
Combined high tibial osteotomy and medial meniscus posterior root repair helps restore limb alignment and meniscal function, providing improved biomechanics and satisfactory clinical outcomes in selected patients with varus knee osteoarthritis.
Dr. Jaideep Das, Department of Orthopaedics, Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra, India. E-mail: jaideepdas01@gmail.com
Abstract
Introduction: Medial compartment osteoarthritis associated with varus malalignment is frequently compounded by medial meniscus root tears, resulting in altered knee biomechanics and accelerated cartilage degeneration. While high tibial osteotomy (HTO) corrects mechanical alignment, medial meniscus root repair restores hoop stress and meniscal function. A combined approach may provide superior biomechanical restoration.
Case Series: This prospective case series includes 20 patients with symptomatic medial compartment osteoarthritis, varus deformity, and magnetic resonance imaging-confirmed medial meniscus root tear treated with combined medial opening wedge HTO and arthroscopic root repair using a pes anserinus and superficial medial collateral ligament preserving technique.
Results: : At a mean follow-up of 20 months, significant improvement was observed in functional outcomes. The Knee Society Score improved from a mean of 52.4 pre-operatively to 88.2 post-operatively, while the Oxford Knee Score improved from 21.8 to 40.2. The mean correction angle achieved was 9.8°, with values extending up to 12–13° in selected patients, and radiological union was achieved in all patients at a mean of 14.2 weeks. Complications were minimal and self-limiting.
Conclusion: A combined medial opening wedge HTO with medial meniscus posterior root repair appears to provide satisfactory functional and radiological outcomes in appropriately selected patients.
Keywords: High tibial osteotomy, medial meniscus root tear, varus knee, osteoarthritis, joint preservation.
Medial compartment osteoarthritis of the knee is closely associated with varus malalignment, which results in disproportionate load transmission across the medial tibiofemoral compartment and progressive cartilage degeneration [1]. The presence of a medial meniscus posterior root tear further aggravates this condition by disrupting the circumferential hoop stress mechanism, thereby increasing contact pressures and accelerating joint degeneration [2,3]. High tibial osteotomy has been widely accepted as an effective joint-preserving procedure that realigns the mechanical axis of the lower limb and redistributes load toward the relatively preserved lateral compartment. [4,5,6] However, correction of alignment alone does not fully restore intra-articular biomechanics in the presence of meniscal insufficiency. Persistent abnormal contact stresses may continue to drive disease progression. Recent advances in knee preservation surgery emphasise the importance of addressing both extra-articular alignment and intra-articular pathology. Repair of the medial meniscus posterior root has been shown to restore hoop stress and improve load distribution. Therefore, combining high tibial osteotomy (HTO) with root repair provides a comprehensive approach aimed at restoring near-normal knee biomechanics [4]. The purpose of this study is to evaluate the clinical and radiological outcomes of combined medial opening wedge HTO and medial meniscus posterior root repair in patients with varus knee osteoarthritis. To the best of our knowledge, literature focuses on pes anserinus and superficial medial collateral ligament (sMCL) preserving techniques in combined procedures remains limited, although pes anserinus-preserving HTO techniques have recently been described [1,5].
This prospective case series was conducted at a tertiary care centre between 2021 and 2024. Twenty patients meeting predefined inclusion criteria were enrolled. Patients were between 30 and 60 years of age; had symptomatic medial compartment osteoarthritis classified as Kellgren–Lawrence Grade II or III; demonstrated varus deformity not exceeding 15°; and had magnetic resonance imaging (MRI) evidence of a medial meniscus posterior root tear. Patients with tricompartmental osteoarthritis, inflammatory arthritis, or significant flexion contracture were excluded. All patients underwent standardised pre-operative clinical evaluation using the Knee Society Score and Oxford Knee Score. Radiological evaluation included full-length weight-bearing radiographs to assess limb alignment and plan deformity correction. Patients were followed up at regular intervals with both clinical and radiological assessment. The study included patients between 30 and 60 years of age who presented with symptomatic medial compartment osteoarthritis classified as Kellgren–Lawrence Grade II or III, associated with varus malalignment of 15° or less. All patients had an intact lateral compartment with cartilage status not exceeding Outerbridge Grade II, maintained a functional range of motion of more than 100°, and demonstrated a medial meniscus root tear confirmed on MRI. In addition, only patients with a stable knee or those with correctable ligamentous laxity were considered suitable candidates for inclusion. Patients were excluded if they had tricompartmental osteoarthritis or involvement of the lateral compartment, as well as in cases of inflammatory arthritis. Individuals with fixed varus deformity >15°, severe flexion contracture exceeding 10°, or significant ligament instability, particularly uncorrected lateral laxity, were not included in the study. Furthermore, patients with a history of prior knee osteotomy, previous infection, or those presenting with isolated varus deformity without an associated medial meniscus root tear were excluded. Statistical analysis was performed using a paired t-test to compare pre-operative and postoperative functional scores. A P < 0.05 was considered statistically significant.
