
Neglected zone VII extensor tendon injuries associated with large tendon gaps can be successfully reconstructed using a fascia lata autograft when meticulous surgical technique is combined with structured rehabilitation. Awareness of the juncturae tendinum is essential during clinical assessment.
Dr. B Nellaiyappan, Department of Hand Surgery, Sri Ramachandra Institute of Higher Education and Research, Porur, Chennai - 600116, Tamil Nadu, India. E-mail: drvenkatesh_11@hotmail.com
Abstract
Introduction: Extensor tendon injuries of the hand are frequently encountered owing to their superficial anatomical position and inadequate soft tissue protection [1][1.1]. When such injuries are neglected, particularly at the level of zone VII, they present substantial reconstructive challenges due to tendon retraction, fibrosis, adhesion formation, and increased tendon gaps. Multiple reconstructive strategies have been described in the literature, with tendon grafting being a dependable option in delayed presentations [2].
Case Report: We describe a case of a 2-month-old neglected zone VII extensor tendon injury of the right hand following a glass-cut trauma. The patient presented with an inability to actively extend the index and middle fingers. Intraoperatively, complete transection of the extensor digitorum communis (EDC) and extensor indicis proprius tendons of the index finger, complete transection of the EDC tendon of the middle finger, and partial transection of the EDC tendon of the ring finger were identified, with an approximate 11 cm tendon gap. Reconstruction was achieved using a fascia lata autograft to bridge the defect. Postoperative care included brief immobilisation followed by early controlled mobilisation, resulting in satisfactory functional recovery.
Conclusion: Reconstruction using a fascia lata autograft represents a reliable and effective method for managing neglected multiple extensor tendon injuries in zone VII. The presence of juncturae tendinum may clinically obscure complete tendon disruption. Even within a short duration after injury, the tendon may not be amenable to primary repair and may require grafting. Structured early rehabilitation remains critical for achieving optimal functional outcomes [3].
Keywords: Extensor tendon injury, zone VII, neglected tendon injury, fascia lata autograft, tendon reconstruction.
Injuries involving the extensor tendons of the hand are commonly encountered in clinical practice due to their superficial location and thin protective soft tissue envelope [1]. Kleinert and Verdan classified extensor tendon injuries into eight anatomical zones, with odd-numbered zones corresponding to joint levels starting from the distal interphalangeal joint and even-numbered zones located between joints, progressing from distal to proximal [2-4]. This was later expanded to nine zones, with zone VIII being the distal third of the forearm and zone IX being the proximal two-thirds of the forearm. Additionally, the absence of interlinking collagen bundles results in reduced holding strength for sutures [5]. Zone VII injuries, occurring at the level of the wrist joint beneath the extensor retinaculum, are particularly complex, as they often involve multiple tendons and are influenced by intricate biomechanical interactions. Timely and appropriate surgical intervention is essential to restore functional hand mechanics and prevent long-term disability. Neglected extensor tendon injuries are characterised by progressive tendon retraction, fibrosis, adhesion formation, and increased tendon gaps, rendering primary repair impractical. Several reconstructive options have been proposed, including tendon transfers, staged reconstruction, and free tendon grafting. Among these, fascia lata autograft has demonstrated favourable outcomes in reconstructing extensive tendon defects due to its tensile strength, adequate length, and ease of harvest [6]. Additionally, fascia lata graft harvest is associated with limited donor-site morbidity. We report a case of a neglected multiple extensor tendon injury in zone VII successfully managed with fascia lata autograft reconstruction, emphasising the clinical significance of juncturae tendinum and the role of early postoperative rehabilitation.
The patient presented with a history of an accidental glass-cut injury to the dorsal aspect of the right hand sustained 2 months prior. Initial treatment was performed at a peripheral healthcare facility, where wound irrigation and primary skin closure were undertaken without definitive tendon repair. Over the subsequent weeks, the patient noted a gradual and progressive inability to actively extend the index and middle fingers.
