
Painful cortical lytic lesions in children may not always represent osteoid osteoma, and non-ossifying fibroma should also be considered in atypical presentations requiring histopathological confirmation.
Dr. Kevin Lourdes, Department of Orthopedic Surgery, Sri Ramachandra Institute of Higher Education and Research, Porur, Chennai - 600116, Tamil Nadu, India. E-mail: kevinlourdes5@gmail.com
Abstract
Introduction: Non-ossifying fibroma (NOF) is a common benign fibrous lesion seen in children and adolescents and is usually asymptomatic. It is often found incidentally and most commonly involves the metaphyseal region of long bones. However, when the lesion arises from the cortical bone and presents with pain, it may clinically and radiologically mimic osteoid osteoma, leading to diagnostic confusion.
Case Report: An 8-year-old boy presented with severe pain in the right leg for 3 weeks. Radiographs revealed a cortical lytic lesion in the proximal tibial diaphysis, and magnetic resonance imaging findings were suggestive of osteoid osteoma. Due to persistent symptoms and diagnostic uncertainty, surgical curettage and saucerisation were performed. Histopathological examination revealed fibrocollagenous tissue composed of spindle-shaped cells arranged in a storiform pattern with scattered osteoclast-type multinucleated giant cells, confirming the diagnosis of NOF. Microbiological culture showed no growth.
Conclusion: Painful cortical lesions in children can mimic osteoid osteoma both clinically and radiologically. Histopathological examination is essential for definitive diagnosis in atypical presentations. This case highlights the importance of considering NOF in the differential diagnosis of painful cortical lesions in children.
Keywords: Non-ossifying fibroma, osteoid osteoma, cortical lesion, proximal tibia, pediatric bone lesion, histopathology, diagnostic dilemma.
Non-ossifying fibroma (NOF) is one of the most frequently encountered benign fibrous lesions of bone in children and adolescents. It commonly occurs in the metaphyseal region of long bones, particularly around the knee joint, including the distal femur and proximal tibia. These lesions are generally asymptomatic and are often detected incidentally during radiographic evaluation performed for unrelated reasons [1,2]. NOF is considered a developmental bone defect rather than a true neoplasm and typically resolves spontaneously with skeletal maturity [2,3,4]. Osteoid osteoma, in contrast, is a benign osteoblastic tumour that commonly affects children and young adults. It is characterised by localised pain, often worse at night, and classically relieved by non-steroidal anti-inflammatory drugs [5,6]. Radiologically, osteoid osteoma presents as a small radiolucent nidus surrounded by varying degrees of reactive sclerosis [5,6]. When a NOF occurs in an unusual location, such as the diaphyseal cortex and presents with pain, it may resemble osteoid osteoma both clinically and on imaging [5,7]. Such atypical presentations may create diagnostic uncertainty, and histopathological examination may be required for confirmation. This report describes a rare case of cortical NOF of the proximal tibial diaphysis in a child that was initially suspected to be osteoid osteoma.
An 8-year-old boy presented with complaints of severe pain in the right leg for a duration of 3 weeks. The pain was localised to the upper part of the leg and was associated with marked tenderness over the proximal diaphyseal region of the tibia on clinical examination. A history of intermittent fever episodes 2 weeks before presentation was present, and a viral fever 3 years back. There was no history of trauma, night cries, or weight loss. Plain radiographs of the right leg showed a well-defined cortical lytic lesion on the medial aspect of the proximal tibial diaphysis with surrounding sclerosis (Fig. 1).

Figure 1: Anteroposterior radiograph of the right leg showing cortical lytic lesion in medial aspect of proximal diaphysis of tibia.
Based on the clinical presentation and radiographic findings, a provisional diagnosis of osteoid osteoma was considered, with subacute osteomyelitis as a primary differential diagnosis. Magnetic resonance imaging demonstrated an approximately 0.5 × 0.4 × 2 cm (anteroposterior × transverse × craniocaudal) cortical lesion with surrounding marrow oedema and cortical thickening (Fig. 2).