Ethical statement:
Ethical approval was not required for this study in accordance with institutional guidelines. The study was performed in accordance with the ethical standards of the Declaration of Helsinki.
A 45-year-old male patient presented with complaints of progressively increasing pain in the medial aspect of the right knee for the past 2 years, associated with difficulty in walking long distances and squatting. There was no history of significant trauma. Clinical examination revealed varus alignment of the knee with tenderness along the medial joint line and painful terminal flexion. Range of motion was 0°–110°. Ligamentous examination showed a stable knee with correctable varus deformity. Pre-operative weight-bearing radiographs of the lower limb demonstrated varus malalignment with medial compartment joint space narrowing consistent with Kellgren–Lawrence Grade II osteoarthritis. The mechanical axis passed medial to the centre of the knee joint (Fig. 1).
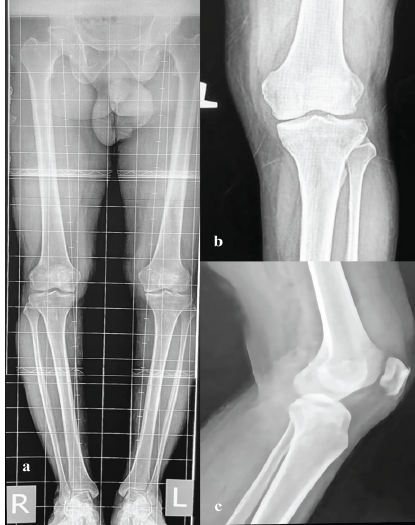
Figure 1: Pre-operative bilateral knee standing scanogram and X-rays. (a) Pre-operative scanogram showing left knee medial compartment osteoarthritis with varus deformity, (b) Pre-operative left knee X-ray anteroposterior view, (c) Pre-operative left knee X-ray lateral view.
Magnetic resonance imaging confirmed a root tear of the medial meniscus, with associated meniscal extrusion and early chondral changes in the medial compartment, while the lateral compartment cartilage was preserved (Fig. 2). Based on clinical and radiological findings, the patient was planned for a combined medial opening wedge HTO with arthroscopic medial meniscus root repair.
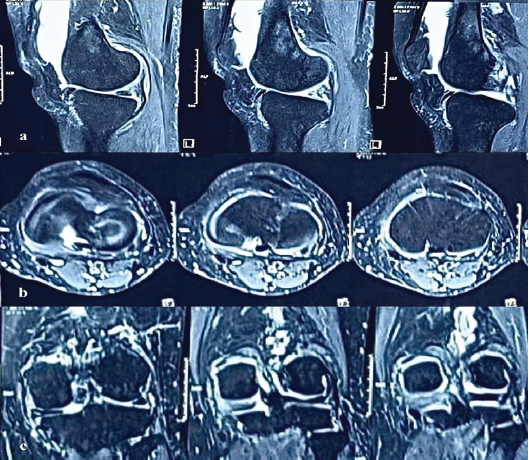
Figure 2: Pre-operative magnetic resonance imaging (MRI) left knee showing a medial meniscus tear. (a) MRI left knee sagittal view, (b) MRI left knee axial view, (c) MRI left knee coronal view.
