
Repeated cultures and careful reimplantation timing are important when a hip replacement infection recurs with different organisms over time.
Dr. Saketh K Kamaraju, Central Michigan University College of Medicine, Saginaw, Michigan, United States. E-mail: kamar1s@cmich.edu
Abstract
Introduction: Periprosthetic joint infection after total hip arthroplasty is uncommon but morbid. Reports usually focus on a single organism or a persistent recurrent infection. This case is important because it describes sequential infections with four distinct and therapeutically challenging organisms in the same arthroplasty, illustrating how management must be repeatedly re-evaluated rather than anchored to the initial culture result.
Case Report: A 62-year-old woman with hypertension, chronic anaemia, and a history of methicillin-resistant Staphylococcus aureus infection underwent robotic-assisted left total hip arthroplasty. Her ethnic background was not available in the deidentified record. Over 16 months, she developed four culture-confirmed periprosthetic joint infections caused by Pseudomonas aeruginosa, Candida glabrata, methicillin-resistant S. aureus, and Serratia marcescens. Each episode was managed with repeat culture acquisition before antimicrobial therapy, surgical debridement with spacer exchange when indicated, and organism-directed antimicrobial or antifungal treatment. Definitive reimplantation was delayed until the wound was healed, inflammatory markers had normalised, and repeat aspiration after an antimicrobial-free interval was negative. At 9 months after reimplantation, she remained free of recurrent infection and was improving with physical therapy. The patient did not have diabetes mellitus, and her serology status was negative. No patient-specific clinical wound photographs or intraoperative photographs were available for publication. The available operative descriptions note debridement through the prior incision with removal of infected tissue and placement or exchange of a temporary antibiotic-loaded cement hip spacer. Available susceptibility reports showed that the P. aeruginosa isolate was susceptible to all tested antipseudomonal agents, the methicillin-resistant S. aureus isolate was susceptible to vancomycin, and the S. marcescens isolate was reported as multidrug-resistant and carbapenem-resistant but remained susceptible to cefepime. The C. glabrata report confirmed organism growth, but an antifungal susceptibility panel was not available in the provided report.
Conclusion: This case emphasises that recurrent hip periprosthetic joint infection during staged management should be treated as a new diagnostic event until proven otherwise. Repeated cultures, multidisciplinary antimicrobial selection, and individualised timing of reimplantation may improve decision-making in complex sequential infections and may be useful to orthopaedic surgeons managing difficult revision arthroplasty cases.
Keywords: Total hip arthroplasty, periprosthetic joint infection, staged revision, Candida glabrata, culture-guided reimplantation.
Periprosthetic joint infection remains one of the most serious complications after total hip arthroplasty [1]. Although contemporary diagnostic frameworks, including International Consensus Meeting criteria and Infectious Diseases Society of America guidance, have improved evaluation and treatment, clinical decision-making remains difficult when infection is chronic, resistant, polymicrobial, or recurrent [2,3]. Staphylococci remain the predominant organisms in total hip arthroplasty infection, but Gram-negative bacilli account for a clinically important subset and may be associated with antimicrobial resistance patterns that limit standard therapy [4]. Pseudomonas aeruginosa is difficult to eradicate and has variable outcomes across debridement, antibiotics, implant retention, and component-exchange strategies [5,6]. Serratia marcescens is much less common, with most available literature limited to isolated cases or small reviews [7,8]. Fungal periprosthetic joint infection is also uncommon. Candida species represent a small subset, and Candida glabrata is particularly challenging because of reduced azole susceptibility. Current guidance generally supports prosthesis removal, staged revision when appropriate, and prolonged antifungal therapy [9,10]. Methicillin-resistant Staphylococcus aureus is another difficult pathogen in arthroplasty infection and is associated with increased risk of treatment failure [11,12,13]. We report a rare case of sequential, culture-confirmed infections with P. aeruginosa, C. glabrata, methicillin-resistant S. aureus, and S. marcescens after a single total hip arthroplasty.
A 62-year-old woman with hypertension, chronic anaemia, and a prior methicillin-resistant S. aureus infection underwent robotic-assisted left total hip arthroplasty without immediate complications. Ethnic background was not available in the deidentified record. She did not have diabetes mellitus, and her serology status was negative. Two months postoperatively, she developed worsening hip pain, swelling, and localised warmth. Blood cultures and joint aspiration grew P. aeruginosa. Through the original incision, all components were removed, extensive debridement was performed, multiple deep tissue samples were obtained before antibiotic administration, and an antibiotic-loaded cement spacer was placed. She received 3 weeks of intravenous (IV) antipseudomonal beta-lactam therapy followed by 12 weeks of oral ciprofloxacin based on susceptibility testing. The P. aeruginosa isolate was susceptible to all tested agents on the provided panel, including cefepime, ceftazidime, ciprofloxacin, meropenem, piperacillin-tazobactam, and aminoglycosides (Table 1).
