
Atypical slipped capital femoral epiphysis in older adolescents should always raise suspicion for underlying endocrine disorders such as hypogonadism. Early surgical stabilization combined with appropriate hormonal therapy is essential to achieve normal physeal closure and excellent long-term functional outcomes.
Dr. Lavudi Rambabu, Department of Orthopaedics, All India Institute of Medical Sciences, Mangalagiri, Andhra Pradesh, India. Phone: +91-8790078123. E-mail: lavudiramchouhan@gmail.com
Abstract
Introduction: Slipped capital femoral epiphysis (SCFE) generally occurs during adolescence; however, atypical cases linked to endocrine dysfunctions such as hypogonadism are uncommon and require a multidisciplinary approach.
Case Report: A 17-year-old adolescent presented with a 2-week history of right hip pain and restricted mobility. He had a body mass index of 40 kg/m² and short stature (140 cm). Radiographs confirmed SCFE. Endocrine work-up revealed hypogonadism. Initial traction for 3 days was followed by closed reduction and internal fixation with cannulated cancellous screws. The patient was advised to be non-weight-bearing for 6 months. Concurrent hormonal therapy for hypogonadism resulted in improved skeletal maturation.
Result: At the 5-year follow-up, the physis had fused completely with excellent functional recovery.
Conclusion: Combined orthopaedic stabilisation and endocrine management can yield excellent long-term outcomes in atypical SCFE.
Keywords: Slipped capital femoral epiphysis, hypogonadism, endocrine disorder, cannulated screw fixation.
Slipped capital femoral epiphysis (SCFE) is characterized by displacement of the femoral head relative to the neck through the growth plate. While it most frequently affects adolescents during periods of rapid growth, atypical presentations are increasingly recognized in association with endocrine and metabolic disorders [1,2]. Endocrine abnormalities such as hypothyroidism, growth hormone imbalance, and hypogonadism can alter physeal biology, predisposing it to mechanical failure even under normal physiological loads [1]. Patients with atypical SCFE often present outside the usual age range, with short stature or delayed skeletal maturation, making clinical suspicion essential [2,3]. Hypogonadism, in particular, results in reduced sex steroid levels, which play a key role in skeletal development and physeal closure, thereby prolonging vulnerability of the growth plate [4].
A 17-year-old male presented with progressively worsening pain in the right hip for 2 weeks, associated with difficulty in ambulation. There was no preceding trauma. Clinical evaluation revealed:
- Short stature for age (<50th centile)
- High body mass index (40 kg/m2)
- Inability to walk
- Severe right hip tenderness
- Limb in external rotation
- Restricted internal rotation and abduction
- No neurovascular compromise
- Normal contralateral hip examination.
The patient exhibited delayed secondary sexual characteristics. Hormonal evaluation confirmed hypogonadism, suggesting an underlying endocrine aetiology for the atypical presentation. Radiographic assessment confirmed SCFE of the right hip. Left hip being normal (Fig. 1).

Figure 1: Anteroposterior radiograph of the pelvis with both hips showing widening of the proximal femoral physis and displacement of the epiphysis on the right side, consistent with slipped capital femoral epiphysis.
Treatment:
The patient was initially managed with analgesics and skin traction for 3 days to reduce discomfort and minimise further displacement. Meanwhile, medical treatment for hypogonadism was initiated. Definitive management included:
- Closed reduction under fluoroscopy (Fig. 2).
- Internal fixation using a cannulated cancellous screw (Fig. 3).

Figure 2: Frog-leg lateral view demonstrating posterior and inferior displacement of the capital femoral epiphysis relative to the metaphysis, confirming the diagnosis of slipped capital femoral epiphysis.

Figure 3: Immediate post-operative radiograph showing satisfactory reduction and fixation with a cannulated cancellous screw across the physis.
Post-operative protocol:
- Strict non-weight-bearing for 6 months due to the added risk of failure of fixation and probability of slip in the contralateral hip due to increased stress.
- Gradual progression to full weight-bearing.
Endocrinological treatment included testosterone replacement therapy, which facilitated improved skeletal maturation and eventual physeal closure at the 1-year follow-up (Fig. 4).

