
Early fixation failure combined with post-operative infection in subtrochanteric femur fractures can rapidly lead to profound proximal femoral bone loss. A structured two-stage approach, beginning with aggressive debridement and antibiotic spacer placement followed by long-stem revision arthroplasty, provides a reliable strategy for infection control and limb reconstruction.
Dr. Ibaad Khan, Department of Orthopaedic Surgery, Rothman Orthopaedic Institute, Philadelphia, Pennsylvania, USA. E-mail: ibaadkhan0@gmail.com
Abstract
Introduction: Subtrochanteric femur fractures are difficult to manage due to high mechanical stresses and complex deforming forces. Treatment often involves placing an intramedullary nail (IM nail) for stabilisation and early mobilisation. Despite being the preferred fixation method, IM nail constructs remain vulnerable to failure, and repeated fixation attempts can compromise remaining bone stock. When fixation failure occurs in conjunction with early post-operative infection, the combined instability and bone loss may necessitate staged reconstruction.
Case Report: A 40-year-old female sustained a right subtrochanteric femur fracture after a motor vehicle collision and underwent IM nail fixation utilising a recon-style design. Within 1 month, she developed progressive displacement with proximal screw cutout and underwent hardware removal and revision nailing utilising a cephalomedullary design with a lag screw. Nineteen days later, the revision construct failed with a new femoral neck fracture and further proximal femoral erosion. She subsequently developed thigh pain and erythema, with elevated inflammatory markers and aspiration cultures positive for Staphylococcus capitis, confirming early post-operative peri-implant infection. The decision was made to proceed with a two-stage reconstruction. Stage 1 involved explantation of all hardware, aggressive synovectomy, and placement of a high-dose static antibiotic spacer consisting of a cemented acetabular ball and an antibiotic cement-coated IM nail. After clinical resolution of infection, she underwent a second-stage revision total hip arthroplasty through a posterior approach. Reconstruction utilised a 54 mm press-fit acetabular cup with a dual mobility liner and a 17 × 300 mm diaphyseal-engaging monoblock tapered fluted titanium stem with cerclage stabilisation. Her post-operative course was notable for a single posterior dislocation managed with closed reduction. At the latest follow-up 4 months postoperatively, she demonstrated stable reconstruction without recurrent infection.
Conclusion: Fixation failure of subtrochanteric femur fractures combined with early post-operative infection can lead to profound proximal femoral bone loss. This case demonstrates successful management using a two-stage approach with aggressive debridement, static antibiotic spacer placement, and definitive revision THA in the setting of acquired extensive proximal femoral bone loss.
Keywords: Subtrochanteric femur fracture, fixation failure, peri-implant infection, proximal femoral bone loss, two-stage reconstruction, revision total hip arthroplasty.
Subtrochanteric femur fractures remain exceptionally challenging to manage primarily due to their complicated, powerful deforming forces, which render successful reduction and fixation challenging [1]. Intramedullary nailing (IM nail) is considered the “gold standard” for treatment of these fractures; however, complications still may occur. Panteli et al. identified a 22.3% re-operation rate in subtrochanteric fractures treated with an IM nail, with individuals younger than 75 and those with fracture-related infection and non-union at higher risk [2]. Repeated failure of fixation can lead to progressive bone loss and an increased risk of instability and infection. When operative fixation of fractures is complicated by infection, patients are at risk for a compromised functional recovery and higher rates of mortality [3,4]. When extensive bone loss and peri-implant infection occur together in the treatment of proximal femoral fractures, joint-preserving fixation becomes exceedingly challenging, and conversion to total hip arthroplasty (THA) is often required. Management involves a staged approach to infection management before definitive reconstruction. We present a case of a subtrochanteric femur fracture complicated by sequential fixation failures and early post-operative infection resulting in acquired extensive proximal femoral bone loss, ultimately requiring two-stage reconstruction with revision THA for limb salvage.
Initial fracture and failure of fixation:
A 40-year-old female with a history of peripartum cardiomyopathy with reduced ejection fraction requiring a left ventricular assist device, atrial fibrillation on warfarin, and alcohol use disorder sustained a right-sided closed subtrochanteric femur fracture from a motor vehicle collision (Fig. 1a and b).