Preoperative planning:
Pre-operative planning was performed using long-leg standing radiographs with the aim of shifting the post-operative mechanical axis to pass through 60–70% of the lateral tibial plateau, corresponding to the Fujisawa point (Fig. 3a). [7,8,9] The correction angle was calculated using the Miniaci method. [7] The mechanical axis of the femur was drawn from the centre of the femoral head to the centre of the knee joint, while the mechanical axis of the tibia was drawn from the centre of the ankle to the knee. A target line was then drawn from the femoral head to the desired weight-bearing point on the lateral tibial plateau. The hinge point was identified at the lateral cortex just above the proximal tibiofibular joint. From this hinge point, one line was drawn to the centre of the ankle, representing the pre-operative axis, and another line was drawn to the target point, representing the desired post-operative axis. The angle formed between these lines represented the required correction angle (Fig. 3b).
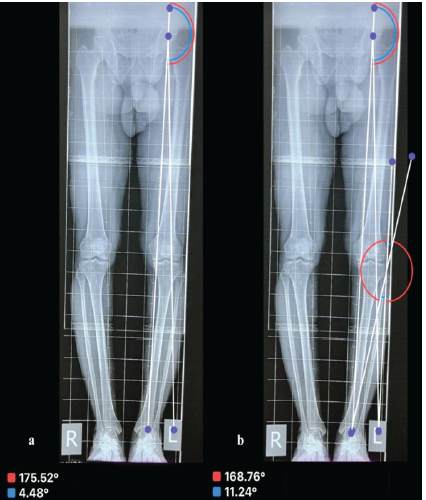
Figure 3: Pre-operative planning over scanogram. (a) Lines drawn through the mechanical axis and the Fujisawa point, (b) calculation of the angle of correction/osteotomy of 11°.
This angular correction was translated into an opening wedge distance at the osteotomy site using geometric planning. [8] An isosceles triangle was constructed with the hinge point as the apex and the base representing the osteotomy gap. An additional allowance of approximately 1 mm was added to compensate for bone loss due to the oscillating saw, thereby minimising the risk of undercorrection. Pre-operative assessment also included evaluation of lateral compartment laxity using valgus stress testing and measurement of the joint line convergence angle. In patients with increased lateral laxity, the planned correction was reduced by approximately 1–2° to avoid overcorrection and excessive valgus alignment. Accordingly, the target mechanical axis was adjusted to pass through 55–60% of the tibial plateau instead of the standard Fujisawa point. All procedures were performed with the patient in the supine position under spinal or general anaesthesia. A longitudinal incision was made over the anteromedial aspect of the proximal tibia, corresponding to the junction of the anterior two-thirds and posterior one-third, approximately 10 cm distal to the medial joint line. Following careful subcutaneous and fatty tissue dissection, the sartorial fascia was incised proximally, and the pes anserinus was identified. The pes was split longitudinally to facilitate atraumatic retraction both anteriorly and posteriorly, thereby preserving its structural integrity. Attention was then directed toward preservation of the sMCL. The tibial footprint of the sMCL, located approximately 5–7 cm distal to the medial joint line along the posteromedial aspect of the proximal tibia, was carefully identified, and a controlled rent of approximately 10 mm was created at its insertion. Through this window, a small curved AO periosteal elevator was introduced, and the medial and posterior surfaces of the sMCL and other soft tissue at the posterior tibial surface were carefully cleared in a subperiosteal plane without complete detachment. This created a safe working space while maintaining ligament integrity. A posterior spike retractor was placed within this plane to protect the posterior neurovascular and soft-tissue structures throughout the procedure. Following completion of the initial exposure, the tourniquet was inflated, and arthroscopy was performed using standard anteromedial and anterolateral portals. After a systematic diagnostic evaluation, the medial meniscus root tear was identified. A suture bite was taken using a Scorpion suture passer loaded with 2 mm FiberWire. In half of the patients, fixation was performed using a luggage tag knot configuration, while in the remaining patients a sliding knot technique was utilised to secure the meniscal tissue. A transtibial tunnel for root repair was then created from the anteromedial surface of the tibia, with the entry point located approximately 3 cm distal to the medial joint line (Fig. 4b). The tunnel was drilled at an angle of approximately 45° in both the coronal and sagittal planes using a 4 mm drill bit till the exit point (Fig. 4d).
