
Combining circumferential fibre augmentation of the medial meniscus with medial open-wedge high tibial osteotomy restores hoop tension and improves extrusion control in varus MMPRT.
Dr. Abbas Bhatia, Department of Orthopaedics, Murup Hospital, 243, 3·15-daero, Masanhappo-gu, Changwon - 51264, South Korea. E-mail: drabbasbhatia@gmail.com
Abstract
Introduction: Medial meniscus posterior root tears (MMPRTs) in varus knees accelerate medial compartment degeneration. While medial open-wedge high tibial osteotomy (MOWHTO) reduces compartmental load, it does not restore meniscal hoop tension. Circumferential fibre augmentation (CFA) may improve meniscal stability and limit extrusion.
Case Report: A 49-year-old female with varus alignment and magnetic resonance imaging (MRI)-confirmed MMPRT underwent single-stage all-inside CFA followed by MOWHTO. Post-operative rehabilitation included protected motion and gradual weight-bearing.
Outcome: At 6 months, the patient showed significant improvement in pain and function, with radiological evidence of osteotomy union, maintained alignment, and a healed posterior root with reduced meniscal extrusion on MRI.
Conclusion: Combining CFA and MOWHTO is feasible and may enhance meniscal stability and load distribution in varus MMPRT. Further studies are required to establish long-term outcomes.
Keywords: Circumferential fiber augmentation, meniscus posterior root tear, high tibial osteotomy, meniscal extrusion.
Medial meniscus posterior root tears (MMPRTs) compromise the circumferential collagen network responsible for hoop tension, resulting in a biomechanical state similar to total meniscectomy. This leads to increased compartmental pressures, rapid cartilage degeneration, and accelerated progression of osteoarthritis [1,2,3]. A recent systematic review further confirmed that varus-aligned knees undergoing MMPRT repair alone carry a heightened risk of persistent meniscal extrusion and inferior radiological outcomes compared with those receiving concomitant realignment. However, the optimal combined surgical strategy remains undefined [4]. In varus-aligned knees, medial open-wedge high tibial osteotomy (MOWHTO) is an established treatment that shifts the mechanical axis laterally to reduce medial loading; however, MOWHTO alone does not address the fundamental loss of hoop tension caused by MMPRTs. Circumferential fibre augmentation (CFA) has emerged as a novel technique designed to restore circumferential integrity by reinforcing the meniscal rim with high-strength suture tape constructs [5]. Early biomechanical studies show superior resistance to elongation and improved extrusion control compared with isolated pullout repair [6]. Despite these advantages, the application of CFA in conjunction with MOWHTO has not previously been reported. This technical note describes a case of simultaneous CFA and MOWHTO in a varus knee with MMPRT, for which reports remain limited in the literature, highlighting the feasibility of the combined approach and its potential advantages in stability, extrusion control, and early post-operative outcomes. The overall surgical strategy is illustrated (Fig. 1).
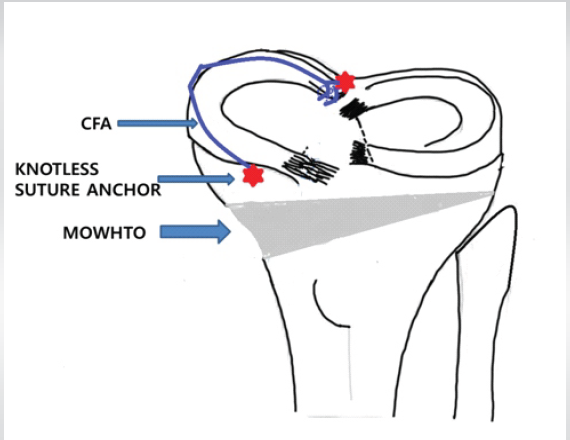
Figure 1: Schematic illustration of medial meniscus posterior root tear (MMPRT) repair using circumferential fiber augmentation combined with medial open-wedge high tibial osteotomy. The diagram demonstrates the MMPRT repaired using a dual-anchor circumferential fiber augmentation construct. Blue represents the circumferential fiber tape used to recreate hoop tension, whereas red indicates the 2.4 mm knotless suture anchors placed at the anterior and posterior horns. The gray region illustrates the open-wedge high tibial osteotomy with plate fixation.
