
The lateral femoral cutaneous nerve is vulnerable during the direct anterior approach in total hip arthroplasty, and nerve capping may be a suitable treatment option for symptomatic neuroma relief.
Dr. Michael John Zappa, 1307 Federal Street, Pittsburgh, PA, 15214, United States. E-mail: zappam14@gmail.com
Abstract
Introduction: The direct anterior approach (DAA) for primary and revision total hip arthroplasty (THA) has been growing in popularity due to reported less soft tissue disruption, less post-operative pain, earlier post-operative functional recovery, and a lower dislocation rate. One potential complication of this approach is damage to the lateral femoral cutaneous nerve (LFCN). The incidence of damage to the LFCN in the literature ranges from 14.8% to 81%. Documented treatments consist mainly of conservative measures; however, here, we describe a case where operative intervention was pursued due to failure of conservative measures.
Case Report: A 59-year-old male with a history of primary and revision DAA THA was referred to the upper extremity clinic for evaluation and treatment of painful LFCN neuroma. After failing non-operative management, the patient underwent LFCN exploration, neuroma excision, and placement of a nerve cap. The patient demonstrated significant improvement in subjective and objective measures at the 1-year post-operative time point.
Conclusion: Care must be taken during the proximal incision extent in DAA THA due to anatomic variations of the LFCN. Although there is not an abundance of evidence, nerve capping may be a reasonable solution for those patients with severe LFCN neuropathy who have failed conservative modalities.
Keywords: Total hip arthroplasty, lateral femoral cutaneous nerve, neuroma, nerve capping, case report.
The direct anterior approach (DAA) for primary and revision total hip arthroplasty (THA) has been growing in popularity for its reported less soft tissue trauma, less post-operative pain, earlier post-operative functional recovery, and lower dislocation rates [1,2]. One potential complication, however, is injury to the lateral femoral cutaneous nerve (LFCN) [3,4,5,6,7,8]. The LFCN is a sensory nerve that supplies the cutaneous area of the anterolateral thigh. It originates from the dorsal divisions of the second and third lumbar nerves, courses along the psoas muscle, and exits the pelvis superficial to the sartorius and tensor fascia lata (TFL). It is here, between the sartorius and TFL, where the LFCN can be injured in the DAA [3,9]. The incidence of LFCN injury in the DAA has ranged from 14.8% to 81% in the literature [8,10,11]. If injured, patients can present with numbness and potentially neuropathic pain along the anterolateral thigh. Documented treatments consist mostly of observation [7,10,11]. Here, we present a case of a patient who developed severe neuropathic pain originating from an LFCN neuroma noted after a revision THA through a DAA, treated by LFCN exploration, neuroma excision, and placement of a nerve cap.
A 59-year-old male with a history of right primary and revision DAA THA was referred to the Hand and Upper Extremity clinic for evaluation and treatment of a painful LFCN neuroma. His past medical history included a body mass index of 26.5 kg/m², a remote history of alcohol abuse, and chronic opioid use since his primary THA. Index primary THA was performed 4 years before osteoarthritis through a DAA (Figs. 1 and 2).
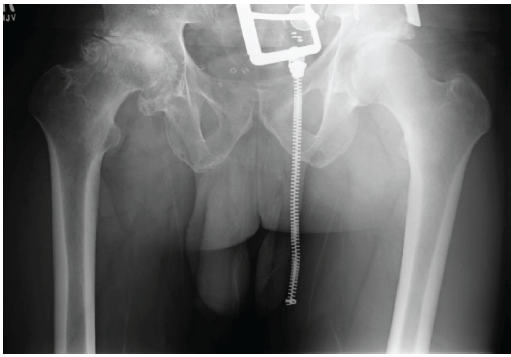
Figure 1: Pre-operative anteroposterior pelvis plain radiograph showing significant right hip arthritis, femoral head collapse, and osteophyte formation.
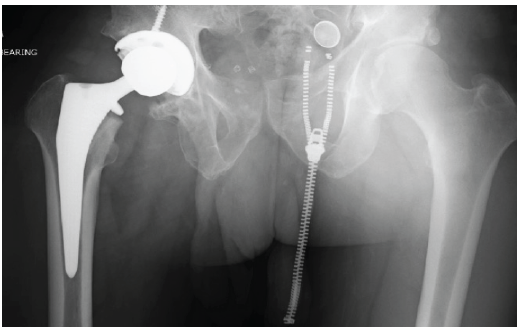
Figure 2: Post-operative anteroposterior (AP) pelvis plain radiograph status post primary right total hip arthroplasty. Leg lengths and offset on the AP pelvis X-ray noted to be within a few millimeters compared to the contralateral side.