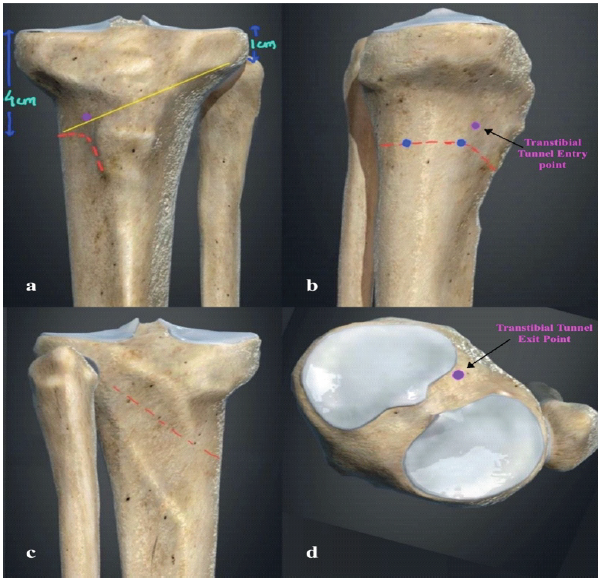
Figure 4: 3D tibia-fibula showing site and plane of osteotomy with transtibial tunnel. (a) Tibia-fibula anteroposterior view with red dotted line shows site of osteotomy, yellow line shows plane of osteotomy directed towards fibula head, (b) Tibia medial view with red dotted line shows site of osteotomy, blue dots as initial guide K-wires, purple dot showing entry of transtibial tunnel, (c) Tibia-fibula posterior view showing direction of osteotomy, (d) Tibia-fibula top view with purple dot showing exit of transtibial tunnel.
A nitinol passing wire was passed through the tunnel, and the FiberWire sutures were retrieved through the tunnel. The drill bit was then reversely placed temporarily within the tunnel to protect the FiberWire sutures during the subsequent osteotomy procedure (Fig. 5a). Subsequently, a biplanar medial opening wedge HTO was performed approximately 4 cm distal to the medial joint line (Fig. 4a). [5,10] Two guide K-wires (1.2 mm) were inserted from the anteromedial tibial surface, one in the anterior one-third and the other in the posterior two-thirds, both directed toward the tip of the fibula (Fig. 4a and b, c, 5b). These guide wires defined the osteotomy plane and were connected using a small oscillating saw. An additional hinge wire was placed parallel to the lateral cortex to preserve and support the lateral cortical hinge (Fig. 5c). The osteotomy cut was directed anteriorly just below the tibial tuberosity to preserve the extensor mechanism (Fig. 4a and b). The posterior cortex was carefully completed using a saw while protecting the posterior soft-tissue structures, particularly near the lateral posterior cortex of the tibia. Gradual opening of the osteotomy was achieved using sequential osteotomes (Fig. 5c and d). The preoperatively calculated correction angle was verified intraoperatively using an angle guide introduced into the osteotomy site and advanced toward the hinge point. The osteotomy was progressively opened until the desired correction angle was achieved (Fig. 5f). Before fixation, proper alignment was checked under fluoroscopy. (Fig. 5e, g).

Figure 5: Intraoperative clinical pictures and C-arm images of the procedure. (a) Intraoperative clinical pictures of exposure, (b-g,i) Intraoperative C-arm images of procedure in sequence, (h) Intraoperative clinical picture showing plate beneath pes anserinus.
Fixation was then performed using a 3- or 4-hole medial locking plate. The plate was positioned under fluoroscopic (C-arm) guidance. A 4 mm drill was passed through the central hole, which was initially occupied by the previously placed drill bit. A distal locking screw was first inserted near the osteotomy site, followed by placement of two proximal locking screws and subsequently two additional distal locking screws to achieve stable fixation. The central drill bit was then replaced with a locking screw. Finally, the drill bit used for tunnel preparation was removed, and the FiberWire sutures were retrieved and secured over a suture disc or directly tied over a plate on the anterior tibial cortex, completing the medial meniscus posterior root repair. The wound was closed in layers, and a sterile dressing was applied (Fig. 5h and i). Postoperatively, patients were mobilised with nil weight bearing for the first 6 weeks. Gradual mobilisation was then initiated with partial weight bearing after 6 weeks, progressing to full weight bearing at 12 weeks (Fig. 6). The same surgical protocol was followed in the remaining 19 patients with comparable intraoperative steps and post-operative rehabilitation.