This study, detailing a technical note and case report, was reviewed and approved by the institutional review board of Murup Hospital (Approval No. [MURUP/2025/002]). The patient provided written informed consent for the surgical procedure and for the publication of this case report and accompanying images. A 49-year-old female with a sedentary occupation (body mass index 24 kg/m²) presented with a 1-year history of insidious, gradually worsening medial knee pain, specifically localised to the posteromedial joint line, which was significantly exacerbated by activities involving loading the medial compartment, such as stair climbing and prolonged standing. Physical examination demonstrated palpable tenderness over the posterior medial joint line and a positive MacMurray test (medial side). Pre-operative range of motion (ROM) was 0–120°, with pain limiting deep flexion. Pre-operative functional assessment revealed a Visual Analogue Scale (VAS) pain score of 8, a Lysholm score of 58, an International Knee Documentation Committee (IKDC) score of 68, and a Knee Injury and Osteoarthritis Outcome Score (KOOS)-Pain score of 72. Standing long-leg radiographs confirmed a mechanical axis deviation (MAD), showing significant varus alignment (MAD of 12 mm medial to the centre of the knee). The femorotibial angle was 182°, the medial proximal tibial angle was 89°, and the posterior tibial slope was 10°. Radiographic evaluation noted Kellgren–Lawrence grade 2 osteoarthritis in the medial compartment. Magnetic resonance imaging (MRI) confirmed a complete MMPRT at the tibial insertion, accompanied by a >3 mm meniscal extrusion from the edge of the tibial plateau (Fig. 2).
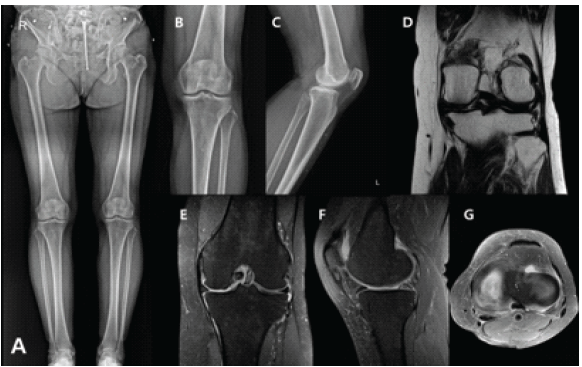
Figure 2: Pre-operative imaging. (a) Scanogram showing varus alignment. (b and c) Standing anteroposterior and lateral radiograph demonstrating medial joint-space narrowing. (d, e, f, g, and h) Magnetic resonance imaging showing posterior root tear of the medial meniscus, submeniscal cleft sign, meniscal extrusion, and superficial medial collateral ligament detachment.
Surgical procedure and technique:
Surgical planning aimed to correct the mechanical axis to the optimal weight-bearing line, positioned at 62% lateral to the medial edge of the tibial plateau, which necessitated a calculated opening wedge of 6 mm. This was performed using the Miniaci method, with the desired weight-bearing line passing through the Fujisawa point. The correction angle was derived by connecting the centre of the femoral head to the target point on the tibial plateau and extending a line from the ankle centre, allowing calculation of the required wedge size [7]. Under general anaesthesia, the procedure commenced with diagnostic arthroscopy. Standard anterolateral viewing and anteromedial working portals were established adjacent to the patellar tendon. A posteromedial portal was created under direct visualisation using transillumination to facilitate safe anchor placement in the posterior root. This confirmed the radial tear at the MMPRT insertion and a complex longitudinal tear extending into the midbody of the medial meniscus.
CFA:
This was performed using an all-inside, knotless dual-anchor technique to restore hoop tension:
- Fibre tape passage: To pass the high-strength suture tape circumferentially through the meniscal substance, a sequential guide system was used. A spinal needle was first passed from the anterior horn, traversing the meniscal body. A Nitinol wire loop (Arthrex or equivalent) was used as a shuttle to pass a 2-mm UHMWPE fibre tape circumferentially through the meniscus (Fig. 3a, b, c, d, e, f).