Clinical examination:
Physical examination revealed a healed scar measuring approximately 3 × 0.5 cm over the dorsal wrist. Active extension of the index finger was absent, although passive mobility was preserved. The middle finger demonstrated partial active extension, while extension of the ring and little fingers remained intact. Grip strength was notably reduced compared with the contralateral hand. Sensory examination did not reveal any deficits. The QuickDASH score for the affected upper limb at presentation was 52.44% (Fig. 1).

Figure 1: Preoperative image demonstrating attempted finger extension with extensor lag of index and middle fingers.
Imaging:
Plain radiographs of the wrist and hand showed no associated fractures or foreign bodies. Ultrasonographic evaluation of the wrist revealed a complete rupture of the extensor digitorum communis (EDC) tendon of the index finger with tendon separation and fluid accumulation within the tendon sheath. A near-complete rupture of the EDC tendon of the middle finger was also identified at the level of zone VII.
Intraoperative findings:
Surgical exploration demonstrated the following findings:
- Complete transection of the EDC and extensor indicis proprius tendons of the index finger
- Complete transection of the EDC tendon of the middle finger
- Approximately 50% partial tear of the EDC tendon of the ring finger.
The distance between the proximal and distal tendon ends measured approximately 11 cm, precluding primary tendon repair (Fig. 2).

Figure 2: Exposure zone VII extensor tendons with multiple tendon transections showing proximal and near cut ends of tendons with gap (~11 cm).
Surgical technique:
Reconstruction was performed using a fascia lata autograft harvested from the contralateral thigh. The graft was attached proximally to the EDC tendon using the Pulvertaft weaving technique. The fascia lata graft was carefully tunnelled beneath the extensor retinaculum to preserve the native tendon biomechanics, ensuring optimal gliding and preventing postoperative bowstringing. Distally, the graft was split into two strips: One strip was woven into the EDC tendon of the index finger and the other into the EDC tendon of the middle finger using the Pulvertaft technique. The partially transected EDC tendon of the ring finger was repaired primarily (Fig. 3).

Figure 3: Fascia lata graft tailored into two distal strips and used to bridge the tendon defects, passing beneath the extensor retinaculum and sutured to cut tendon ends.
Postoperative rehabilitation:
Postoperatively, the wrist and fingers were immobilised in a functional position for 3 weeks. Rehabilitation was then initiated, consisting of passive tendon-gliding exercises, active-assisted wrist and finger extension and use of a customised splint.
Physiotherapy was continued under close supervision to optimise tendon excursion and functional recovery (Fig. 4).

Figure 4: Postoperative photograph showing application of customized extension splint.
Complications:
The patient developed localised swelling measuring 1 × 1 cm over the dorsal aspect of the right hand at the scar site, at the base of the third metacarpal. At the 6-month follow-up, ultrasonography of the right hand showed a soft tissue nodule measuring 0.3 × 0.6 × 0.4 cm over the dorsal aspect of the hand at the mid-third metacarpal level, suggestive of a suture-site granuloma. The patient underwent excision of the suture granuloma as a day-care procedure and subsequently recovered completely (Fig. 5).

Figure 5: Preoperative and postoperative image of suture granuloma excision.
At 6 months follow-up, the patient exhibited marked improvement in active extension of the index and middle fingers. Grip strength, pinch strength, and overall hand function improved progressively. The patient was able to perform activities of daily living with minimal residual limitation and expressed satisfaction with the surgical outcome (Fig. 6 and Flowchart 1).
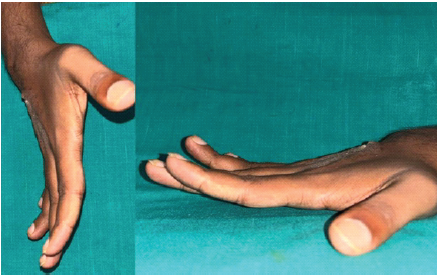
Figure 6: 6 months post follow up showing extension of index and middle finger with no extensor lag.