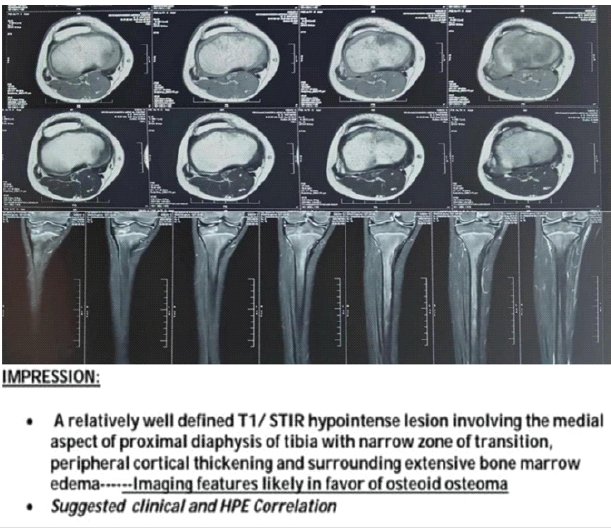
Figure 2: Magnetic resonance imaging of the right leg showing hypointense lesion in medial aspect of proximal diaphysis with narrow zone of transition, peripheral cortical thickening.
Due to persistent severe pain and diagnostic uncertainty, surgical intervention was planned. The lesion was approached through a longitudinal incision over the medial aspect of the proximal tibia under fluoroscopic guidance. Intraoperatively, a cortical lytic lesion with surrounding sclerosis was identified. Curettage and saucerisation of the lesion were performed (Fig. 3), and the tissue was sent for histopathological examination and microbiological culture.

Figure 3: Intraoperative image showing post-curettage and saucerization status.
Postoperatively, an X-ray was taken (Fig. 4), and the patient was advised non-weight-bearing mobilisation with walker support to avoid postoperative cortical stress and possible pathological fracture.
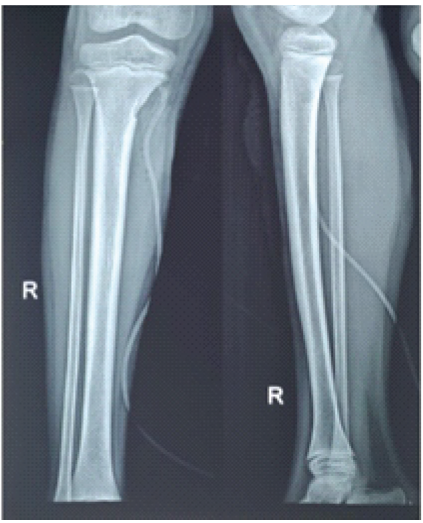
Figure 4: Immediate post-operative radiograph showing curettage of the lesion.
Weight-bearing was then increased gradually as tolerated. The culture report showed no bacterial growth. Histopathological examination revealed fibrocollagenous tissue composed of spindle-shaped cells arranged in a storiform pattern (Fig. 5) with scattered osteoclast-type multinucleated giant cells (Fig. 6).
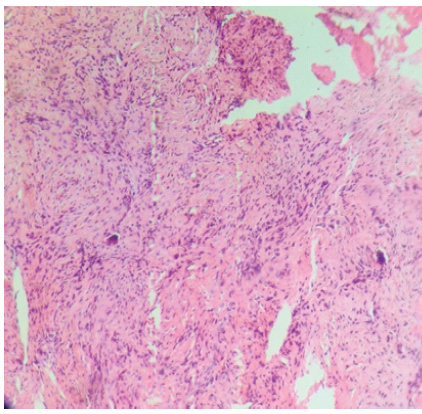
Figure 5: Histopathological examination slide showing bland spindle cells arranged in storiform pattern suggestive of non-ossifying fibroma.
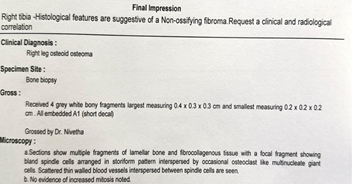
Figure 6: Histopathological examination report suggestive of non-ossifying fibroma.
These findings were consistent with NOF. On serial follow-up over 1 year, the patient remained symptomatically improved with no clinical or radiological evidence of recurrence. The child was able to resume routine activities and sports without post-operative morbidity or functional impairment.