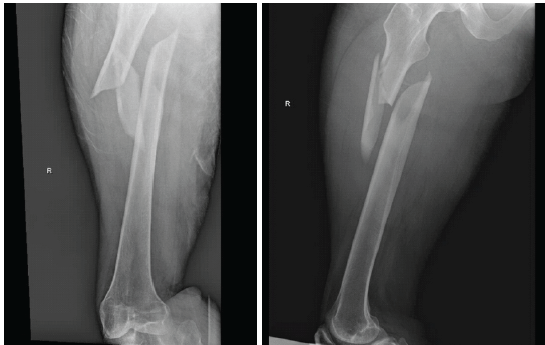
Figure 1: (a and b) Initial subtrochanteric femur fracture. Anteroposterior (a) and lateral (b) radiographs demonstrating a right subtrochanteric femur fracture with characteristic proximal fragment flexion/abduction and comminution consistent with a high-energy injury.
She underwent operative fixation with a reconstruction IM nail, with an initially uncomplicated postoperative course (Fig. 2).
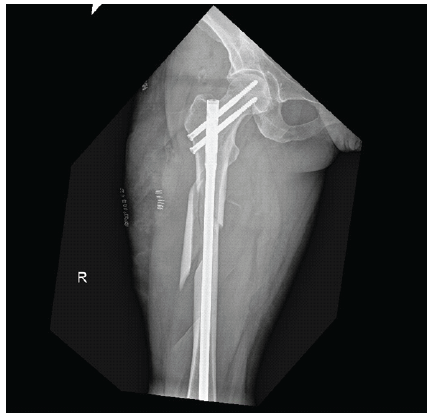
Figure 2: Initial intramedullary nail fixation. Immediate post-operative anteroposterior radiograph following intramedullary nail fixation of the subtrochanteric fracture, demonstrating initial acceptable alignment and implant positioning.
Postoperatively, she was made weight-bearing as tolerated (WBAT). Within 4 weeks, she developed increased pain, and radiographs demonstrated fracture displacement with proximal screw cutout, fracture propagation into the femoral neck, and progressive proximal femoral erosion (Fig. 3).

Figure 3: Failure of initial fixation. Anteroposterior radiograph showing interval loss of reduction with proximal screw cutout, flexion of the proximal fragment, and progressive proximal femoral erosion consistent with early fixation failure.
She subsequently underwent hardware removal and revision IM nailing with a cephalomedullary nail with a lag screw (Fig. 4).

Figure 4: Revision intramedullary (IM) nailing with femoral neck fixation. Post-operative anteroposterior radiograph after hardware removal and revision IM nailing with femoral neck fixation using a cephalomedullary screw as a locked, cannulated lag screw.
Postoperatively, she was made toe-touch weight-bearing (TTWB). Nineteen days later, the revision construct failed with displacement of the femoral neck fracture and further loss of proximal femoral structural integrity (Fig. 5).
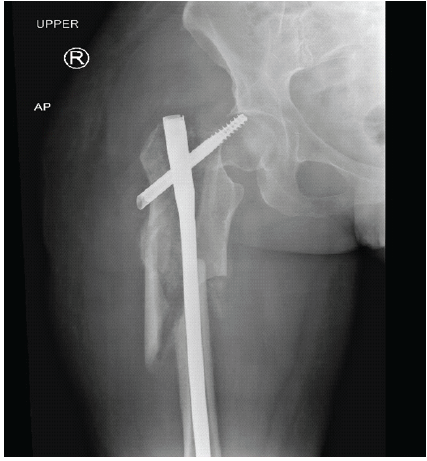
Figure 5: Second failure with a new femoral neck fracture. Anteroposterior radiograph following revision intramedullary nail and femoral neck fixation demonstrating subsequent failure with displacement of the femoral neck fracture and further compromise of proximal femoral structural integrity.
She underwent a second revision consisting of hardware removal, revision of intramedullary fixation and placement of a locking compression plate on the proximal anterolateral femur (Fig. 6).
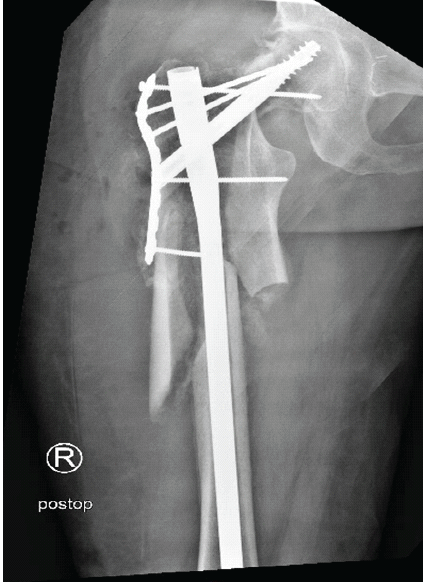
Figure 6: Second revision with revision intramedullary (IM) nailing and proximal femoral locking plate. Post-operative anteroposterior radiograph after removal of hardware and revision IM nailing with femoral neck fixation using a cephalomedullary screw as a locked cannulated lag screw in addition to placement of a locking compression plate on the proximal anterolateral femur. Calcium phosphate cement and demineralized bone matrix evident after placement into a large posterolateral femoral head defect.