- Posterior fixation: Posterior fixation was achieved using a 2.6-mm knotless suture anchor (e.g., FiberTak/PushLock or equivalent) inserted through the posteromedial portal at the native root footprint. Care was taken to avoid iatrogenic cartilage injury during posterior anchor insertion by maintaining appropriate portal trajectory and knee positioning.
- Anterior fixation: The remaining end of the fibre tape was brought to the anterior horn. Final tensioning was performed under arthroscopic visualisation to ensure restoration of meniscal contour and reduction of extrusion without overconstraint. The construct was secured using a second 2.6-mm knotless anchor at the anterior horn, with appropriate tension applied to restore circumferential stability (Fig. 3g). Arthroscopic probing confirmed stable meniscal fixation and reduction of the meniscal extrusion.
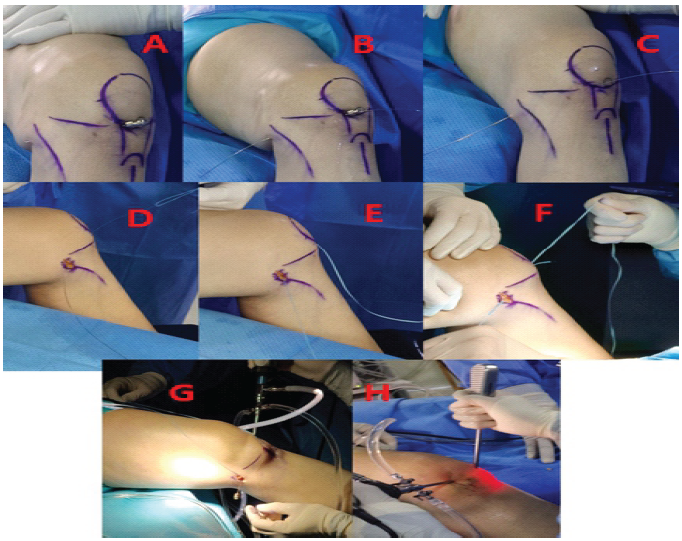
Figure 3: Intraoperative images (a) Spinal needle passed through the anterior horn and body of the medial meniscus. (b and c) The guide wire passed along the same tract. (d) Nitinol wire introduced through the guide wire path. (e) Suture thread shuttled through the Nitinol wire. (f) Fiber tape passed through the suture thread to complete the circumferential passage. (g) Via a posteromedial portal, posterior knotless anchor fixation was performed after taking bites in the posterior root of the medial meniscus. (h) Anterior traction applied to the fiber tape and fixed with a knotless suture anchor at the anterior horn, completing the circumferential construct.
MOWHATO:
Immediately following CFA, the MOWHTO was performed. A skin incision was made over the medial proximal tibia. The osteotomy began distal to the tibial tubercle and was carefully initiated at the medial cortex using an oscillating saw. It extended laterally under fluoroscopic guidance toward the lateral hinge, leaving a critical 10 mm lateral cortical bridge intact. The gap was opened using sequential osteotomes to a predetermined size of 6 mm. The final correction angle was verified intraoperatively using alignment rods and confirmed through C-arm imaging. The open gap was supported using a non-resorbable 6 mm beta-TCP wedge for stability and was supplemented with an ipsilateral distal femoral autograft (from the planned plate fixation site). Fixation was achieved with a TomoFix plate and screws, ensuring rigid stability of the osteotomy (Fig. 4).
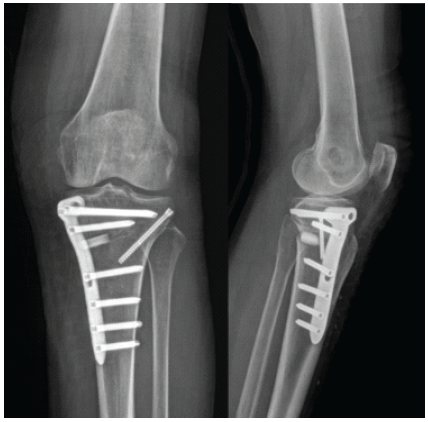
Figure 4: Post-operative imaging (Immediate). Anteroposterior and lateral radiographs.