NOF is a benign fibrous lesion that usually occurs in the metaphyseal region of long bones in skeletally immature individuals. Most lesions are asymptomatic and discovered incidentally [1,2]. However, lesions may become symptomatic when they are large, involve a significant portion of the cortex, or occur in atypical locations such as the diaphysis [2,3,4]. In the present case, the lesion was located in the cortical region of the proximal tibial diaphysis, which is an uncommon location for NOF but a relatively common location for osteoid osteoma [5,6]. The presence of severe localised pain and a cortical lytic lesion with surrounding sclerosis on imaging led to an initial diagnosis of osteoid osteoma. Differential diagnoses such as eosinophilic granuloma, stress fracture, subacute osteomyelitis, osteoblastoma, and malignant cortical lesions were considered. However, eosinophilic granuloma was considered less likely due to the absence of systemic manifestations and normal laboratory parameters. Stress fracture was unlikely because there was no history of significant trauma or repetitive stress activity. Malignant lesions were considered less probable in view of the absence of constitutional symptoms such as loss of appetite, weight loss, or persistent fever. Radiographically, osteoid osteoma typically presents as a small radiolucent nidus surrounded by dense reactive sclerosis. Brodie’s abscess, a form of subacute osteomyelitis, may also present as a lytic lesion with surrounding sclerosis and can be associated with localised pain [5,8]. In the present case, magnetic resonance imaging revealed cortical thickening, marrow oedema, and adjacent reactive changes that were not specific to a single pathology and could be encountered in osteoid osteoma and subacute osteomyelitis, as well as other cortical bone lesions. Computed tomography (CT) was not done in this case, as subacute osteomyelitis and low-grade infection were part of the initial differential diagnosis, prompting preference for magnetic resonance imaging to assess marrow oedema, soft-tissue reaction, and possible inflammatory changes. While CT could have provided improved visualisation of a cortical nidus suggestive of osteoid osteoma, the final diagnosis was confirmed through histopathological examination [7,9]. As the overall clinical suspicion for infection remained low and routine microbiological studies did not reveal any organism growth, further molecular investigations and extended infectious workup were not considered necessary. In addition, the combined clinical and imaging features were felt to be more consistent with a benign cortical bone lesion than an active indolent infection. After radiological assessment, an open biopsy combined with curettage and debridement was chosen instead of CT-guided biopsy, as it provided sufficient tissue for histopathological evaluation, facilitated exclusion of infection, and enabled concurrent treatment of the lesion in view of ongoing pain and diagnostic ambiguity. Histopathological examination plays a crucial role in differentiating these lesions. NOF shows spindle-shaped fibroblasts arranged in a storiform pattern with multinucleated giant cells and fibrocollagenous stroma. In contrast, osteoid osteoma shows a nidus composed of osteoid and woven bone lined by osteoblasts in a vascular stroma [1,5]. In the present case, histopathological findings confirmed the diagnosis of NOF, and microbiological culture ruled out infection. Although observation is the standard approach for most NOFs, conservative treatment was not adequate in the present case because the patient continued to experience persistent severe pain even after a 3-week period of non-operative management. Furthermore, the unusual cortical diaphyseal location and unresolved diagnostic uncertainty favoured surgical exploration with biopsy [2,10]. This case demonstrates that NOF can present as a painful cortical lesion and may mimic osteoid osteoma clinically and radiologically, thereby creating a diagnostic conundrum.
Limitations:
As a single-case report of cortical NOF involving the proximal tibial diaphysis in a child, this study has limited general applicability. In addition, the uncommon cortical diaphyseal presentation makes it difficult to derive standardised diagnostic and treatment recommendations from an isolated case. Standardised functional outcome measures and pain scoring systems were not formally documented during the preoperative and postoperative periods.
Cortical NOF of the tibial diaphysis is a rare presentation and can mimic osteoid osteoma clinically and radiologically. Histopathological examination is essential for definitive diagnosis in atypical cases. Symptomatic lesions can be managed successfully with curettage and follow-up.
Painful cortical lesions involving the proximal diaphysis of the tibia in children are commonly presumed to be osteoid osteomas due to their typical clinical presentation of localised pain, often worse at night and relieved by non-steroidal anti-inflammatory drugs. However, not all painful cortical lesions represent osteoid osteoma. Several benign and malignant conditions can mimic osteoid osteoma clinically and radiologically, making accurate diagnosis challenging. Therefore, histopathological confirmation becomes essential when imaging findings are atypical or when clinical features do not perfectly match osteoid osteoma.
