
This article highlights the successful use of surgical management and an early rehabilitation strategy for a rare significantly displaced intra-articular radial head fracture in a skeletally immature patient to achieve complete recovery.
Dr. Haritha Haridas Mandoth Veetil, Princess Royal University Hospital, Orpington, United Kingdom. E-mail: haritha.veetil@nhs.net
Abstract
Introduction: Radial head (RH) fractures are relatively uncommon injuries in children, typically resulting from a fall onto an outstretched hand, and can pose significant challenges in diagnosis and management, particularly when they are displaced or involve the articular surface.
Case Report: A 12-year-old female sustained a comminuted, displaced, partial-articular fracture of the RH following a fall onto her arm during a netball game. Open reduction and internal fixation were performed using headless compression screws. Post-operative recovery was uneventful with a full range of motion at 3-month follow-up.
Conclusion: This case highlights the successful surgical management and early rehabilitation strategy of a rare, significantly displaced intra-articular RH fracture in a young child.
Keywords: Radial head fracture, paediatric.
Intra-articular radial head (RH) fractures in paediatric patients are uncommon, and those with significantly displaced fragments present unique management challenges due to the complexity of the elbow physeal anatomy, small size of fragments and the potential for growth disruption at the associated growth plate. While undisplaced fractures can often be treated conservatively, a grossly displaced intra-articular fracture is an indication for operative fixation to restore joint congruity and function while minimising growth plate disturbance. This case report aims to contribute to the limited body of evidence on surgical management of comminuted displaced intra-articular RH fractures in skeletally immature patients, emphasising the role of advanced imaging, meticulous surgical technique and structured rehabilitation in optimising outcomes.
A 12-year-old fit and well female presented to the emergency department with pain and restriction in movement after falling onto her left arm during a netball game. Clinical examination revealed localised tenderness laterally over the RH with no significant swelling, ecchymosis or any open wounds. Neurovascular function was intact.
Investigations:
Lateral and attempted anteroposterior plain radiographs of the elbow demonstrated a displaced fracture of the RH in a skeletally immature patient (Fig. 1a and b).
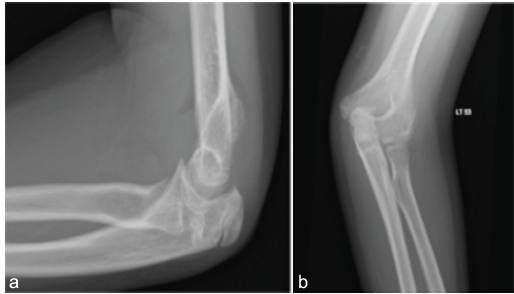
Figure 1: (a) Lateral radiograph of elbow showing a proximally displaced radial head fragment. (b) Attempted anteroposterior radiograph of elbow with radial head fracture fragments hidden behind the capitellum.
A pre-operative computed tomography (CT) of the elbow (Figs. 2a and b) revealed a comminuted partial-articular Salter-Harris (SH) type 3 fracture involving 50% of the anterior RH, which was in two fragments, both having migrated posteriorly and proximally.
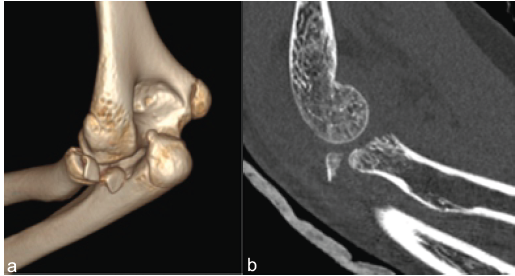
Figure 2: (a) Computed tomography (CT) 3D reconstruction demonstrating two radial head fragments displaced dorsal to radiocapitellar joint. (b) Sagittal section of CT demonstrating posteriorly displaced radial head fragment.