Figure 4: Radiograph at 1-year follow-up showing maintained alignment and progressive physeal healing without complications such as avascular necrosis or chondrolysis.
Outcome:
At 5-year follow-up:
- Radiographs demonstrated complete fusion of the physis (Fig. 5)
- No evidence of avascular necrosis or chondrolysis
- Full, painless range of motion
- Return to unrestricted daily activities.
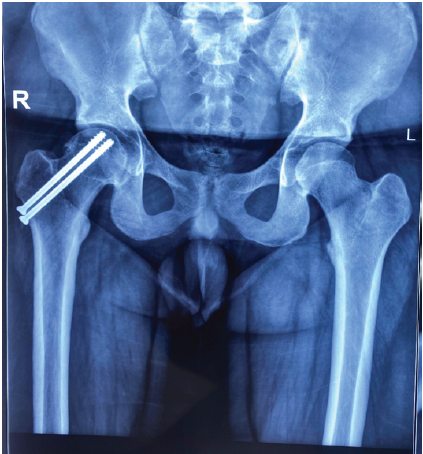
Figure 5: Radiograph at 5-year follow-up demonstrating complete physeal fusion with maintained femoral head alignment and no degenerative changes.
Such favourable outcomes are consistent with literature emphasising early stabilisation combined with systemic disease management [1,5].
SCFE is typically observed between 10 and 16 years of age; however, cases presenting outside this range should raise suspicion for underlying systemic pathology [1,3]. Atypical SCFE is frequently associated with endocrine disorders, and its reported prevalence ranges widely, though it remains relatively uncommon [1,3]. Several studies highlight the association between endocrine disorders and atypical SCFE:
- Loder et al. reported that endocrine disorders are present in up to 20% of atypical SCFE cases [6].
- Wells et al. emphasised delayed skeletal maturity in hypogonadal patients, leading to prolonged physeal vulnerability [7].
- Peck suggested routine endocrine screening in patients presenting with atypical features such as short stature or obesity [8].
Hormonal imbalances affect the structural integrity of the physis by altering chondrocyte maturation and extracellular matrix composition, thereby increasing susceptibility to shear forces [1,9]. Hypogonadism contributes to delayed epiphyseal closure due to deficiency of sex steroids, which are critical for skeletal maturation and bone health [4,10]. Obesity, as seen in this patient, further increases mechanical stress across the hip joint, compounding the risk of slip [9]. Management strategies consistently recommend:
- Early surgical stabilization
- Avoidance of aggressive manipulation
- Identification and treatment of underlying endocrine pathology.
Long-term outcomes are favourable when both orthopaedic and systemic conditions are addressed. Current evidence supports in situ fixation using cannulated screws as the preferred treatment modality due to its reliability and low complication rates [1,5]. Importantly, patients with atypical features such as short stature or endocrine abnormalities should undergo thorough hormonal evaluation [2,11]. Recent studies also highlight the role of metabolic and hormonal factors, including vitamin D and endocrine dysfunction, in influencing disease severity and progression [11]. Failure to recognise underlying endocrinopathy may result in delayed healing, bilateral involvement, or recurrence [2,9]. In the present case, timely orthopaedic stabilisation combined with hormonal therapy resulted in satisfactory physeal closure and excellent long-term functional recovery.
Atypical SCFE associated with hypogonadism requires a comprehensive approach integrating surgical stabilization and endocrine correction. Early diagnosis and multidisciplinary care can lead to excellent long-term outcomes.
Always evaluate for endocrine disorders in atypical SCFE. Combined orthopaedic and hormonal management is key to successful long-term outcomes.