References
- 1. De Salvo S, Pavone V, Coco S, Dell’Agli E, Blatti C, Testa G. Benign bone tumors: An overview of what we know today. J Clin Med 2022;11:699. [Google Scholar] [PubMed]
- 2. Herget GW, Mauer D, Krauß T, El Tayeh A, Uhl M, Südkamp NP, et al. Non-ossifying fibroma: Natural history with an emphasis on a stage-related growth, fracture risk and the need for follow-up. BMC Musculoskelet Disord 2016;17:147. [Google Scholar] [PubMed]
- 3. Fritzsche H, Schaser KD, Hofbauer C. Benigne Tumoren und tumorähnliche läsionen des knochens: Allgemeine behandlungsprinzipien [Benign tumours and tumour-like lesions of the bone: General treatment principles]. Orthopade 2017;46:484-97. [Google Scholar] [PubMed]
- 4. Ritschl P, Karnel F, Hajek P. Fibrous metaphyseal defects–determination of their origin and natural history using a radiomorphological study. Skeletal Radiol 1988;17:8-15. [Google Scholar] [PubMed]
- 5. Kransdorf MJ, Stull MA, Gilkey FW, Moser RP. Osteoid osteoma. Radiographics 1991;11:671-96. [Google Scholar] [PubMed]
- 6. Greenspan A. Benign bone-forming lesions: Osteoma, osteoid osteoma, and osteoblastoma. Clinical, imaging, pathologic, and differential considerations. Skeletal Radiol 1993;22:485-500. [Google Scholar] [PubMed]
- 7. Carneiro BC, Da Cruz IA, Ormond Filho AG, Silva IP, Guimarães JB, Silva FD, et al. Osteoid osteoma: The great mimicker. Insights Imaging 2021;12:32. [Google Scholar] [PubMed]
- 8. Roberts JM, Drummond DS, Breed AL, Chesney J. Subacute hematogenous osteomyelitis in children: A retrospective study. J Pediatr Orthop 1982;2:209-14. [Google Scholar] [PubMed]
- 9. Matcuk GR Jr., Waldman LE, Fields BK, Colangeli M, Palmas M, Righi A, et al. Conventional radiography for the assessment of focal bone lesions of the appendicular skeleton: Fundamental concepts in the modern imaging era. Skeletal Radiol 2025;54:1391-406. [Google Scholar] [PubMed]
- 10. Campanacci M, Ruggieri P, Gasbarrini A, Ferraro A, Campanacci L. Osteoid osteoma. Direct visual identification and intralesional excision of the nidus with minimal removal of bone. J Bone Joint Surg Br 1999;81:814-20. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 O-arm Navigation-assisted Excision of Cervical Osteoid Osteoma Adjacent to the Vertebral Artery: Technical Note and Case Report
August 1, 2026 O-arm Navigation-assisted Excision of Cervical Osteoid Osteoma Adjacent to the Vertebral Artery: Technical Note and Case Report August 1, 2026 Understanding Diagnostic Challenges in Ewing Sarcoma – A Report of Two Cases
August 1, 2026 Understanding Diagnostic Challenges in Ewing Sarcoma – A Report of Two Cases July 1, 2026 Diagnostic Dilemma in a Distal Femoral Intramedullary Lesion: Enchondroma Mimicking Low-Grade Chondrosarcoma with Discordant Biopsy Findings: A Case Report
July 1, 2026 Diagnostic Dilemma in a Distal Femoral Intramedullary Lesion: Enchondroma Mimicking Low-Grade Chondrosarcoma with Discordant Biopsy Findings: A Case Report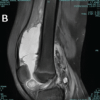 July 1, 2026 Post-traumatic Hemosiderotic Synovitis Mimicking Pigmented Villonodular Synovitis in a Non-hemophilic Child: First Reported Case from the United Arab Emirates
July 1, 2026 Post-traumatic Hemosiderotic Synovitis Mimicking Pigmented Villonodular Synovitis in a Non-hemophilic Child: First Reported Case from the United Arab Emirates