Reformatting of the CT images estimated the two fragments to be 4.2 mm in depth and each approximately a quarter of an RH with an original diameter of 15.9 mm. The scan also confirmed posterior subluxation of the RH with the appearance of a posterior capitellum Osborne-Cotterill lesion. The ulno-humeral joint was congruent, and all ossification centres were present in accordance with her age. Relevantly, the physis seen of the non-fractured proximal radius appeared to be ossified. There were no other obvious injuries to bone or growth plates.
Treatment:
The significance of the disruption to the RH articular surface and displacement of the fragments, along with subluxation at the radiocapitellar joint, were all indications for surgery to reduce and fix the fracture while restoring joint congruency and stability. Appropriate explanation, discussion, and informed consent with the patient and her parents were carried out, but due to the availability of an upper limb surgeon, surgery was delayed until 12 days post-injury. She underwent open reduction and internal fixation (ORIF) under general anaesthesia in the supine position with a high-arm tourniquet and standard preparation with betadine and chlorhexidine. A lateral longitudinal incision over the left elbow was made using the extensor digitorum communis (EDC) splitting approach. The lateral ulnar collateral ligament was found to be intact with no significant Osborne-Cotterill lesion. The annular ligament was incised longitudinally to expose the RH and fracture. Two fracture fragments representing >50% of the RH were identified posteriorly within the capsule. These fragments were reduced and fixed together extracorporeally on the table using a 1.7 mm cannulated headless compression screw (HCS). The reconstituted half of the RH was then reduced and fixed to the intact RH and neck under direct vision and with an intra-operative image intensifier using two 2.2 mm cannulated HCS in a tripod configuration. All screw heads were buried under cartilage to avoid articular prominence (Fig. 3a and b).
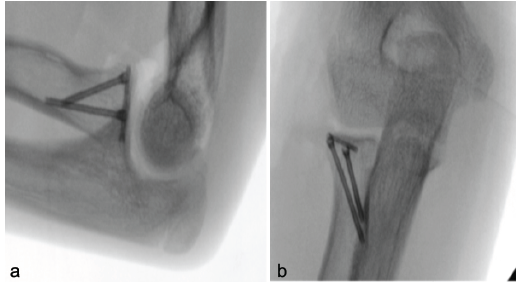
Figure 3: (a) Lateral intraoperative fluoroscopy demonstrating one transverse headless compression screw (HCS) and two HCS in tripod configuration. (b) Anteroposterior intraoperative fluoroscopy demonstrating one transverse HCS and two HCS in tripod configuration.
After fixation, examination with intra-operative imaging confirmed a stable fracture and congruent radiocapitellar and ulnohumeral joints. Full range of motion (ROM) of the elbow and forearm in all directions was demonstrated, and elbow stability under varus and valgus stress was evident. The annular ligament and EDC were repaired, followed by appropriate wound closure, dressing, and application of a bulky bandage using wool and crepe, but no plaster immobilisation.
Post-operative rehabilitation:
Postoperatively, the patient was given adequate analgesia and given instructions for gentle active elbow mobilisation limited to 30° to 130° of flexion and 60° of pronation to 60° of supination for the first 4 weeks before allowing a full ROM. She was encouraged to mobilise her shoulder, wrist, and fingers immediately and advised to avoid lifting, loading, and resistance for 6 weeks, after which there were no restrictions.
Outcome and follow-up:
The patient was reviewed at 9 days, 6 weeks, 3 months, and 12 months postoperatively, with formal physiotherapy starting at 2 weeks following surgery. She made an uneventful recovery with near-full ROM at 6 weeks. Relevant post-operative radiographs at that stage demonstrated satisfactory positions of implants and fragments with evidence of lateral callus (Fig. 4a and b). She had a full pain-free ROM and function at both 3-month and 12-month follow-ups (Fig. 5a, b, c, d, e).