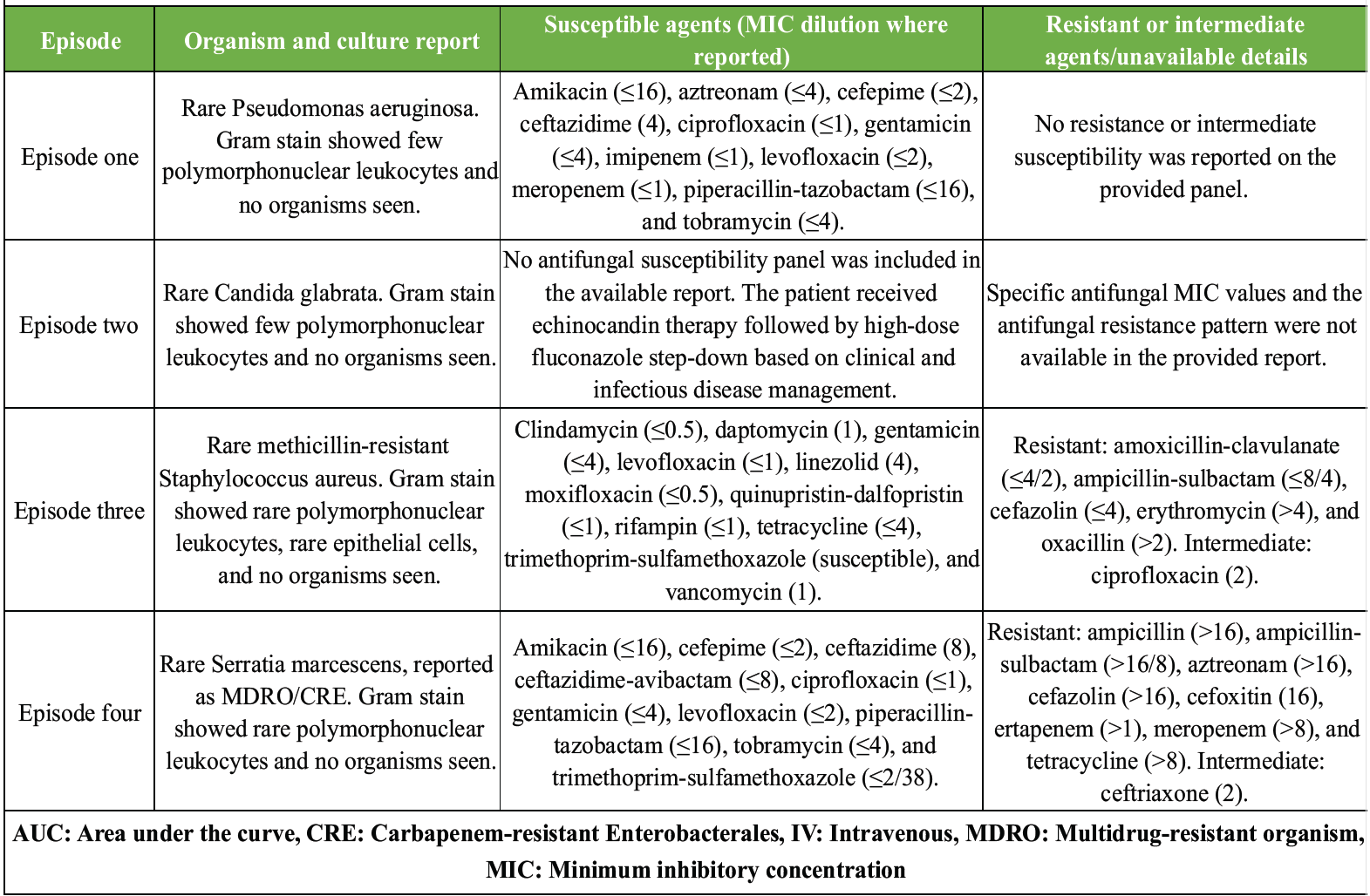
Table 1: Culture and susceptibility results by infection episode. This table summarizes the available culture reports, Gram stain findings, antimicrobial susceptibility interpretations, and visible minimum inhibitory concentration values. For Candida glabrata, the available report confirmed growth but did not include an antifungal susceptibility panel.