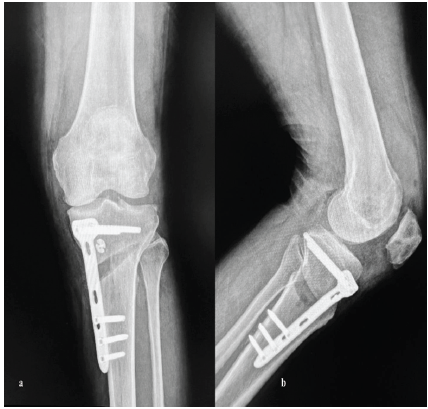
Figure 6: Immediate post-operative X-rays. (a) X-ray left knee anteroposterior view, (b) X-ray left knee lateral view.
The study included 20 patients with a mean age of 46.9 years. At a mean follow-up of 20 months, significant improvement was observed in functional outcomes. The Knee Society Score improved from a mean of 52.4 preoperatively to 88.2 postoperatively, while the Oxford Knee Score improved from 21.8 to 40. 2. Range of motion also showed improvement from a mean of 106° to 124° (Table 1).
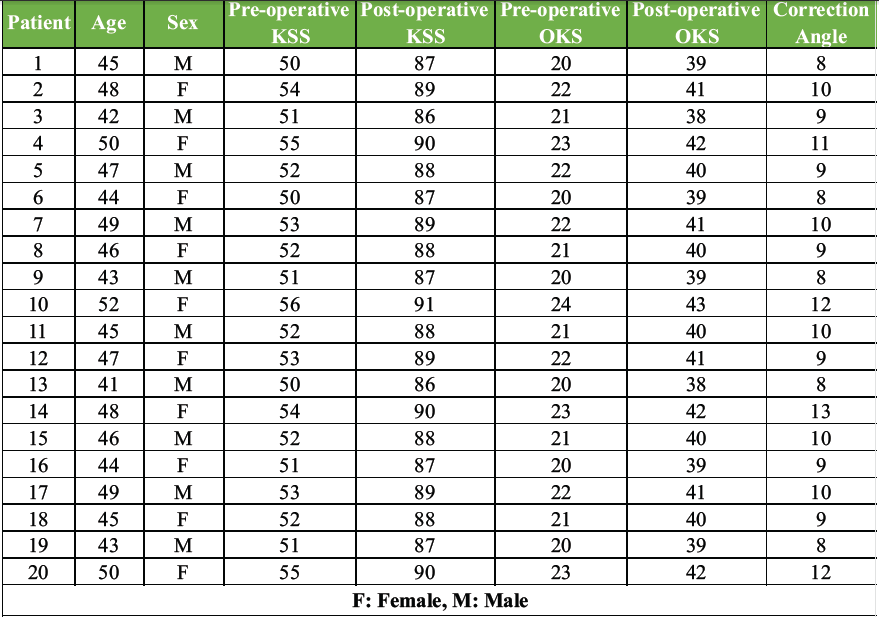
Table 1: Demographic, clinical, and radiological outcomes of patients undergoing combined medial opening wedge high tibial osteotomy with medial meniscus posterior root repair. Pre-operative and post-operative functional scores, including Knee Society Score (KSS) and Oxford Knee Score (OKS), along with the achieved correction angle for each patient, are presented
These improvements in functional scores were found to be statistically significant (P < 0.001). Radiological evaluation demonstrated a mean correction angle of 9.8°, with a range extending up to 12–13° in selected patients with higher preoperativevarus deformity. Post-operative alignment achieved slight valgus positioning in all cases. All osteotomies achieved union at a mean duration of 14.2 weeks (Fig. 7).

Figure 7: 9 Months follow-up X-rays and Scanogram. (a) X-ray left knee anteroposterior view, (b) X-ray left knee lateral view, (c) Bilateral knee standing scanogram.
Complications were minimal, with one case of superficial infection managed conservatively and two cases of transient saphenous nerve paraesthesia that resolved spontaneously. No cases of non-union, implant failure, or loss of correction were observed.