During this second revision a large posterolateral femoral head defect was observed; this was treated with injection of calcium phosphate cement and demineralised bone matrix. Within 2 weeks, she developed increasing thigh pain and erythema, and laboratory studies demonstrated rising inflammatory markers (erythrocyte sedimentation rate [ESR] of 74 mm/hr and C-reactive protein [CRP] of 15.25 mg/dL). Hip aspiration cultures grew Staphylococcus capitis (erythromycin resistant), confirming early postoperative peri-implant infection. Due to these findings, the decision was made to transfer the patient to a tertiary care adult reconstruction practice to proceed with a two-stage reconstruction.
Stage 1: Explantation, debridement, and antibiotic spacer placement:
The patient underwent the first stage of the spacer, which required the removal of hardware using her prior lateral approach. A sinus tract in the fascia directly communicated with the hip joint. Significant fibrinous and necrotic tissue was encountered, and a thorough synovectomy was performed using a rongeur and electrocautery. All hardware was removed. The femoral head was fragmented, and the acetabulum demonstrated significant erosion; loose necrotic bone was removed in pieces. Aggressive irrigation and debridement were performed of the acetabulum, femoral canal, and surrounding soft tissues using saline, dilute betadine, hydrogen peroxide, and Dakin’s solution. After the aforementioned debridement, a spacer was constructed. Five bags of cement were prepared, each containing 2 g vancomycin and 1.2 g tobramycin. Two bags were used to fashion an acetabular cement ball, and three bags were used to coat an antibiotic IM nail. A 35 mm screw was inserted into the pelvis to anchor the acetabular spacer. The femoral canal was reamed to 14 mm, and the antibiotic nail was inserted. Postoperatively, the patient was started on intravenous (IV) vancomycin and transitioned to IV cefazolin and IV daptomycin. Serial radiographs demonstrated stable spacer positioning and no progressive bone loss, and inflammatory markers normalised within a few months (Figs. 7a and b).
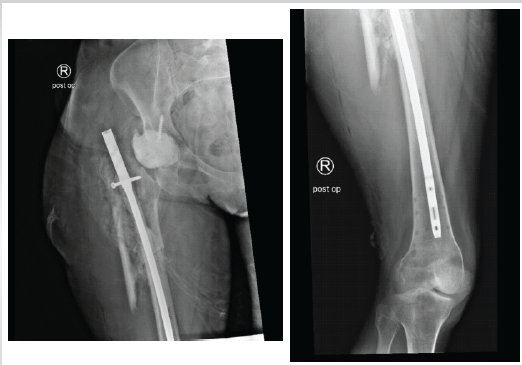
Figure 7: (a and b) Post-operative imaging after first-stage explantation and antibiotic spacer placement. Anteroposterior (a) and lateral (b) radiographs after first-stage surgery showing removal of failed hardware, placement of a static acetabular cement spacer, and insertion of an antibiotic-coated intramedullary nail spanning the proximal femoral defect.
Stage 2: Revision THA:
After clinical and biochemical resolution of infection, she returned for the second-stage revision THA. Pre-operative CRP was 6 mg/L, ESR was 15 mm/h, and joint fluid aspiration demonstrated a 7,553/µL total nucleated cell count with 83% neutrophils. A posterolateral approach incorporating her prior scar was used. The cemented acetabular spacer block, along with intramedullary rod, was removed, and dense fibrous tissue in the acetabulum was sharply debrided. Cultures were obtained. The hip and thigh were once again aggressively irrigated and debrided. Reconstruction proceeded with sequential acetabular reaming to 54 mm. A 54 mm modular revision acetabular component was implanted with excellent scratch fit, secured with five acetabular screws, and a dual-mobility liner was inserted. Attention was turned to the femur, where significant malrotation and proximal deformity were noted. Prophylactic cerclage wiring (three cables) was placed distal to prior callus and fracture sites. After removing residual cement, the canal was sequentially reamed to a size 17 × 300 mm diaphyseal-engaging monoblock tapered fluted titanium stem. A -3 head was trialled and was stable with no signs of impingement or dislocation through a full arc of motion. The final 17 × 300 mm diaphyseal-engaging monoblock tapered fluted titanium stem was implanted. Leg lengths and stability were confirmed under fluoroscopy. The wound was irrigated with 9 L of saline, betadine, and Dakin’s solution before closure. Post-operative radiographs demonstrated a well-positioned long-stem revision THA with cerclage cables (Fig. 8a and b).