After an approximately 2-week antibiotic-free interval, repeat aspiration was performed. At 4 months, persistent concern for infection led to spacer exchange rather than reimplantation. Approximately 3 months later, she again developed hip pain and swelling. Aspiration and intraoperative cultures grew C. glabrata. Repeat debridement and spacer exchange were performed after cultures were obtained. She completed 6 weeks of echinocandin therapy followed by high-dose fluconazole. Reimplantation was again deferred because of ongoing concern for infection. The available C. glabrata report confirmed rare growth, but it did not include an antifungal susceptibility panel (Table 1). Because no formal antifungal susceptibility panel was included in the available C. glabrata report, antifungal treatment was selected under infectious disease guidance, using echinocandin therapy followed by high-dose fluconazole step-down; complete antifungal minimum inhibitory concentration (MIC) data were not available in the deidentified record. One month later, recurrent symptoms prompted repeat evaluation, and cultures yielded methicillin-resistant S. aureus. She underwent repeat debridement with spacer exchange, with multiple deep cultures obtained before antibiotics. She completed 6 weeks of IV vancomycin using area-under-the-curve-guided dosing. Rifampin was considered after wound stabilisation. The interstage plan again included protected weight-bearing, multidisciplinary follow-up, an antibiotic-free interval, and repeat aspiration. The methicillin-resistant S. aureus susceptibility report showed resistance to oxacillin, erythromycin, cefazolin, amoxicillin-clavulanate, and ampicillin-sulbactam, intermediate susceptibility to ciprofloxacin, and susceptibility to vancomycin, daptomycin, linezolid, rifampin, trimethoprim-sulfamethoxazole, clindamycin, gentamicin, levofloxacin, moxifloxacin, quinupristin-dalfopristin, and tetracycline (Table 1). Approximately 4 months later, she experienced a fourth recurrence, and cultures grew