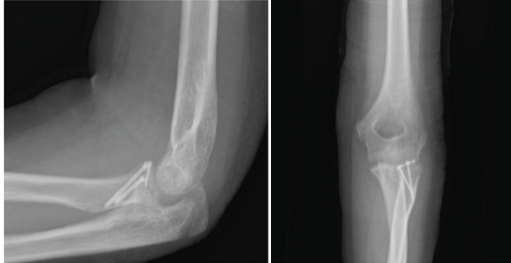
Figure 4: (a) Lateral view of elbow 2 weeks post-operative radiograph. (b) Anteroposterior view of the elbow 2 weeks post-operative radiograph.
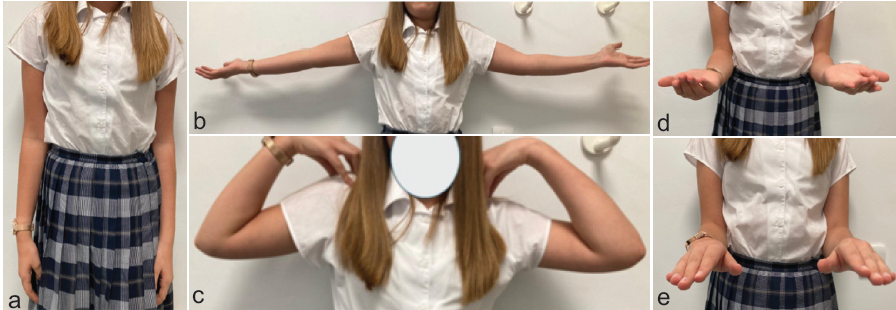
Figure 5: (a) Normal appearance of arm after 3 months post-operative. (b) Full range of motion (ROM) on extension of elbow after 3 months post-operative. (c) Full range of motion (ROM) on flexion of elbow after 3 months post-operative. (d) Full ROM on supination after 3 months post-operative. (e) Full ROM on pronation after 3 months post-operative.
RH and neck fractures represent approximately 14% of all paediatric fractures and about 4–7% of elbow injuries in children [1,2]. The mechanism of injury often involves a fall on an outstretched arm, commonly producing valgus stress and axial loading, and resulting in compressive forces between the RH and the capitellum [3,4]. The resulting injury is frequently a radial neck fracture, undisplaced or displaced. In the case we present, the posterior subluxation at the radiocapitellar joint seen on CT and anterior fracture fragments was a suggestion that the mechanism of injury also involved a supinated forearm and posterior force on the RH, likely as part of the posterolateral rotatory instability spectrum. In paediatric patients, an associated capsuloligamentous injury is rarely seen due to the elasticity of the soft tissues [5]. Paediatric fractures differ significantly from adult fractures due to their open growth plates. The incomplete and varied extent of ossification of the epiphyses and physes, dependent on age, complicates both diagnosis and treatment [6]. Radial neck fractures in children are usually caused by a fall on an outstretched hand with valgus stress at the elbow. The Judet classification for paediatric radial neck fractures and the modified Mason classification for adult RH fractures help guide treatment decisions [7]. Non-operative treatment is generally preferred for non-displaced or minimally displaced fractures. With radial neck fractures in children, less than either 30° angulation or 3 mm translation is an indication for conservative management [1]. For RH fractures, surgical intervention must be considered for intra-articular fractures with significantly displaced fragments, especially if a mechanical block to motion exists or if satisfactory reduction cannot be restored by closed means [8,9,10]. Kalbitz et al. discussed his series of 67 paediatric RH fractures, but of these, only 2 were SH type 3, both without comminution, and there was no described treatment for these specifically [1]. We were unable to locate any evidence available specifically for the treatment of displaced intra-articular paediatric RH fractures. In our case, the fracture was partial-articular, significantly displaced, and comminuted with a subluxated proximal radius. If treated non-operatively, predictably, there may be a high chance of a resulting restriction in movement, particularly extension and pronosupination, due to the posterior positioning of the displaced fragments. The lead author felt ORIF was essential for this injury pattern to restore joint congruency, allow early mobilisation, and retain function. A lateral EDC-split approach was chosen for optimal visualisation of the RH and neck and reduced risk to the posterior interosseous nerve compared to the Kaplan approach [11,12]. Headless screws were selected for fixation due to their compressive stability, low profile, and minimal risk of hardware prominence – which is especially critical with articular fragments [13,14,15]. The other issue here was due to the young age of the patient (i.e., 12 years of age) and comminution; the fragments were small and may not have been amenable to systems with larger 3.5 mm or 2.5 mm HCS. We were able to utilise smaller 2.2 mm and 1.7 mm HCS options to capture and fix these lesser-sized fragments with adequate compression and without further fragment blow-out. This is an important consideration in a young paediatric patient where RH fracture reduction and stabilisation are key to preserve the joint, and RH replacement is not an option, logically and practically. Prolonged immobilisation in adults increases the risk of elbow stiffness, the most common complication following RH surgery [16,17]. Elbow stiffness is rarely an issue, though, in the paediatric population with adequately positioned or reduced fractures. Post-fixation rehabilitation still requires a cautious approach to prevent subsequent implant failure and fracture re-displacement, particularly in a non-adherent or non-compliant child. Patient and parent education and information are paramount, and post-operative rehabilitation may need to be cautiously tailored. Early but protected ROM, as implemented in our case, allowed satisfactory outcomes without short-term complications. Complications such as growth disturbance, physeal closure, and the rare occurrence of heterotopic ossification (HO) in children can lead to long-term complications such as loss of motion and function, so such injuries require ongoing surveillance [14,18]. Our patient’s recovery was uncomplicated and showed good functional results with early motion following anatomic fixation.
Displaced intra-articular RH fractures in children are uncommon but can significantly affect function if mismanaged, so they require precise evaluation and treatment planning. In severely displaced cases, ORIF can provide reliable fracture stabilisation and allow early rehabilitation. Continued follow-up is essential to detect potential growth-related complications.
This case report demonstrates that prompt surgical intervention combined with an early, structured rehabilitation protocol can result in excellent functional and radiological outcomes in skeletally immature patients with rare, significantly displaced intra-articular radial head fractures. The case emphasises the importance of achieving anatomical reduction and stable fixation in order to restore elbow congruity, facilitate early mobilisation, and minimise the risk of long-term complications such as stiffness, functional deficit, and growth disturbance in this uncommon paediatric injury pattern.
References
- 1. Kalbitz M, Lackner I, Perl M, Pressmar J. Radial head and neck fractures in children and adolescents. Front Pediatr 2023;10:988372. [Google Scholar] [PubMed]
- 2. Yang L, Yang X, Zuo J, Wang D, Li L, Tang X. A retrospective review of 101 operatively treated radial neck fractures in children and analysis of risk factors for functional outcomes. Injury 2022;53:3310-16. [Google Scholar] [PubMed]
- 3. Swensen SJ, Tyagi V, Uquillas C, Shakked RJ, Yoon RS, Liporace FA. Maximizing outcomes in the treatment of radial head fractures. J Orthop Traumatol 2019;20:15. [Google Scholar] [PubMed]
- 4. Harbrecht A, Hackl M, Leschinger T, Wegmann K, Seybold D, Müller LP. Radial head fractures with interposed capitellar cartilage fragment-hindrance to bone healing-a case series. Arch Orthop Trauma Surg 2021;141:1615-24. [Google Scholar] [PubMed]
- 5. Massetti D, Marinelli M, Palmisani R, Coppa V, Gigante AP. Pediatric trans-olecranon fracture dislocation of the elbow associated with fracture of the radial head and with medial collateral ligament lesion: A case report and review of the literature. Trauma Case Rep 2021;32:100399. [Google Scholar] [PubMed]
