
Larger Cage Footprint Improves Stability The LTLIF cage provides wider endplate coverage, improving load distribution and reducing focal stress concentration on the vertebral endplates. This may reduce the risk of cage migration and cage subsidence.
Dr. Ayush Sharma, Department of Spine Surgery, Dr. Babasaheb Ambedkar Memorial Hospital, Mumbai, Maharashtra, India. E-mail: drayush@gmail.com
Abstract
Introduction: Transforaminal lumbar interbody fusion (TLIF) is a widely accepted surgical technique for the management of degenerative lumbar spondylolisthesis. The procedure provides circumferential decompression, restoration of disc height, and segmental stabilization. Despite favorable outcomes, complications such as interbody cage migration or posterior cage back-out may occur, compromising surgical success and necessitating revision surgery.
Case Report: We present the case of a 45-year-old male with symptomatic degenerative L4–L5 spondylolisthesis who underwent minimally invasive TLIF (MIS-TLIF) after failure of conservative treatment. Postoperatively, the patient developed posterior migration of the interbody cage with neural compression leading to cauda equina syndrome. Revision MIS-LTLIF (MIS-TLIF using a large-footprint cage) was performed with the removal of the migrated cage of size 9 × 22 mm and insertion of a larger-footprint interbody cage of size 10 × 40 mm following meticulous bilateral disc space clearance and endplate preparation. Post-revision surgery imaging demonstrated stable implant positioning, and the patient showed significant clinical improvement without further complications.
Conclusion: Interbody cage back-out following TLIF is a preventable complication. Inadequate disc space preparation and selection of a suboptimal cage footprint may significantly contribute to cage migration. Proper surgical technique and appropriate implant choice are essential to ensure construct stability and favorable clinical outcomes.
Keywords: Degenerative spondylolisthesis, transforaminal lumbar interbody fusion, LTLIF, cage migration, lumbar spine, revision spine surgery
Degenerative lumbar spondylolisthesis is a common cause of low back pain and radiculopathy in adults, most frequently involving the L4–L5 motion segment. It results from progressive intervertebral disc degeneration, facet joint arthropathy, and ligamentous laxity, leading to anterior translation of the cephalad vertebra and segmental instability [1,2,3]. Clinically, patients may present with mechanical low back pain, radicular symptoms, or neurogenic claudication, often resulting in significant functional disability and reduced quality of life. Surgical intervention is indicated in patients with persistent symptoms who fail adequate conservative management. Transforaminal lumbar interbody fusion (TLIF) has gained widespread acceptance as an effective surgical option for degenerative spondylolisthesis, as it allows decompression of neural elements, restoration of disc height, and circumferential fusion through a unilateral posterior approach while minimising neural retraction [4,5,6]. Favourable clinical and radiological outcomes have been reported with TLIF when appropriate patient selection and surgical technique are employed [7]. Despite its advantages, TLIF is not devoid of complications. Interbody cage migration, particularly posterior cage back-out, is a recognised but potentially preventable complication that may lead to recurrent pain, neurological compromise, loss of fusion potential, and the need for revision surgery [8,9,10]. Several factors have been implicated in cage migration, including inadequate disc space preparation, improper cage sizing, insufficient endplate contact, cage positioning, and biomechanical instability at the operated segment [11,12,13]. This case report describes interbody cage back-out following TLIF for degenerative L4–L5 spondylolisthesis and highlights the critical role of meticulous disc space preparation and appropriate cage footprint selection in preventing this complication.
A 45-year-old male presented with chronic low back pain associated with left radicular pain radiating along the L5 dermatome. Symptoms had progressively worsened over several months and were aggravated by prolonged standing and walking. The patient had undergone more than 6 months of conservative treatment, including non-steroidal anti-inflammatory drugs, activity modification, and supervised physiotherapy, without satisfactory relief (Fig. 1).
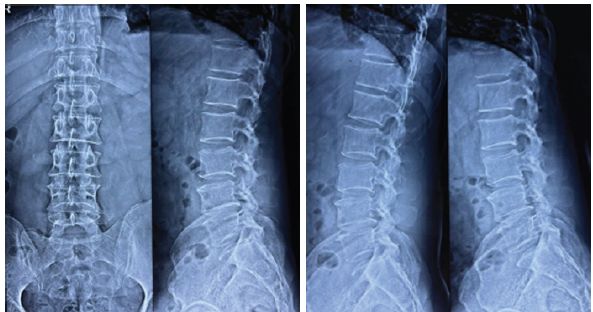
Figure 1: X-ray lumbosacral spine anteroposterior view and lateral flexion and extension view before index surgery.