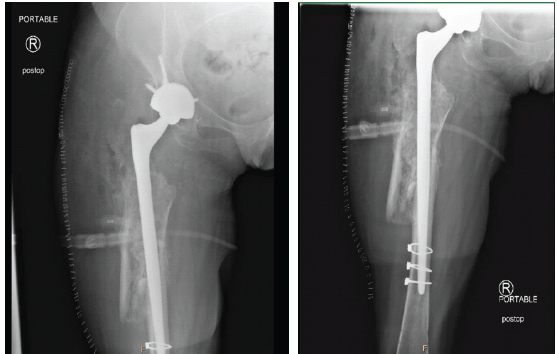
Figure 8: (a and b) Post-operative imaging after Stage 2 revision total hip arthroplasty. Proximal (a) and distal (b) Anteroposterior radiographs after revision total hip arthroplasty demonstrating a 54-mm acetabular shell with dual-mobility liner and a 17 × 300 mm tapered fluted revision femoral stem with cerclage fixation for diaphyseal support.
Post-operative course:
Postoperatively, she was TTWB with strict posterior precautions. She experienced a posterior hip dislocation 39 days postoperatively and successfully underwent closed reduction on a Hana table at our institution. Imaging demonstrated displaced right superior and inferior pubic rami fractures as well as a non-displaced left inferior pubic rami fracture, which were managed non-operatively. At the latest follow-up 4 months postoperatively, she was WBAT without use of an assistive device, with no evidence of recurrent infection and acceptable radiographic alignment.
The management of failed subtrochanteric femur fractures remains challenging, particularly when complicated by early post-operative infection and proximal femoral bone loss. Reduction can be challenging due to comminution and deforming muscle forces, and management may be complicated by loss of fixation and implant failure [5,6]. Infection represents a less common but significant complication when treating these fractures, with one study reporting that approximately 6.4% of subtrochanteric fractures managed with IM nails are complicated by infection [7]. Our patient demonstrated both failure of fixation and post-operative peri-implant infection, ultimately leading to progressive catastrophic destruction of the proximal femur. As infection serves to impair fracture healing and is a known driver of non-union, a comprehensive management approach was necessary in this case [8]. Given the extent of bone loss, necrotic tissue, and structural compromise noted intraoperatively, the decision was made to proceed with two-stage revision, as studies have demonstrated it to be a safe treatment option for proximal femoral fracture cases complicated by infection [9]. Operative findings from the first-stage surgery – including communication of a sinus tract directly into the joint, extensive fibrinous necrotic tissue, and destruction of the femoral head – highlighted the severity of the infection and near-complete structural compromise of the proximal femur. Following spacer placement, infection control, normalisation of inflammatory markers, and negative aspiration, the patient subsequently underwent revision THA using a long 300-mm tapered fluted revision stem, cerclage fixation, and dual mobility acetabular construct. Tapered fluted stems have been shown to confer good outcomes even in cases of significant bone loss, while dual mobility liners are often recommended in complex revisions due to their low complication rates and increased stability [10,11]. While the patient experienced a post-operative dislocation requiring closed reduction, her reconstruction remained stable and infection-free at follow-up. Post-operative dislocation is a recognised complication of complex proximal femur reconstruction with THA, especially in patients with concomitant infection and multiple prior surgeries [12]. Hip precautions and external bracing were appropriate given her risk profile.
Failure of subtrochanteric femur fixation complicated by early post-operative infection can result in severe proximal femoral bone loss, leaving patients with limited options for reconstruction. This case demonstrates successful eradication of infection and restoration of function using a two-stage approach involving extensive debridement, high-dose static antibiotic spacer placement, and revision THA with long-stem diaphyseal fixation. Despite the technical challenges and risk of complications, staged reconstruction remains an effective management strategy for patients with unsalvageable proximal femur fractures.