S. marcescens. Management again included debridement through the existing incision, spacer exchange, and culture-directed antimicrobial therapy. She received 6 weeks of IV cefepime, followed by an antimicrobial-free interval and repeat aspiration. The S. marcescens isolate was reported as a multidrug-resistant organism and a carbapenem-resistant Enterobacterales. It was resistant to multiple agents, including ertapenem and meropenem, but remained susceptible to cefepime, ceftazidime, ceftazidime-avibactam, ciprofloxacin, piperacillin-tazobactam, aminoglycosides, levofloxacin, and trimethoprim-sulfamethoxazole (Table 1). After approximately 4 months of negative cultures, a well-healed wound, and normalised inflammatory markers, definitive reimplantation was performed. At 9 months after reimplantation, there was no evidence of recurrent infection, and the patient was regaining function with physical therapy. The susceptibility results are summarised in Table 1, and the sequential management decisions are summarised in Table 2 and Fig. 1.
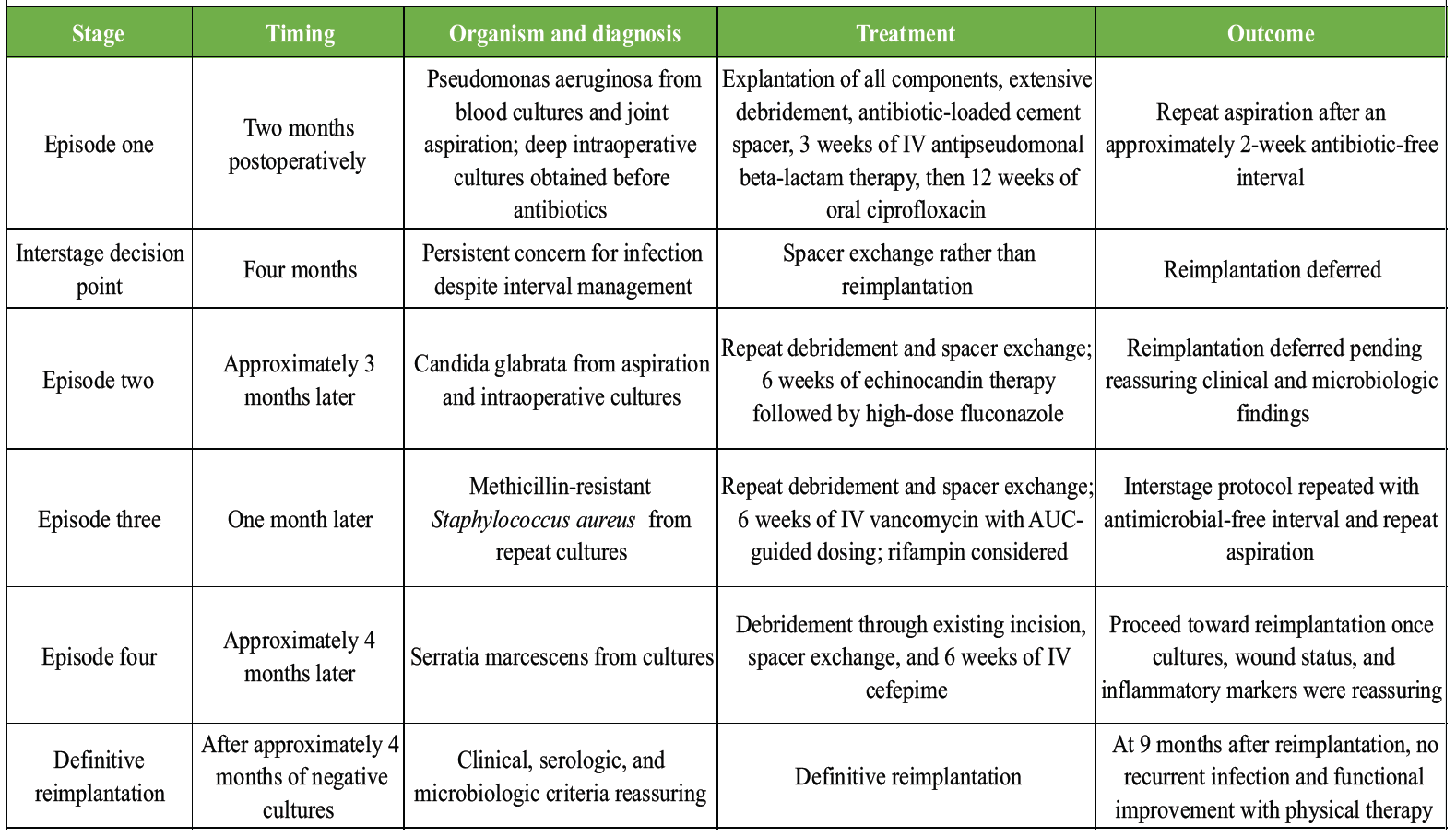
Table 2: Sequential infection episodes after left total hip arthroplasty. This table summarizes the timing, culture-confirmed organism, diagnostic method, treatment, and outcome during staged management. Definitive reimplantation was performed once cultures remained negative, the wound had healed, inflammatory markers had normalized, and aspiration after an antibiotic-free interval was reassuring. No patient-specific clinical or intraoperative photographs were available; operative records described use of a temporary antibiotic-loaded cement hip spacer.
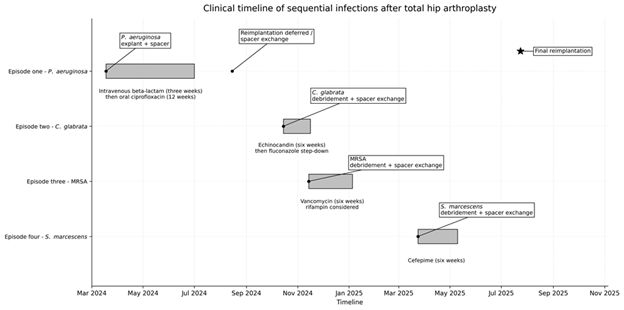
Figure 1: Timeline of sequential infections. Clinical timeline of four culture-confirmed periprosthetic joint infections after left total hip arthroplasty. Dots mark culture confirmation, shaded bars show organism-directed therapy, and the star marks final reimplantation. Reimplantation was deferred at the 4-month review because of persistent concern for infection.