Neurological examination revealed radicular pain without objective motor weakness. Sensory examination was normal, deep tendon reflexes were preserved, and there was no bowel or bladder involvement. Plain radiographs of the lumbosacral spine demonstrated degenerative Grade 1 spondylolisthesis at the L4–L5 level. Dynamic flexion–extension views suggested segmental instability. Magnetic resonance imaging revealed disc degeneration at L4–L5 with associated central canal stenosis and compression of the traversing nerve roots in combination with bilateral facet arthropathy, correlating with the patient’s clinical presentation. Computed tomography was used to further assess bony anatomy and assist in surgical planning (Fig. 2).
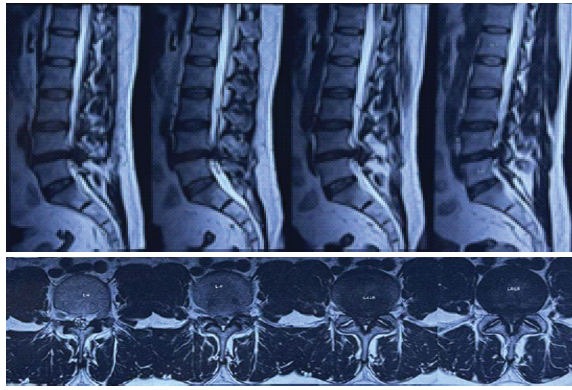
Figure 2: Magnetic resonance imaging lumbosacral spine T2 sagittal axial views before index surgery.
Given the persistence of symptoms despite adequate conservative management and the presence of radiological instability, surgical intervention was planned. The patient underwent an uneventful minimally invasive TLIF for the L4–L5 level in another hospital. An interbody cage of size 9 × 22 mm was inserted following disc removal, and posterior instrumentation was applied. Immediate post-operative radiographs were satisfactory. On post-operative day 5, the patient started complaining of weakness in both lower limbs, urinary retention, and bowel disturbances. Subsequent imaging revealed posterior migration (back-out) of the interbody cage. The patient was subsequently referred to our tertiary spine care center for further management. Considering the intracanalicular location of the cage and cauda equina syndrome, emergency revision surgery was planned (Fig. 3).
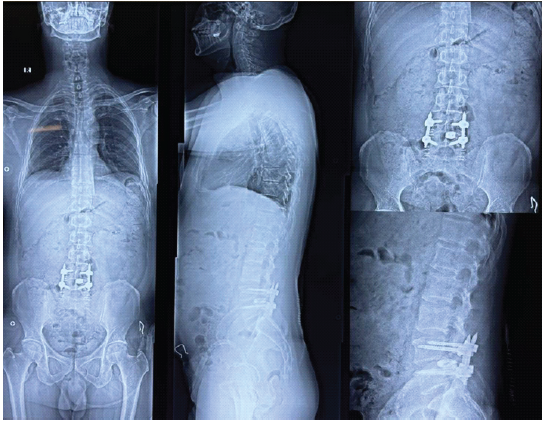
Figure 3: X-ray lumbosacral (LS) whole spine with focused LS spine anteroposterior view and lateral view after index surgery, indicating cage back-out.
Revision surgery involved the MIS-LTLIF approach with removal of the migrated cage from the left side. A complete contralateral facetectomy was then performed on the right side. The disc space was thoroughly re-explored, and meticulous disc clearance was performed bilaterally with careful preparation of the vertebral endplates while preserving subchondral bone. A larger-footprint interbody cage measuring 10 × 40 mm was selected and inserted using a reverse orthogonal maneuver from the right side to orient the large-footprint cage in an optimal position. Final stabilization was achieved with pedicle screw instrumentation. Post-revision radiographs and computed tomography confirmed appropriate cage positioning and restoration of disc height without evidence of migration. The patient demonstrated significant improvement in low back pain, lower limb weakness with complete recovery of bowel and bladder function over a 6-week period and remained clinically stable without further complications (Fig. 4).