When failure of fixation occurs with peri-implant infection after treating subtrochanteric femur fractures, early recognition and transition to a staged reconstruction approach are critical. High-dose antibiotic spacers and diaphyseal-engaging revision stems allow for successful salvage, even in the setting of severe proximal femoral bone loss.
References
- 1. Garrison I, Domingue G, Honeycutt MW. Subtrochanteric femur fractures: Current review of management. EFORT Open Rev 2021;6:145-51. [Google Scholar] [PubMed]
- 2. Panteli M, Vun JS, West RM, Howard A, Pountos I, Giannoudis PV. Subtrochanteric femoral fractures and intramedullary nailing complications: A comparison of two implants. J Orthop Traumatol 2022;23:27. [Google Scholar] [PubMed]
- 3. Willey M, Karam M. Impact of infection on fracture fixation. Orthop Clin North Am 2016;47:357-64. [Google Scholar] [PubMed]
- 4. Duckworth AD, Phillips SA, Stone O, Moran M, Breusch SJ, Biant LC. Deep infection after hip fracture surgery: Predictors of early mortality. Injury2012;43:1182-6. [Google Scholar] [PubMed]
- 5. Lundy DW. Subtrochanteric femoral fractures. J Am Acad Orthop Surg 2007;15:663-71. [Google Scholar] [PubMed]
- 6. Bedi A, Toan Le T. Subtrochanteric femur fractures. Orthop Clin North Am 2004;35:473-83. [Google Scholar] [PubMed]
- 7. Panteli M, Vun JS, West RM, Howard A, Pountos I, Giannoudis PV. Surgical site infection following intramedullary nailing of subtrochanteric femoral fractures. J Clin Med 2021;10:3331. [Google Scholar] [PubMed]
- 8. Hellwinkel JE, Working ZM, Certain L, García AJ, Wenke JC, Bahney CS. The intersection of fracture healing and infection: Orthopaedics research society workshop 2021. J Orthop Res 2022;40:541-52. [Google Scholar] [PubMed]
- 9. Dingemans SA, Sier MAT, Peters RW, Goslings JC, Schepers T. Two-stage treatment in patients with patients with high-energy femoral fractures does not lead to an increase in deep infectious complications: A propensity score analysis. Eur J Trauma Emerg Surg 2018;44:125-31. [Google Scholar] [PubMed]
- 10. Ali E, Howard LC, Neufeld ME, Masri BA. Treatment of femoral bone loss in revision total hip arthroplasty: A clinical practice review. Ann Jt 2024;9:4. [Google Scholar] [PubMed]
- 11. Dubin JA, Bains SS, Chen Z, Hameed D, Moore MC, Mont MA, et al. Single center evaluation of outcomes of modular dual mobility liners during revision total hip arthroplasty: A five-year follow-up. J Orthop 2023;43:75-8. [Google Scholar] [PubMed]
- 12. Xu Q, Wang Q, Zhu J, Lin J, Lu Z, Wang T, et al. Clinical outcomes of proximal femoral reconstruction technique combined with THA in the treatment of high dislocation secondary to septic arthritis: A retrospective single-center study. BMC Musculoskelet Disord 2023;24:732. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Metallosis Following Total Hip Arthroplasty: A Case Report
August 1, 2026 Metallosis Following Total Hip Arthroplasty: A Case Report August 1, 2026 Short-term Outcomes of Impaction Bone Grafting Technique with a Collared Fully Hydroxyapatite-Coated Stem in Revision Total Hip Arthroplasty: A Case Series
August 1, 2026 Short-term Outcomes of Impaction Bone Grafting Technique with a Collared Fully Hydroxyapatite-Coated Stem in Revision Total Hip Arthroplasty: A Case Series August 1, 2026 Outcome of Large-Diameter Jumbo Cups or Acetabular Mesh with Impaction Bone Grafting for Acetabular Defects in Primary and Revision Total Hip Arthroplasty: A Case Series
August 1, 2026 Outcome of Large-Diameter Jumbo Cups or Acetabular Mesh with Impaction Bone Grafting for Acetabular Defects in Primary and Revision Total Hip Arthroplasty: A Case Series July 1, 2026 Custom-Made Monoflange Acetabular Component for Revision Hip Arthroplasty in Paprosky Type IIIA Defect: A Case Report
July 1, 2026 Custom-Made Monoflange Acetabular Component for Revision Hip Arthroplasty in Paprosky Type IIIA Defect: A Case Report