A PubMed-focused literature review was performed using combinations of the following keywords: total hip arthroplasty, periprosthetic joint infection, staged revision, P. aeruginosa, C. glabrata, methicillin-resistant S. aureus, S. marcescens, spacer exchange, and reimplantation. The available literature describes these pathogens individually in prosthetic joint infection, but the sequential emergence of four distinct pathogens in the same hip arthroplasty is rarely represented. This makes the case educational because each recurrence required a fresh diagnostic and therapeutic approach rather than simply extending the prior treatment plan. Given the complexity of this case, the available culture and susceptibility information is summarised in Table 1. The bacterial reports allow reporting of sensitive, resistant, and intermediate interpretations with MIC dilutions where visible in the available reports. The only remaining missing susceptibility detail is the antifungal susceptibility panel for C. glabrata, which was not included in the provided report. The Gram-negative episodes contributed substantially to management complexity. In chronic P. aeruginosa prosthetic joint infection, revision with component exchange has been associated with higher success than debridement, antibiotics, and implant retention in many settings, and prolonged targeted therapy remains important [5,6,14]. Oral fluoroquinolone therapy is generally most appropriate when susceptibility is confirmed. S. marcescens prosthetic joint infection is uncommon, but reported cases emphasise the importance of adequate debridement and organism-directed antimicrobial therapy [7,8]. The identification of C. glabrata required a major change in strategy. Because this organism may have reduced azole susceptibility, guidelines favour prosthesis removal and prolonged antifungal therapy, often beginning with an echinocandin and transitioning to fluconazole only when susceptibility and clinical response support that approach [9,10,15]. In this patient, repeat deep cultures were prioritised before treatment changes, and reimplantation was deferred until clinical, serologic, and microbiologic parameters were reassuring. When methicillin-resistant S. aureus was isolated, vancomycin was administered with area-under-the-curve-guided dosing to balance efficacy and nephrotoxicity risk [16]. Rifampin was considered because of its activity against staphylococcal biofilm, but its role must be individualised, particularly because available evidence is mixed and may depend on the surgical strategy used [12,13,17]. The central lesson from this case is that recurrent infection during staged arthroplasty management should not be assumed to represent persistence of the original organism. Repeat cultures changed management at each episode. Similarly, reimplantation was not performed according to a fixed timeline; it was delayed until the wound was quiet, inflammatory markers had normalised, and aspiration after an antimicrobial-free interval was negative. This approach is consistent with guidance emphasising clinical judgement and microbiologic confirmation before reimplantation [3,18,19]. This case report is limited by its single-patient design and short-term follow-up after final reimplantation. The sequential emergence of distinct organisms may reflect host factors, prior antimicrobial exposure, healthcare-related exposure, or other variables that cannot be fully separated in a case report. Nonetheless, the case provides a practical example of culture-driven decision-making in a rare and complex periprosthetic hip infection. Additional limitations include the absence of patient-specific clinical or intraoperative photographs and the lack of an antifungal susceptibility panel for the C. glabrata isolate in the provided report. The bacterial susceptibility reports were available and are summarised in Table 1, but interpretation remains limited by the single-patient design and the retrospective nature of the case report.
Sequential periprosthetic hip infections can disrupt standard staged-revision pathways when new pathogens emerge between procedures. This case highlights the importance of repeated culture acquisition, organism-directed antimicrobial therapy, thorough debridement with spacer exchange when indicated, and individualised reimplantation timing. For orthopaedic surgeons and infection specialists, the case reinforces that each recurrence should be treated as a new diagnostic event until culture data prove otherwise.
In recurrent or staged hip periprosthetic joint infection, a new positive culture should not be assumed to represent persistence of the original organism. Re-culturing, targeted therapy, and individualised reimplantation timing are essential when sequential pathogens emerge.
References
- 1. Patel R. Periprosthetic joint infection. N Engl J Med 2023;388:251-62. [Google Scholar] [PubMed]