Post-operative course and outcome:
Postoperatively, the patient received thromboprophylaxis with oral aspirin (75 mg once daily) for 2 weeks, along with mechanical prophylaxis using compression stockings. Post-operative management included strict non-weight-bearing for 6 weeks, protected ROM with controlled flexion limited to 90° by week 4, and gradual progression to full weight-bearing starting between 8 and 10 weeks. Subsequently, strengthening exercises focusing on quadriceps and hamstring conditioning were initiated, along with proprioceptive training. Return to full functional activities was allowed at approximately 3–4 months, depending on clinical and radiological progression. At the 6-month follow-up, the patient reported substantial clinical improvement. She was walking without a limp or support and could manage stairs comfortably. Subjective scores showed significant improvement: the VAS pain score decreased from 8 preoperatively to 2, the Lysholm score improved from 58 to 94, the IKDC score from 68 to 91, and the KOOS-Pain score from 72 to 88. Post-operative radiographs confirmed osteotomy union, maintained axis correction, and proper plate fixation. MRI at 6 months demonstrated continuity of the medial meniscus posterior root, reduced meniscal extrusion compared to the preoperative state, and stable, intact anchor positioning (Fig. 5).
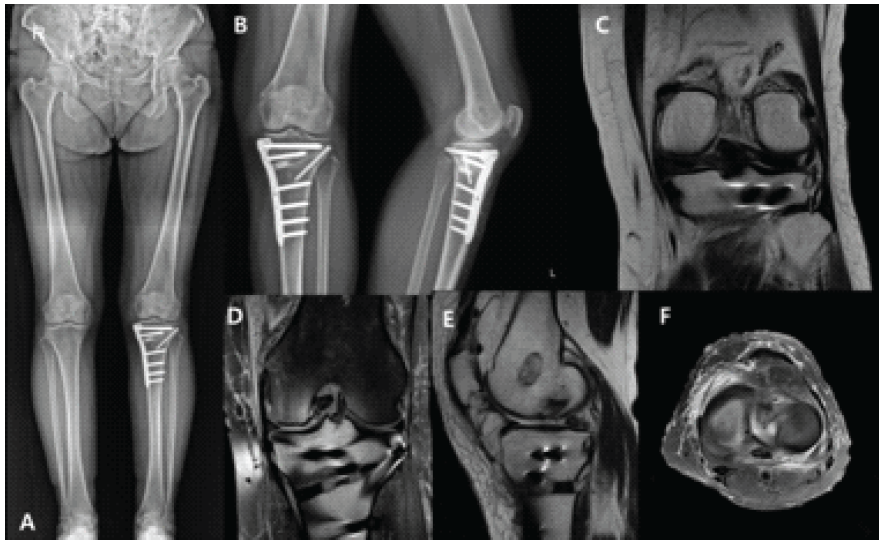
Figure 5: Six months post-operative imaging. (a) Scanogram showing a neutral mechanical axis after medial open-wedge high tibial osteotomy + circumferential fiber augmentation. (b) Anteroposterior and lateral radiographs showing maintained correction and osteotomy healing. (c, d, e, and f) Coronal and sagittal magnetic resonance imaging demonstrating decreased meniscal extrusion and intact anterior and posterior anchors at 6 months.