His post-operative course was complicated by persistent anterolateral hip pain. Initial conservative management consisting of trochanteric bursa injection, physical therapy, and shoe lifts failed to improve his pain. Work-up showed no signs of infection. He was noted postoperatively to have a 1 cm long leg length discrepancy on the operative side, due to a prior tibial malunion on the contralateral limb. The patient’s persistent post-operative anterolateral hip pain at this point was determined to be due to overlengthening. Approximately 8 months after the index THA, the patient underwent DAA revision hip arthroplasty. The original incision was extended proximally to perform a TFL release. A +4 mm head was exchanged for a −3 mm head, which decreased his leg length and offset approximately 4–5 mm (Fig. 3).
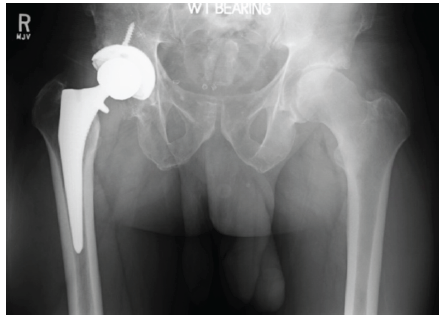
Figure 3: Post-operative anteroposterior pelvis plain radiograph status post revision of right total hip arthroplasty for functional leg length discrepancy. The femoral head was downsized from +4 mm to −3 mm decreasing the leg length and offset about 4–5 mm.
During his post-operative course, he developed hyperaesthesia and allodynia over the anterolateral thigh along with a positive Tinel’s sign over the entire incision. Lidocaine injection at the proximal incision in the region of the LFCN provided short-term relief of symptoms, confirming the presumed diagnosis of neuroma/complex regional pain syndrome (CRPS) II. He underwent extensive conservative management, including a multimodal pain regimen and trochanteric bursitis injection, which did not provide symptomatic relief. After failing these modalities, he also underwent two LFCN radiofrequency ablations (RFAs) 6 months after the revision surgery with approximately 3 months of improvement after each RFA procedure. A magnetic resonance imaging of the hip was obtained, which did not show any abnormal findings. Inflammatory markers and serum metal ion levels were within normal limits. The patient was sent to an upper extremity nerve specialist for further evaluation. Physical examination at this time demonstrated a positive Tinel’s sign over the entire length of the previous incision, significant hypersensitivity to touch about the incision, and pain about the proximal extent of the incision with hip flexion. The patients’ symptoms were determined to be due to neuroma formation. Subsequently, the patient underwent exploration of the LFCN, excision of the neuroma, and nerve capping of the posterior branch. Please see the surgical technique section below for details regarding the procedure. At the patient’s 1-year post-operative visit, he noted significant improvement in his neuropathic pain. Physical examination at this time demonstrated resolution of Tinel’s sign and hypersensitivity along the distal 75–80% of his incision. He continues to have mild discomfort over the lateral hip but reports significant improvement when compared to pre-procedure. Further, he reports that he is limping less, no longer requires a cane outside of the house, and can comfortably ambulate around a grocery store without taking breaks to rest. In addition, he was noted to be able to participate more in physical therapy due to improvement of anterior neuropathic-type pain. He had significantly decreased his pain medication use, including Percocet, tramadol, and Neurontin.
Surgical technique:
The patient underwent exploration of the LFCN, excision of the neuroma, and nerve capping of the posterior branch. The patients’ original incision was extended both proximally toward the anterior superior iliac spine (ASIS) and distally down the thigh. Dense scar tissue was noted. The LFCN was located just lateral to the ASIS, exiting below the inguinal ligament (Fig. 4).
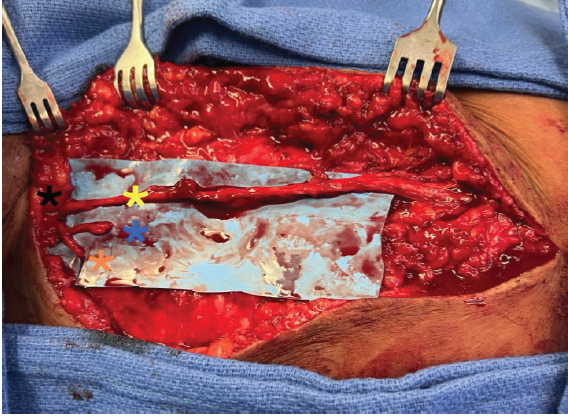
Figure 4: Exploration of lateral femoral cutaneous nerve (LFCN). Black star represents location of anterior superior iliac spine. It is important to note the LFCN traveling laterally to the anterior superior iliac spine. Yellow star shows the intact anterior branch of the LFCN traveling down the lateral thigh. Blue star displaying the lacerated posterior branch with resected neuroma. Orange star is showing a second posterior branch that is intact diving below the blue sheet.