References
- 1. Lindgren AM, Lieber AM, Shah SA, Thacker MM. Management of atypical slipped capital femoral epiphysis. J Pediatr Orthop Soc North Am 2024;5:727. [Google Scholar] [PubMed]
- 2. Shaw KA, Shiver AL, Oakes T, Fletcher ND. Slipped Capital Femoral Epiphysis Associated with Endocrinopathy: A Narrative Review. JBJS Rev. 2022 Feb 7;10(2). doi: 10.2106/JBJS.RVW.21.00188. PMID: 35130197. [Google Scholar] [PubMed] [CrossRef]
- 3. Lindgren AM, Lieber AM, Shah SA, Thacker MM. Management of Atypical Slipped Capital Femoral Epiphysis. J Pediatr Soc North Am. 2024 Feb 12;5(3):727. doi: 10.55275/JPOSNA-2023-727. PMID: 40433322; PMCID: PMC12088152. [Google Scholar] [PubMed] [CrossRef]
- 4. Dwyer AA, Quinton R. Editorial: New aspects in hypogonadism. Front Endocrinol 2020;11:426. [Google Scholar] [PubMed]
- 5. Sawicka-Gutaj N, Woźniak W, Naczk J, Pochylski M, Kruczyński J, Budny B, et al. Slipped capital femoral epiphysis in a 25-year-old hypogonadic man with a large cranial chondroma: Causality or coincidence? SCFE in hypogonadism case report. BMC Endocr Disord 2021;21:167. [Google Scholar] [PubMed]
- 6. Loder RT, Aronsson DD, Dobbs MB, Weinstein SL. Slipped capital femoral epiphysis. J Bone Joint Surg Am 2000;82:1170-88. [Google Scholar] [PubMed]
- 7. Wells D, King JD, Roe TF, Kaufman FR. Review of slipped capital femoral epiphysis associated with endocrine disease. J Pediatr Orthop 1993;13:610-4. [Google Scholar] [PubMed]
- 8. Peck DM. Slipped capital femoral epiphysis: Diagnosis and management. Am Fam Physician 2010;82:258-62. [Google Scholar] [PubMed]
- 9. Bellemore JM, Carpenter EC, Yu NY, Birke O, Little DG. Biomechanics of Slipped Capital Femoral Epiphysis: Evaluation of the Posterior Sloping Angle. Journal of Pediatric Orthopedics. 2016 Sep;36(6):651-655. DOI: 10.1097/bpo.0000000000000512. PMID: 25955168. [Google Scholar] [PubMed] [CrossRef]
- 10. De Silva NL, Papanikolaou N, Grossmann M, Antonio L, Quinton R, Anawalt BD, Jayasena CN. Male hypogonadism: pathogenesis, diagnosis, and management. Lancet Diabetes Endocrinol. 2024 Oct;12(10):761-774. doi: 10.1016/S2213-8587(24)00199-2. Epub 2024 Aug 16. PMID: 39159641. [Google Scholar] [PubMed] [CrossRef]
- 11. Ning P, Lin S, Geng H, Liu T. The role of vitamin D in slipped capital femoral epiphysis in children and adolescents: A retrospective case-control study. Front Endocrinol (Lausanne) 2025;15:1497103. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Delayed Slipped Capital Femoral Epiphysis Following Surgical Fixation of a Femoral Neck Fracture in a Child: A Rare Case Report
May 1, 2026 Delayed Slipped Capital Femoral Epiphysis Following Surgical Fixation of a Femoral Neck Fracture in a Child: A Rare Case Report April 1, 2026 Open Reduction and Treatment with Bone Morphogenetic Protein-2 for Correction of Closed Tibial Pseudoarthrosis in a 32-Year-Old Non-smoking Male with Osteoporosis and Hypogonadism: A Case Report
April 1, 2026 Open Reduction and Treatment with Bone Morphogenetic Protein-2 for Correction of Closed Tibial Pseudoarthrosis in a 32-Year-Old Non-smoking Male with Osteoporosis and Hypogonadism: A Case Report April 1, 2026 Pediatric Hip Pathology in Eastern India. A Cross-sectional Study on Types and Incidence
April 1, 2026 Pediatric Hip Pathology in Eastern India. A Cross-sectional Study on Types and Incidence October 1, 2025 Non-union of Talus Fracture in a 34-Year-Old Male Managed with Open Reduction and Internal Fixation Using Cancellous Cannulated Screws: A Case Report
October 1, 2025 Non-union of Talus Fracture in a 34-Year-Old Male Managed with Open Reduction and Internal Fixation Using Cancellous Cannulated Screws: A Case Report