MMPRTs disrupt circumferential collagen bundles, resulting in a 25–30% increase in medial contact pressure and rapid cartilage degeneration [1,5]. Transtibial pullout repair restores the root attachment but fails to re-establish full hoop tension, resulting in persistent extrusion and incomplete load transmission [2,5]. CFA was developed to reinforce circumferential continuity using ultra-high-molecular-weight polyethylene (UHMWPE) tapes, which resist elongation and maintain tension across the meniscus under compression [1,6]. Kita et al. first demonstrated biomechanical advantages of CFA constructs in cadaveric models, showing improved fixation stiffness and reduced extrusion [6]. Kodama et al. subsequently integrated CFA with transtibial pullout repair and reported improved tension distribution without meniscal tissue cutout [5]. This case represents the first application of CFA combined with MOWHTO, addressing both biological and mechanical aspects of MMPRT management. An additional practical advantage of this technique is the avoidance of transtibial tunnels. The dual-anchor CFA allowed for fixation without the need for transtibial tunnels, which can interfere with the osteotomy plane during MOWHTO and compromise both tunnel integrity and osteotomy stability. Previous studies on concurrent MMPRT repair and MOWHTO using only pullout techniques have shown extrusion persistence and suboptimal hoop stress recovery [8,9]. In contrast, our combined approach provided circumferential load reinforcement, potentially reducing the risk of post-operative meniscal extrusion and recurrent overload on the corrected axis. The simultaneous correction of the mechanical axis via MOWHTO and the restoration of hoop tension through CFA create a synergistic biomechanical environment. Traditional transtibial pullout repair, while addressing the root attachment, often fails in the context of persistent varus alignment due to sustained high compressive loads on the fragile repair site. The tape augmentation offers superior resistance to stretching and load dissipation, thereby protecting the healing root and effectively controlling medial extrusion – a critical predictor of failure [2,10]. This dual intervention not only unloads the compromised medial compartment but also provides a mechanically reinforced meniscal structure capable of effectively translating the remaining loads to the newly aligned joint surface. This protective mechanism is vital for long-term cartilage survival. Recent biomechanical and imaging data suggest that residual extrusion following MMPRT repair is a key determinant of clinical outcome [2,10]. By integrating CFA, extrusion control may be optimised, improving joint-space preservation. Moreover, MOWHTO increases intra-articular pressure redistribution toward the lateral compartment, complementing the reinforced medial meniscus. Notably, a recent meta-analysis of 725 patients demonstrated that combined HTO and meniscal root repair yielded significantly superior IKDC and Hospital for Special Surgery scores compared with high tibial osteotomy alone, underscoring the functional benefit of addressing hoop tension alongside mechanical realignment [11]. Early radiologic outcomes in our case confirmed meniscal integrity, reduced extrusion, and osteotomy union – all findings that align with previously reported biomechanical predictions [1,3,6] (Fig. 5). The combined technique carries limitations, including increased operative complexity and a potential learning curve. However, in select patients with varus alignment and root tears, the synergy between CFA and MOWHTO may provide superior load sharing and repair protection. Long-term comparative studies and biomechanical models are needed to validate this dual-intervention concept.
Simultaneous CFA and MOWHTO are technically feasible and may enhance meniscal stability and healing in varus knees with posterior root tears. This combined approach offers a biomechanically sound alternative for complex cases where traditional pullout repair alone may be insufficient.
Isolated high tibial osteotomy or root repair may be insufficient in varus-aligned MMPRT because hoop tension restoration and extrusion control remain suboptimal. A single-stage combination of circumferential fibre augmentation and medial open-wedge high tibial osteotomy provides a biomechanically complementary strategy that protects the repaired root and optimises load sharing in selected patients.
References