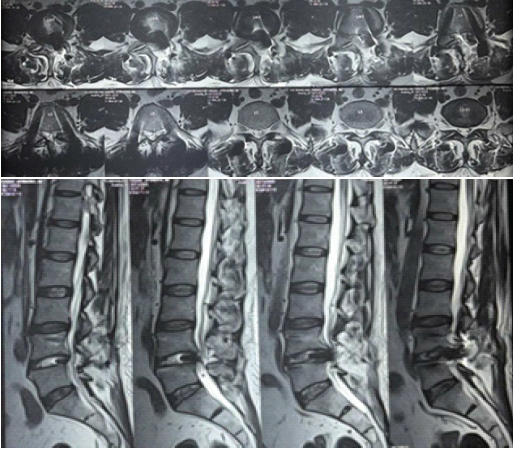
Figure 4: Magnetic resonance imaging lumbosacral spine T2 sagittal axial views after index surgery, indicating cage back-out.
Interbody cage migration following TLIF is an infrequent but clinically significant complication. Posterior cage back-out may result in recurrent pain, neurological compromise, construct instability, and failure of fusion [8,9,10]. The etiology of cage migration is multifactorial and includes implant-related, technical, and patient-specific factors (Fig. 5).
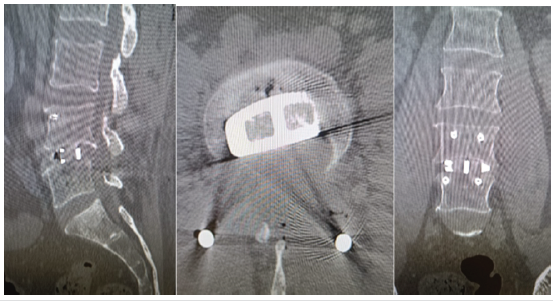
Figure 5: Final post-operative computed tomography lumbosacral spine with large footprint cage.
Inadequate disc space preparation is a critical technical factor contributing to cage instability. Residual disc material and insufficient endplate preparation can prevent optimal cage seating, reduce frictional resistance, and compromise cage-endplate contact, thereby increasing the risk of migration [11,12]. Preservation of subchondral bone while achieving adequate endplate exposure is essential to ensure stable cage placement and promote fusion. Cage footprint and appropriate cage height also play pivotal roles in preventing migration. Larger-footprint cages increase the contact surface area between the implant and vertebral endplates, thereby improving load distribution and reducing peak endplate stress. This reduces focal stress concentration on the vertebral endplates and enhances resistance to posterior migration [13,14,15,16]. This is particularly important in degenerative spondylolisthesis, where inherent segmental instability and altered biomechanics increase the risk of implant failure. In the present case, revision surgery with meticulous disc space preparation and insertion of a larger footprint cage via the MIS-LTLIF approach resulted in stable fixation and a satisfactory clinical outcome. This highlights the importance of surgical technique and appropriate implant selection in preventing cage back-out following TLIF.
Interbody cage back-out following TLIF is a preventable complication. Thorough disc space preparation and selection of an adequately sized, large footprint interbody cage are essential for achieving stable fixation and preventing cage migration. Early diagnosis and timely revision surgery using appropriate surgical technique can lead to favorable clinical outcomes
Meticulous disc preparation and appropriate large-footprint cage selection are critical in preventing cage migration following TLIF for degenerative lumbar spondylolisthesis .