The inguinal ligament and sartorius fascia were noted to be tight, leading to compression of the LFCN. The nerve was subsequently de-compressed. The anterior branch was dissected distally for 15 cm, and no damage to the nerve was noted; however, there was a dense, adherent scar throughout its length. The posterior branch was then identified proximally about 1 cm distal from the ASIS. Multiple branches were noted and extended laterally in a fan-like distribution. One of the branches was previously injured and noted to have a neuroma formation that was later confirmed by pathology. This was excised sharply. An AxoGen nerve cap was placed on the end of the lysed nerve (Fig. 5).
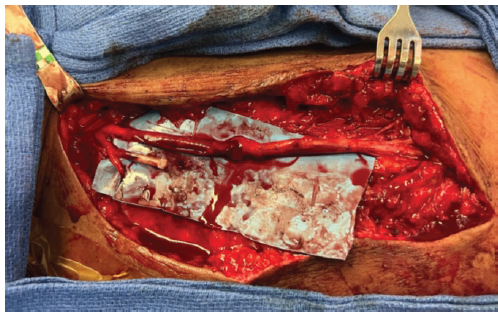
Figure 5: Status post nerve capping of lacerated posterior lateral femoral cutaneous nerve branch.
To prevent further scar formation and possible compression along the anterior branch, an AxoGen nerve wrap was utilised and loosely secured around the nerve.
Here, we present a case with injury to the posterior branch of the LFCN following primary and revision THA through a DAA. The patient subsequently developed symptomatic neuroma formation and the development of CRPS Type II. Failure of conservative management consisting of physical therapy, pain management, injections, and RFAs led us to perform a nerve exploration, neuroma resection, and nerve capping. To our knowledge, there are no other case reports documenting this procedure. LFCN injuries are prevalent and have been documented to range from 14.8% to 81%. Presentation can range from mild numbness and tingling to severe meralgia paresthetica [4]. Observation has been shown to be a promising treatment option. Ozaki et al. showed that with observation alone, the incidence of neuropathic-related symptoms decreased 96% at 26-month follow-up [10]. Patton et al. and Vajapey et al. had similar results at 2 years as well. On the contrary, Schwaiger et al. looked at 16 patients who failed conservative management and underwent surgical decompression of the LFCN for meralgia paresthetica. Of these patients, 86% reported complete satisfaction, and 14% reported partial satisfaction [12]. It is believed that the majority of these nerve-related injuries are secondary to retractors and stretches placed on the nerve during the time of surgery [3]. Recommendations have been made on safe approach technique, but anatomic variations in the LFCN make this difficult. Anatomic variations of the LFCN were described by Bartlett et al. and Rudin et al., who showed that the LFCN crossed the DAA incisional line 44% and 32%, respectively [3,9]. Bartlett et al. also showed that the LFCN travelled lateral to the ASIS in 11% of cases [3]. This is similar to the course of the LFCN our patient had and poses a high risk of nerve injury by crossing the DAA incision at an abnormal location. Furthermore, the incision had to be extended proximally at the time of the revision surgery to perform a release of the TFL, putting the LFCN at increased risk. Biedermann et al. showed that performing a TFL release in pelvic osteotomies leads to a 30% incidence of LFCN dysesthesias [13]. The treatment of neuromas remains a challenge. Various treatment options are now available, including both conservative and surgical. Pharmacotherapies such as antidepressants and antiepileptics remain the basis of traumatic neuropathic pain management. For those that fail these modalities, procedures involving regenerative peripheral nerve interface can be performed, where the nerve stump can be transpositioned into a muscle, vein, or bone, which have some degree of efficacy [14,15]. Newer modalities include nerve capping, electrical stimulation, and adipose autograft [14]. Nerve capping has been thoroughly studied in animal models [16,17,18,19,20,21]. The idea is to cover the proximal nerve stump to prevent axonal fibre growth, scarring, and adhesions which would ultimately block neuroma formation and pain. Several studies have looked at nerve capping in humans [22,23]. Uemura et al. present a case report of nerve capping a digital nerve in a patient who developed a painful digital neuroma. The patient had an equivalent reduction in disabilities of the arm, shoulder, and hand scores compared to studies of digital nerve transposition into muscle and bone [23]. Gould et al. also looked at nerve capping in neuromas in the foot and ankle [22]. He showed that 85% of patients had significant improvement in pain scores.