- 1. Familiari F, Chahla J, Compagnoni R, DePhillipo NN, Moatshe G, LaPrade RF, et al. Meniscal extrusion consensus statement: MenIN Study Group. Knee Surg Sports Traumatol Arthrosc 2024;32:1446-54. [Google Scholar] [PubMed]
- 2. Kawada K, Furumatsu T, Tamura M, Xue H, Higashihara N, Kintaka K, et al. Medial joint space narrowing progresses after pullout repair of medial meniscus posterior root tear. Int Orthop 2023;47:2401-7. [Google Scholar] [PubMed]
- 3. Perry AK, Lavoie-Gagne O, Knapik DM, Maheshwer B, Hodakowski A, Gursoy S, et al. Examining the efficacy of medial meniscus posterior root repair: A meta-analysis and systematic review of biomechanical and clinical outcomes. Am J Sports Med 2023;51:1914-26. [Google Scholar] [PubMed]
- 4. Wang H, Man Q, Gao Y, Xu L, Zhang J, Ma Y, et al. The efficacy of medial meniscal posterior root tear repair with or without high tibial osteotomy: A systematic review. BMC Musculoskelet Disord 2023;24:464. [Google Scholar] [PubMed]
- 5. Kodama Y, Masuda S, Yokomizo D, Ohmori T, Tanaka M. Circumferential fiber augmentation technique combined with transtibial pullout repair. Arthrosc Tech 2024;13:103132. [Google Scholar] [PubMed]
- 6. Kita K, Kusano M, Tsujii A, Ohori T, Tanaka Y, Nakamura N, et al. Meniscal circumferential fiber augmentation: A biomechanical arthroscopic meniscal repair technique. Arthrosc Tech 2023;12:e1673-8. [Google Scholar] [PubMed]
- 7. Cheng X, Liu F, Xiong F, Huang Y, Paulus AC. Radiographic changes and clinical outcomes after open and closed wedge high tibial osteotomy: a systematic review and meta-analysis. J Orthop Surg Res. 2019 Jun 14;14(1):179. doi: 10.1186/s13018-019-1222-x. PMID: 31200743; PMCID: PMC6570851. [Google Scholar] [PubMed] [CrossRef]
- 8. Vosoughi F, Vahedi P, Nakhjiri MT, Keyhani S, Soleymanha M, LaPrade R, Tollefson LV, Oskouie IM. High tibial osteotomy and concurrent medial meniscus root repair provides improved objective outcomes compared to high tibial osteotomy alone for knee osteoarthritis: A systematic review. Knee Surg Sports Traumatol Arthrosc. 2025 Sep;33(9):3361-3374. doi: 10.1002/ksa.12796. Epub 2025 Jul 18. PMID: 40679279. [Google Scholar] [PubMed] [CrossRef]
- 9. Okamura H, Ishikawa H, Ohno T, Fujita S, Yamamoto S, Yamakami S, Nagasaki K, Kudo Y. Medial Meniscus Posterior Root Reconstruction and Open-Wedge High-Tibial Osteotomy for Medial Meniscus Posterior Root Tear With Varus Knee Alignment: A Retrospective Study on Short-Term Outcomes. Cureus. 2024 Mar 29;16(3):e57170. doi: 10.7759/cureus.57170. PMID: 38681336; PMCID: PMC11056034. [Google Scholar] [PubMed] [CrossRef]
- 10. Furumatsu T, Kodama Y, Kamatsuki Y, Hino T, Okazaki Y, Ozaki T. Meniscal Extrusion Progresses Shortly after the Medial Meniscus Posterior Root Tear. Knee Surg Relat Res. 2017 Dec 1;29(4):295-301. doi: 10.5792/ksrr.17.027. PMID: 29172390; PMCID: PMC5718799. [Google Scholar] [PubMed] [CrossRef]
- 11. Ade-Conde AM, Cruickshank M, Bouchard MD, Vivekanantha P, Meena A, Malik SS, et al. Combined high tibial osteotomy and root repair improves patient-reported outcomes in medial meniscus posterior root tears: A systematic review and meta-analysis. J ISAKOS 2026;16;101035. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Pes Anserinus and Superficial Medial Collateral Ligament Preserving High Tibial Osteotomy Combined with Arthroscopic Medial Meniscus Root Repair for Medial Compartment Osteoarthritis with Varus Deformity: A Prospective Case Series of 20 Patients
June 1, 2026 Pes Anserinus and Superficial Medial Collateral Ligament Preserving High Tibial Osteotomy Combined with Arthroscopic Medial Meniscus Root Repair for Medial Compartment Osteoarthritis with Varus Deformity: A Prospective Case Series of 20 Patients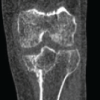 June 1, 2026 Restoration of Limb Alignment in Post-Traumatic Genu Varum Case Using Medial Open Wedge Proximal Tibial Osteotomy with Posterior Tibial Slope Correction: A Case Report
June 1, 2026 Restoration of Limb Alignment in Post-Traumatic Genu Varum Case Using Medial Open Wedge Proximal Tibial Osteotomy with Posterior Tibial Slope Correction: A Case Report February 1, 2026 Outcome of Medial Open Wedge High Tibial Osteotomy for Knee Osteoarthritis: A Case Series
February 1, 2026 Outcome of Medial Open Wedge High Tibial Osteotomy for Knee Osteoarthritis: A Case Series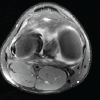 December 1, 2025 Biomechanical Reinforcement of a Bucket-handle Lateral Meniscus Tear Using Circumferential Fiber Augmentation: A Case Report
December 1, 2025 Biomechanical Reinforcement of a Bucket-handle Lateral Meniscus Tear Using Circumferential Fiber Augmentation: A Case Report