- 2. Sebastian S, Van Kueck M, Moriarty TF, Berbari EF. Diagnostic guidelines for periprosthetic joint infection: Know the differences. J Arthroplasty 2025;40:S83-6. [Google Scholar] [PubMed]
- 3. Osmon DR, Berbari EF, Berendt AR, Lew D, Zimmerli W, Steckelberg JM, et al. Diagnosis and management of prosthetic joint infection: Clinical practice guidelines by the infectious diseases society of America. Clin Infect Dis 2013;56:e1-25. [Google Scholar] [PubMed]
- 4. Hanssen JL, Van Der Wal RJ, Mahdad R, Keizer S, Delfos NM, Van Der Lugt JC, et al. Targeted antimicrobial regimens for Gram-negative prosthetic joint infections: A prospective multicenter study. Antimicrob Agents Chemother 2024;68:e0123224. [Google Scholar] [PubMed]
- 5. Prie H, Meyssonnier V, Kerroumi Y, Heym B, Lidove O, Marmor S, et al. Pseudomonas aeruginosa prosthetic joint-infection outcomes: Prospective, observational study on 43 patients. Front Med (Lausanne) 2022;9:1039596. [Google Scholar] [PubMed]
- 6. Kim BI, Schwartz AM, Wixted CM, Prado IP, Polascik BA, Seidelman JL, et al. Outcomes after Pseudomonas prosthetic joint infections. J Am Acad Orthop Surg 2024;32:e489-502. [Google Scholar] [PubMed]
- 7. Karczewski D, Skowronski J, Wasilewska A. Serratia marcescens prosthetic joint infection: Two case reports and a review of the literature. J Med Case Rep 2023;17:226. [Google Scholar] [PubMed]
- 8. Cannon TA, Norman P, Bearcroft P. Successfully treated multiresistant Serratia marcescens prosthetic hip joint infection: Case report. Ann R Coll Surg Engl 2014;96:e8-10. [Google Scholar] [PubMed]
- 9. Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the infectious diseases society of America. Clin Infect Dis 2016;62:e1-50. [Google Scholar] [PubMed]
- 10. Cobo F, Rodriguez-Granger J, Sampedro A, Aliaga-Martinez L, Navarro-Mari JM. Candida prosthetic joint infection: A review of treatment methods. Int J Environ Res Public Health 2017;14:535. [Google Scholar] [PubMed]
- 11. Salgado CD, Dash S, Cantey JR, Marculescu CE. Higher risk of failure of methicillin-resistant Staphylococcus aureus prosthetic joint infections. Clin Infect Dis 2007;45:469-76. [Google Scholar] [PubMed]
- 12. Zimmerli W, Sendi P. Role of rifampin against staphylococcal biofilm infections in vitro, in animal models, and in orthopedic device-related infections. Antimicrob Agents Chemother 2019;63:e01746-18. [Google Scholar] [PubMed]
- 13. Scheper H, De Greeff SC, Schreurs BW, Hoekstra H. Outcome of debridement, antibiotics, and implant retention for staphylococcal prosthetic joint infection: The role of rifampicin. Open Forum Infect Dis 2021;8:ofab298. [Google Scholar] [PubMed]
- 14. Shah NB, Osmon DR, Steckelberg JM, Sierra RJ, Walker RC, Tande AJ, et al. Pseudomonas prosthetic joint infections: A review of 102 episodes. J Bone Joint Infect 2016;1:25-30. [Google Scholar] [PubMed]
- 15. Escola-Verge L, Munoz-Pons H, Corona PS, Pigrau C. Candida periprosthetic joint infection: Is it curable? Antibiotics (Basel) 2021;10:458. [Google Scholar] [PubMed]
- 16. Rybak MJ, Le J, Lodise TP, Levine DP, Bradley JS, Liu C, et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: A revised consensus guideline and review by the American society of health-system pharmacists, the infectious diseases society of America, the pediatric infectious diseases society, and the society of infectious diseases pharmacists. Am J Health Syst Pharm 2020;77:835-64. [Google Scholar] [PubMed]
- 17. Karlsen OE, Borgen P, Bragnes B, Figved W, Grogaard B, Rydinge J, et al. Rifampin combination therapy in staphylococcal prosthetic joint infections: A randomized controlled trial. J Orthop Surg Res 2020;15:365. [Google Scholar] [PubMed]
- 18. Aalirezaie A, Bauer TW, Fayaz H, Griffin W, Higuera CA, Krenn V, et al. Hip and knee section, diagnosis, reimplantation: Proceedings of international consensus on orthopedic infections. J Arthroplasty 2019;34:S369-79. [Google Scholar] [PubMed]
- 19. Tsikopoulos K, Sidiropoulos K. Is there sufficient evidence to support the use of antibiotic holiday just before the second stage of an infected total hip or knee arthroplasty revision surgery? World J Orthop 2024;15:483-5. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Revision of a Dislocated Articulating Antibiotic Hip Spacer as an Alternative to Girdlestone Arthroplasty: A Case Report
June 1, 2026 Revision of a Dislocated Articulating Antibiotic Hip Spacer as an Alternative to Girdlestone Arthroplasty: A Case Report January 1, 2025 A Rare Case of Staphylococcus Caprae Periprosthetic Hip Infection with Unusual Clinical Presentation
January 1, 2025 A Rare Case of Staphylococcus Caprae Periprosthetic Hip Infection with Unusual Clinical Presentation September 1, 2024 Case Reports: Periprosthetic Joint Infection after Total Joint Arthroplasty Following Swimming Activity
September 1, 2024 Case Reports: Periprosthetic Joint Infection after Total Joint Arthroplasty Following Swimming Activity August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report
August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report