Care must be taken during the proximal incision extent in DAA THA due to anatomic variations of the LFCN, especially in cases requiring TFL release and revision THA with scarred and abnormal anatomy. Although there is not an abundance of evidence, nerve capping may be a reasonable solution for those patients with severe LFCN neuropathy who have failed conservative modalities.
The lateral femoral cutaneous nerve is vulnerable to iatrogenic injury during the direct anterior approach during total hip arthroplasty. Similar to injuries to other peripheral nerves, a symptomatic neuroma may develop if the nerve is injured. The treatment of symptomatic neuromas remains a challenge. Conservative measures range from observation to medical management with antiepileptics and antidepressants. In this case report, we describe a novel technique of neuroma excision and “nerve capping” which demonstrated significant improvement of subjective and objective symptoms at the 1-year post-operative time point. To our knowledge, this is the 1st time this technique has been described in the literature for neuromas involving the lateral femoral cutaneous nerve.
References
- 1. Goebel S, Steinert AF, Schillinger J, Eulert J, Broscheit J, Rudert M, et al. Reduced postoperative pain in total hip arthroplasty after minimal-invasive anterior approach. Int Orthop 2012;36:491-8. [Google Scholar] [PubMed]
- 2. Restrepo C, Parvizi J, Pour AE, Hozack WJ. Prospective Randomized Study of Two Surgical Approaches for Total Hip Arthroplasty. J Arthroplasty 2010;25:671-9.e1. [Google Scholar] [PubMed]
- 3. Bartlett JD, Lawrence JE, Khanduja V. What is the risk posed to the lateral femoral cutaneous nerve during the use of the anterior portal of supine hip arthroscopy and the minimally invasive anterior approach for total hip arthroplasty? Arthroscopy 2018;34:1833-40. [Google Scholar] [PubMed]
- 4. DeHart MM, Riley LH. Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg 1999;7:101-11. [Google Scholar] [PubMed]
- 5. Goulding K, Beaulé PE, Kim PR, Fazekas A. Incidence of lateral femoral cutaneous nerve neuropraxia after anterior approach hip arthroplasty. Clin Orthop Related Res 2010;468:2397-404. [Google Scholar] [PubMed]
- 6. Homma Y, Baba T, Sano K, Ochi H, Matsumoto M, Kobayashi H, et al. Lateral femoral cutaneous nerve injury with the direct anterior approach for total hip arthroplasty. Int Orthop 2016;40:1587-93. [Google Scholar] [PubMed]
- 7. Patel NK, Krumme J, Golladay GJ. Incidence, Injury Mechanisms, and Recovery of Iatrogenic Nerve Injuries During Hip and Knee Arthroplasty. J Am Acad Orthop Surg 2021;29:e940-9. [Google Scholar] [PubMed]
- 8. Vajapey SP, Morris J, Lynch D, Spitzer A, Li M, Glassman AH. Nerve injuries with the direct anterior approach to total hip arthroplasty. JBJS Rev 2020;8:1-8. [Google Scholar] [PubMed]
- 9. Rudin D, Manestar M, Ullrich O, Erhardt J, Grob K. The anatomical course of the lateral femoral cutaneous nerve with special attention to the anterior approach to the hip joint. J Bone Joint Surg Am 2016;98:561-7. [Google Scholar] [PubMed]
- 10. Ozaki Y, Homma Y, Baba T, Sano K, Desroches A, Kaneko K. Spontaneous healing of lateral femoral cutaneous nerve injury and improved quality of life after total hip arthroplasty via a direct anterior approach. J Orthop Surg (Hong Kong) 2017;25:2309499016684750. [Google Scholar] [PubMed]
- 11. Patton RS, Runner RP, Lyons RJ, Bradbury TL. Clinical outcomes of patients with lateral femoral cutaneous nerve injury after direct anterior total hip arthroplasty. J Arthroplasty 2018;33:2919-26.e1. [Google Scholar] [PubMed]