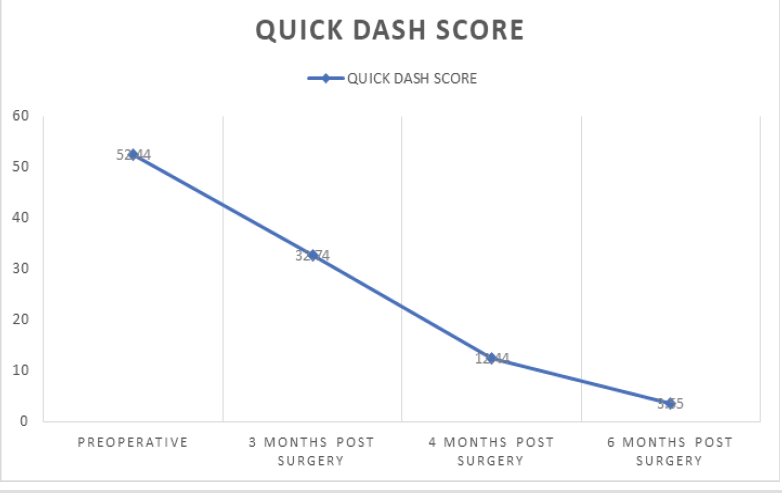
Flowchart 1: Quick dash score assessment.
Neglected extensor tendon injuries present substantial reconstructive challenges due to tendon retraction, scarring, and the formation of extensive tendon gaps. Accurate and timely diagnosis is essential to prevent permanent functional impairment. Injuries involving zone VII are particularly demanding due to the confined space beneath the extensor retinaculum and frequent involvement of multiple tendons [7]. A thorough clinical history – including the mechanism of injury, finger position at the time of trauma, progression of deformity, and hand dominance – is essential when planning management. Imaging modalities such as ultrasonography and magnetic resonance imaging (MRI) can assist in determining the extent, level, and gap of tendon injury. In the present case, functional disability associated with a zone VII injury warranted operative management. A comprehensive diagnostic workup was undertaken prior to surgical intervention. Plain radiographs of the wrist and hand were obtained to rule out associated fractures or foreign bodies, particularly given the history of glass-cut injury. Dynamic clinical assessment of tendon function, including tenodesis effect and independent finger extension, was performed to evaluate the integrity of the extensor mechanism. Ultrasonography was utilised as the primary imaging modality due to its accessibility and ability to provide dynamic assessment of tendon continuity, level of injury, and gap estimation. Although MRI can provide superior soft tissue delineation, it was not performed in this case, as ultrasound findings were conclusive and correlated well with clinical examination. Neurovascular assessment was carried out and found to be normal. No additional systemic evaluation was required as the injury was localised with no clinical suspicion of associated systemic or proximal pathology. Reported long-term outcomes following extensor tendon repair demonstrate 63–83% favourable results in proximal zones (V–VIII), compared with <50% good outcomes in distal zones (I–IV) [8]. In delayed presentations such as ours, primary repair is often not feasible, making free tendon grafting the preferred reconstructive strategy [9]. Fascia lata autograft offers multiple advantages, including sufficient length, high tensile strength, excellent biological compatibility, and minimal donor-site morbidity, making it a viable alternative to grafts such as the palmaris longus, particularly for large defects [10]. Preservation of partial finger extension despite complete tendon disruption may be explained by the presence of juncturae tendinum, which facilitate force transmission between adjacent extensor tendons and may mask the severity of injury [11]. This phenomenon accounted for the retained extension of the middle finger in our patient. Controlled mobilisation following secure reconstruction is crucial to minimise adhesion formation, enhance tendon gliding, and improve functional outcomes. We employed the Norwich rehabilitation regimen, involving initial immobilisation followed by static splinting with active-assisted extension and controlled passive sliding exercises. While dynamic splinting may yield superior results, it requires complex systems; hence, controlled active mobilisation without dynamic splinting was preferred [12]. Meticulous evaluation of all dorsal hand and forearm wounds is imperative to avoid missing extensor tendon injuries. In cases of uncertainty, surgical exploration should be considered to assess tendon integrity [13]. Surgeons should be prepared for tendon grafting, as even within a short duration, primary tenorrhaphy may not be possible.
A fascia lata autograft provides a dependable and effective solution for the reconstruction of neglected multiple extensor tendon injuries in zone VII. Awareness of juncturae tendinum is essential during clinical assessment. A structured postoperative rehabilitation protocol plays a decisive role in achieving favourable functional outcomes.