- 6. Meyers AL, Marquart MJ. Pediatric Physeal Injuries Overview. Treasure Island, FL: StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/nbk560546/ [Last accessed on 15 March 2026]. [Google Scholar] [PubMed]
- 7. Iannuzzi NP, Leopold SS. In brief: The mason classification of radial head fractures. Clin Orthop Relat Res 2012;470:1799-802. [Google Scholar] [PubMed]
- 8. Kruppa C, Königshausen M, Schildhauer TA, Dudda M. Isolated pediatric radial head and neck fractures. A rare injury. Analysis and follow up of 19 patients. Injury 2015;46:S10-6. [Google Scholar] [PubMed]
- 9. Langenberg LC, Van Den Ende KI, Reijman M, Boersen GJ, Colaris JW. Pediatric radial neck fractures: A systematic review regarding the influence of fracture treatment on elbow function. Children (Basel) 2022;9:1049. [Google Scholar] [PubMed]
- 10. Zwingmann J, Welzel M, Dovi-Akue D, Schmal H, Südkamp NP, Strohm PC. Clinical results after different operative treatment methods of radial head and neck fractures. Injury Int J Care Injured 2013;44:1540-50. [Google Scholar] [PubMed]
- 11. Berdusco R, Louati H, Desloges W, Papp SR, Pollock JW. Lateral elbow exposures: The extensor digitorum communis split compared with the Kocher approach. JBJS Essent Surg Tech 2015;5:e30. [Google Scholar] [PubMed]
- 12. Jacob J, Isaac B. Anatomical considerations regarding the posterior interosseous nerve for surgical approaches in the proximal forearm: A cadaveric study. J Anat Soc India 2021;70:69-74. [Google Scholar] [PubMed]
- 13. Leung AG, Peterson HA. Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop 2000;20:7-14. [Google Scholar] [PubMed]
- 14. Macken AA, Eygendaal D, Van Bergen CJ. Diagnosis, treatment and complications of radial head and neck fractures in the pediatric patient. World J Orthop 2022;13:238-49. [Google Scholar] [PubMed]
- 15. Phadatare JP, Mankar S, Harkare VV, Sakhare RH, Thakkar HB. Radial head fracture (mason type 4) fixation with headless compression screws: The “tripod technique”. Cureus 2024;16:e67576. [Google Scholar] [PubMed]
- 16. He X, Fen Q, Yang J, Lei Y, Heng L, Zhang K. Risk factors of elbow stiffness after open reduction and internal fixation of the terrible triad of the elbow joint. Orthop Surg 2021;13:530-6. [Google Scholar] [PubMed]
- 17. Bašković M, Pešorda D, Zaninović L, Hasandić D, Vuga KL, Pogorelić Z. Management of pediatric elbow fractures and dislocations. Children 2024;11:906-6. [Google Scholar] [PubMed]
- 18. Nicholson LT, Skaggs DL. Proximal radius fractures in children. J Am Acad Orthop Surg 2019;27:e876-86. [Google Scholar] [PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Comparison of Radial Head Prosthesis versus Excision in Comminuted Radial Head Fractures: A Retrospective Comparative Study
June 1, 2026 Comparison of Radial Head Prosthesis versus Excision in Comminuted Radial Head Fractures: A Retrospective Comparative Study July 1, 2025 Pediatric Capitellum Fracture Fixation with Bio-absorbable K-wire
July 1, 2025 Pediatric Capitellum Fracture Fixation with Bio-absorbable K-wire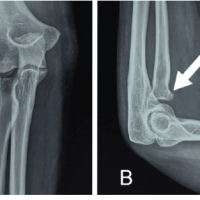 March 1, 2025 Functional Outcome of Radial Head Fracture Treated with Open Reduction Internal Fixation using Plating Versus Herbert Screw Fixation: A Case Series
March 1, 2025 Functional Outcome of Radial Head Fracture Treated with Open Reduction Internal Fixation using Plating Versus Herbert Screw Fixation: A Case Series October 1, 2024 Terrible Triad Injuries around the Elbow: It is Still a Puzzle? Prospective Study
October 1, 2024 Terrible Triad Injuries around the Elbow: It is Still a Puzzle? Prospective Study