- 12. Schwaiger K, Panzenbeck P, Purschke M, Russe E, Kaplan R, Heinrich K, et al. Surgical decompression of the lateral femoral cutaneous nerve (LFCN) for Meralgia paresthetica treatment: Experimental or state of the art? A single-center outcome analysis. Medicine (Baltimore) 2018;97:e11914. [Google Scholar] [PubMed]
- 13. Biedermann R, Donnan L, Gabriel A, Wachter R, Krismer M, Behensky H. Complications and patient satisfaction after periacetabular pelvic osteotomy. Int Orthop 2008;32:611-7. [Google Scholar] [PubMed]
- 14. Regal S, Tang P. Surgical management of neuromas of the hand and wrist. J Am Acad Orthop Surg 2019;27:356-63. [Google Scholar] [PubMed]
- 15. Yao C, Zhou X, Zhao B, Sun C, Poonit K, Yan H. Treatments of traumatic neuropathic pain: A systematic review. Oncotarget 2017;8:57670-9. [Google Scholar] [PubMed]
- 16. Nieto FR, Cendán CM, Cañizares FJ, Cubero MA, Vela JM, Fernández-Segura E, et al. Genetic inactivation and pharmacological blockade of sigma-1 receptors prevent paclitaxel-induced sensory-nerve mitochondrial abnormalities and neuropathic pain in mice. Mol Pain 2014;10:11. [Google Scholar] [PubMed]
- 17. Okuda T, Ishida O, Fujimoto Y, Tanaka N, Inoue A, Nakata Y, et al. The autotomy relief effect of a silicone tube covering the proximal nerve stump. J Orthop Res 2006;24:1427-37. [Google Scholar] [PubMed]
- 18. Sakai Y, Ochi M, Uchio Y, Ryoke K, Yamamoto S. Prevention and treatment of amputation neuroma by an atelocollagen tube in rat sciatic nerves. J Biomed Mater Res 2005;73B:355-60. [Google Scholar] [PubMed]
- 19. Yan H, Zhang F, Kolkin J, Wang C, Xia Z, Fan C. Mechanisms of nerve capping technique in prevention of painful neuroma formation. PLoS One 2014;9:e93973. [Google Scholar] [PubMed]
- 20. Yan H, Zhang F, Wang C, Xia Z, Mo X, Fan C. The role of an aligned nanofiber conduit in the management of painful neuromas in rat sciatic nerves. Ann Plast Surg 2015;74:454-61. [Google Scholar] [PubMed]
- 21. Yi J, Jiang N, Li B, Yan Q, Qiu T, Swaminatha Iyer K, et al. Painful terminal neuroma prevention by capping PRGD/PDLLA conduit in rat sciatic nerves. Adv Sci (Weinh) 2018;5:1700876. [Google Scholar] [PubMed]
- 22. Gould JS, Naranje SM, McGwin G Jr., Florence M, Cheppalli S. Use of collagen conduits in management of painful neuromas of the foot and ankle. Foot Ankle Int 2013;34:932-40. [Google Scholar] [PubMed]
- 23. Uemura T, Onode E, Yokoi T, Shintani K, Okada M, Takamatsu K, et al. Nerve capping technique with nerve conduit for treating painful digital neuroma: A case report. J Orthop Sci 2022;27:284-7. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Management of Subtrochanteric Femur Fracture with Pre-existing Grade IV Psoriatic Hip Arthritis Using Primary Total Hip Arthroplasty with a Long Distal-Loading Stem: A Case Report
April 1, 2026 Management of Subtrochanteric Femur Fracture with Pre-existing Grade IV Psoriatic Hip Arthritis Using Primary Total Hip Arthroplasty with a Long Distal-Loading Stem: A Case Report August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report
August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report August 1, 2026 Posterior Acetabular Wall Fracture Mimicking a Subcapital Femoral Neck Fracture on Plain Radiographs: A Diagnostic Pitfall and the Role of Intraoperative Fluoroscopy: A Case Report
August 1, 2026 Posterior Acetabular Wall Fracture Mimicking a Subcapital Femoral Neck Fracture on Plain Radiographs: A Diagnostic Pitfall and the Role of Intraoperative Fluoroscopy: A Case Report August 1, 2026 Case Report of Rapidly Destructive Osteoarthritis of the Hip following Multiple High-dose Intra-articular Steroid Injections
August 1, 2026 Case Report of Rapidly Destructive Osteoarthritis of the Hip following Multiple High-dose Intra-articular Steroid Injections