced symptom recurrence and joint re-fibrosis.
- USG-Guided Hydro distention: A minimally invasive technique using fluid injection to stretch the capsule, demonstrated greater long-term pain relief and functional recovery with fewer recurrences.
Our observations were:
- Pre-treatment pain and disability scores were similar in both groups.
- At 1-month follow-up, hydro distention showed significantly lower SPADI scores compared to MUA, indicating superior efficacy.
- The majority of patients had symptoms for 6–12 months, with the right shoulder being more commonly affected.
While both treatments are effective, USG-guided hydrodistention provided better long-term outcomes in pain reduction and functional recovery. The choice of treatment should consider patient preferences, symptom severity, and clinical factors.
Future directions:
- Larger randomised controlled trials to confirm findings.
- Exploration of adjunctive therapies (e.g., physical therapy) and novel pharmacological agents.
- Advancements in imaging and biomarkers to tailor personalised treatments.
Ultrasound-guided interventions in adhesive capsulitis provide precise, targeted delivery of anti-inflammatory medication, resulting in rapid pain relief, improved ROM, and lower recurrence rates. The ability to perform real-time assessment and achieve early analgesia enhances patient compliance with physiotherapy, leading to better overall functional recovery compared to non-guided techniques.
References
- 1. Wu F, Kachooei AR, Ebrahimzadeh MH, Bagheri F, Hakimi E, Shojaie B, et al. Bilateral arm-abduction shoulder radiography to determine the involvement of the scapulothoracic motion in frozen shoulder. Arch Bone Jt Surg 2018;6:225-32. [Google Scholar] [PubMed]
- 2. Hubbard MJ, Hildebrand BA, Battafarano MM, Battafarano DF. Common soft tissue musculoskeletal pain disorders. Prim Care 2018;45:289-303. [Google Scholar] [PubMed]
- 3. Oderuth E, Ali M, Atchia I, Malviya A. A double blind randomised control trial investigating the efficacy of platelet rich plasma versus placebo for the treatment of greater trochanteric pain syndrome (the HIPPO trial): A protocol for a randomised clinical trial. Trials 2018;19:517. [Google Scholar] [PubMed]
- 4. Rugg CM, Hettrich CM, Ortiz S, Wolf BR, MOON Shoulder Instability Group. Zhang AL. Surgical stabilization for first-time shoulder dislocators: A multicenter analysis. J Shoulder Elbow Surg 2018;27:674-85. [Google Scholar] [PubMed]
- 5. Jahn S, Seror J, Klein J. Lubrication of articular cartilage. Annu Rev Biomed Eng 2016;18:235-58. [Google Scholar] [PubMed]
- 6. Kadi R, Milants A, Shahabpour M. Shoulder Anatomy and normal variants. J Belg Soc Radiol 2017;101 Suppl 2:3. [Google Scholar] [PubMed]
- 7. Varacallo M, Seaman TJ, Mair SD. Biceps tendon dislocation and instability. In: StatPearls. StatPearls Publishing; Treasure Island, FL; 2023. [Google Scholar] [PubMed]
- 8. Schmidt CC, Jarrett CD, Brown BT. Management of rotator cuff tears. J Hand Surg Am 2015;40:399-408. [Google Scholar] [PubMed]
- 9. Hubbard MJ, Hildebrand BA, Battafarano MM, Battafarano DF. Common Soft Tissue Musculoskeletal Pain Disorders. Prim Care. 2018;45(2):289-303. [Google Scholar] [PubMed]
- 10. Xiao RC, DeAngelis JP, Smith CC, Ramappa AJ. Evaluating nonoperative treatments for adhesive capsulitis. Winter J Surg Orthop Adv 2017;26:193-9. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Comparative Outcome Analysis of Leukocyte-Rich Platelet-rich Plasma, Leukocyte-Poor Platelet-rich Plasma, Injectable Platelet-rich Fibrin and Corticosteroid Injections in Periarthritis of the Shoulder: A Double-Blinded, Four-Arm Randomized Controlled Trial
August 1, 2026 Comparative Outcome Analysis of Leukocyte-Rich Platelet-rich Plasma, Leukocyte-Poor Platelet-rich Plasma, Injectable Platelet-rich Fibrin and Corticosteroid Injections in Periarthritis of the Shoulder: A Double-Blinded, Four-Arm Randomized Controlled Trial February 1, 2026 Outcomes of Clinico-radiologically Predetermined Patient-specific Multi-site Steroid Injection in Primary Frozen Shoulder: A Prospective Study
February 1, 2026 Outcomes of Clinico-radiologically Predetermined Patient-specific Multi-site Steroid Injection in Primary Frozen Shoulder: A Prospective Study December 1, 2025 Functional Outcome of Intra-articular Platelet-Rich Plasma in the Treatment of Frozen Shoulder
December 1, 2025 Functional Outcome of Intra-articular Platelet-Rich Plasma in the Treatment of Frozen Shoulder November 1, 2025 Comparative Efficacy of Manipulation Under Anaesthesia Versus Arthroscopic Capsular Release in Primary Frozen Shoulder: A Prospective Randomized Study
November 1, 2025 Comparative Efficacy of Manipulation Under Anaesthesia Versus Arthroscopic Capsular Release in Primary Frozen Shoulder: A Prospective Randomized Study