References
- 1. Jacobsen S, Sonne-Holm S, Rovsing H, Monrad H, Gebuhr P. Degenerative lumbar spondylolisthesis: An epidemiological perspective: The copenhagen osteoarthritis study. Spine (Phila Pa 1976) 2007;32:120-5. [Google Scholar] [PubMed]
- 2. Kalichman L, Hunter DJ. Diagnosis and conservative management of degenerative lumbar spondylolisthesis. Eur Spine J 2008;17:327-35. [Google Scholar] [PubMed]
- 3. Resnick DK, Watters WC. Lumbar spondylolisthesis: Classification and management. Neurosurg Focus 2002;13:E1. [Google Scholar] [PubMed]
- 4. Harms J, Rolinger H. A one-stager procedure in operative treatment of spondylolistheses: Dorsal traction-reposition and anterior fusion (author’s transl). Z Orthop Ihre Grenzgeb 1982;120:343-7. [Google Scholar] [PubMed]
- 5. Lowe TG, Tahernia AD, O’Brien MF, Smith DA. Unilateral transforaminal posterior lumbar interbody fusion (TLIF): Indications, technique, and 2-year results. J Spinal Disord Tech 2002;15:31-8. [Google Scholar] [PubMed]
- 6. Humphreys SC, Hodges SD, Patwardhan AG, Eck JC, Murphy RB, Covington LA. Comparison of posterior and transforaminal approaches to lumbar interbody fusion. Spine (Phila Pa 1976) 2001;26:567-71. [Google Scholar] [PubMed]
- 7. Rosenberg WS, Mummaneni PV. Transforaminal lumbar interbody fusion: Technique, complications, and early results. Neurosurgery 2001;48:569-74; discussion 574-5. [Google Scholar] [PubMed]
- 8. Chen L, Yang H, Tang T. Cage migration in spondylolisthesis treated with posterior lumbar interbody fusion using BAK cages. Spine (Phila Pa 1976) 2005;30:2171-5. [Google Scholar] [PubMed]
- 9. Kimura H, Shikata J, Odate S, Soeda T. Risk factors for cage retropulsion after PLIF. Spine (Phila Pa 1976) 2009;34:E837-43. [Google Scholar] [PubMed]
- 10. Rickert M , Fennema P , Wehner D, Rahim T , Hölper B, Eichler M, et al. Cage migration and subsidence after lumbar interbody fusion. World Neurosurg 2016;90:242-50. [Google Scholar] [PubMed]
- 11. Marchi L, Oliveira L, Amaral R, Abdala N, Coutinho E, Pimenta L, et al. Radiographic and clinical evaluation of cage migration after lumbar interbody fusion. Neurosurg Focus 2019;46:E10. [Google Scholar] [PubMed]
- 12. Kim MC, Chung HT, Cho JL, Kim DJ, Chung NS. Factors affecting cage migration after TLIF. Clin Spine Surg 2020;33:E252-8. [Google Scholar] [PubMed]
- 13. Abbushi A, Cabraja M, Thomale UW, Woiciechowsky C, Kroppenstedt SN. Influence of cage positioning and footprint on TLIF outcomes. Eur Spine J 2017;26:1463-72. [Google Scholar] [PubMed]
- 14. Phan K, Rao PJ, Mobbs RJ. Biomechanics of large footprint interbody cages. Orthop Surg 2018;10:187-95. [Google Scholar] [PubMed]
- 15. Wang H, Zhou Y, Li C, Liu J, Xiang L. Endplate preparation and cage footprint selection in lumbar interbody fusion. BMC Musculoskelet Disord 2022;23:416. [Google Scholar] [PubMed]
- 16. Rangnekar A, Sharma A, Naseem A, Agrawal H, Gajbhiye K, Marathe N, et al. Intraoperative Anteropulsion of an Interbody Fusion Cage During MIS-TLIF: Management and Technical Considerations. J Minim Invasive Spine Surg Tech. 2023;8(2):226-230. doi:10.21182/jmisst.2023.00787. [Google Scholar] [PubMed] [CrossRef]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Hybrid Posterior Fixation Incorporating Cervical Facet Fixation for the Treatment of Proximal Junctional Failure
July 1, 2026 Hybrid Posterior Fixation Incorporating Cervical Facet Fixation for the Treatment of Proximal Junctional Failure July 1, 2026 Acute Cauda Equina Syndrome Following Transpedicular Biopsy of a Lumbar Vertebral Lesion: A Case Report of Spinal Non-Hodgkin’s Lymphoma
July 1, 2026 Acute Cauda Equina Syndrome Following Transpedicular Biopsy of a Lumbar Vertebral Lesion: A Case Report of Spinal Non-Hodgkin’s Lymphoma January 1, 2026 Outcomes of Unilateral Biportal Endoscopic Surgery for Prolapsed Intervertebral Disc: A Single-center Study
January 1, 2026 Outcomes of Unilateral Biportal Endoscopic Surgery for Prolapsed Intervertebral Disc: A Single-center Study October 1, 2025 Do Spino-pelvic Parameters Predict Development of Spondylolisthesis in Degenerative Disc Disease at the L4-5 Level
October 1, 2025 Do Spino-pelvic Parameters Predict Development of Spondylolisthesis in Degenerative Disc Disease at the L4-5 Level