Neglected zone VII extensor tendon injuries associated with large tendon gaps can be successfully reconstructed using a fascia lata autograft when meticulous surgical technique is combined with structured rehabilitation.
References
- 1. Kontor JA. Extensor tendon injuries and repairs in the hand. Can Fam Physician 1982;28:1159-63. [Google Scholar] [PubMed]
- 2. Newport ML, Williams CD. Extensor tendon injuries. Hand Clin 1995;11:373-86. [Google Scholar] [PubMed]
- 3. Chester DL, Beale S, Beveridge L, Nancarrow JD, Titley OG. A prospective, controlled, randomized trial comparing early active extension with passive extension using a dynamic splint in the rehabilitation of repaired extensor tendons. J Hand Surg Br 2002;27:283-8. [Google Scholar] [PubMed]
- 4. Kleinert HE, Verdan C. Report of the committee on tendon injuries. J Hand Surg 1983;8A:794-8. [Google Scholar] [PubMed]
- 5. Verdan CE Primary and secondary repair of flexor and extensor injuries. In: Flynn IE, editor. Hand Surgery. Baltimore: Williams and Wilkins; 1966. p. 220-75. [Google Scholar] [PubMed]
- 6. Green DP, Hotchkiss RN, Pederson WC, Wolfe SW. Green’s Operative Hand Surgery. 6th ed. Philadelphia, PA: Elsevier Churchill Livingstone; 2011. p. 187-215. [Google Scholar] [PubMed]
- 7. Wehbé MA, Schneider LH. Extensor tendon injuries. Clin Orthop Relat Res 1984; 183:75-90. [Google Scholar] [PubMed]
- 8. Colzani G, Tos P, Battiston B, Merolla G, Porcellini G. Traumatic extensor tendon injuries to the hand: Clinical anatomy, biomechanics, and surgical procedure review. J Hand Microsurg 2016;8:2-12. [Google Scholar] [PubMed]
- 9. Doyle JR. Extensors Tendons-Acute Injuries. Philadelphia, PA: Elsevier Churchill Livingstone; 1999. p. 195-219. [Google Scholar] [PubMed]
- 10. Stern PJ. Tendon grafting and reconstruction. J Hand Surg Am 1991;16:913-8. [Google Scholar] [PubMed]
- 11. Landsmeer JM. The anatomy of the dorsal aponeurosis of the human finger and its functional significance. Anat Rec 1949;104:31-44. [Google Scholar] [PubMed]
- 12. Sylaidis P, Youatt M, Logan A. Early active mobilization for extensor tendon injuries. The norwich regime. J Hand Surg Br 1997;22:594-6. [Google Scholar] [PubMed]
- 13. Wiktor Ł, Tomaszewski R. Neglected zone VII extensor tendons reconstruction with a palmaris longus tendon autograft. Medicina (Kaunas) 2025;61:249. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Vascularized First Dorsal Metacarpal Artery-Based Adipofascial Flap to Augment Multiple Zone VII Extensor Tendon Repairs after Glass Laceration: A Case Report
July 1, 2026 Vascularized First Dorsal Metacarpal Artery-Based Adipofascial Flap to Augment Multiple Zone VII Extensor Tendon Repairs after Glass Laceration: A Case Report May 1, 2026 Semitendinosus Autograft Reconstruction for Neglected Patellar Tendon Rupture: Technical Simplicity with Excellent Outcome
May 1, 2026 Semitendinosus Autograft Reconstruction for Neglected Patellar Tendon Rupture: Technical Simplicity with Excellent Outcome January 1, 2025 A Case Report: Interposition Arthroplasty for Post-traumatic Elbow Arthritis
January 1, 2025 A Case Report: Interposition Arthroplasty for Post-traumatic Elbow Arthritis November 10, 2022 Management of Neglected Patellar Tendon Rupture by Peroneus Longus Autograft and Suture Anchor: A Case Report
November 10, 2022 Management of Neglected Patellar Tendon Rupture by Peroneus Longus Autograft and Suture Anchor: A Case Report