The achieved postoperative alignment in our series is comparable to previous studies demonstrating the influence of limb alignment on clinical outcome after open-wedge HTO [6]. The present study demonstrates that a combined medial opening wedge HTO with medial meniscus posterior root repair results in significant improvement in both functional and radiological outcomes. In our series, the Knee Society Score improved from 52.4 preoperatively to 88.2 postoperatively, while the Oxford Knee Score improved from 21.8 to 40.2, indicating substantial functional recovery. These findings are comparable to those reported by Feucht et al., who observed significant improvement in clinical scores following transtibial medial meniscus root repair, with Lysholm scores improving from approximately 54 to 85 at final follow-up [4]. Similarly, Bode et al. reported favourable mid-term outcomes following HTO, with survival rates exceeding 85% at 5 years [11,12,13]. Recent literature supports the advantage of combined procedures addressing both coronal alignment and meniscal function restoration. Biomechanical and clinical studies have demonstrated that correction of varus alignment, together with medial meniscus root repair, improves load distribution, restores hoop stress, and may reduce progression of medial compartment degeneration. Radiologically, our study achieved a mean correction angle of 9.8°, with successful union in 100% of cases at a mean duration of 14.2 weeks. These results are consistent with those reported by Takeuchi et al., who demonstrated reliable union rates within 12–16 weeks following medial opening wedge HTO [11]. Furthermore, the ability to safely achieve higher correction angles (up to 12–13° in selected patients) without compromising outcomes is in agreement with findings from Schröter et al., who emphasised the importance of individualised correction planning [12]. Biomechanically, medial meniscus posterior root tears have been shown to increase tibiofemoral contact pressures comparable to total meniscectomy, as demonstrated by Allaire et al. [2]. This underscores the importance of root repair in restoring hoop stress. Our results support this concept, as combined correction of alignment and restoration of meniscal function resulted in improved clinical outcomes and absence of disease progression during follow-up. An important technical aspect of this study is the preservation of the pes anserinus and sMCL. Previous studies, such as those by Lee et al., have demonstrated improved stability and enhanced healing with preservation techniques [14]. Our findings further validate this approach, with a 100% union rate and absence of instability-related complications. [15]. Compared to previously published literature, the present study demonstrated consistent correction, satisfactory functional improvement, and minimal complications. The absence of major complications such as non-union, implant failure, or loss of correction highlights the safety and reproducibility of the procedure. However, biological healing of the repaired meniscal root could not be objectively confirmed in all patients because post-operative MRI evaluation was not routinely performed.
Limitations:
The present study has several limitations. First, the sample size was relatively small, consisting of only 20 patients, which limits the generalisability of the findings. Second, this was a prospective case series without a randomised control group; therefore, direct comparison with isolated HTO or isolated medial meniscus root repair could not be performed. The follow-up duration was relatively short, preventing assessment of long-term survivorship, durability of correction, and progression of osteoarthritis. Functional outcomes were primarily evaluated using validated clinical scoring systems, while objective biomechanical assessments, such as gait analysis, were not performed. Post-operative MRI to evaluate meniscal healing was not routinely obtained in all patients, and second-look arthroscopic assessment was not undertaken to confirm biological healing of the repaired root. The study was conducted at a single tertiary care centre, which may introduce institutional bias. In addition, all procedures were performed by experienced surgeons, and therefore, reproducibility of outcomes among less experienced surgeons remains uncertain. Selection bias may also be present because only carefully selected patients with preserved lateral compartments, limited deformity, and relatively early osteoarthritis were included in the study. Consequently, the applicability of this technique to patients with advanced osteoarthritis, inflammatory arthritis, severe deformity, or major ligament instability remains limited. Furthermore, the influence of different root repair configurations, cartilage status, degree of meniscal extrusion, and pre-operative ligament laxity on post-operative outcomes was not analysed separately. Post-operative rehabilitation compliance was also not objectively assessed and may have influenced functional recovery. Radiological evaluation mainly focused on correction and osteotomy union without detailed quantitative cartilage assessment. Therefore, larger multicentric randomised comparative studies with longer follow-up are required to further validate the reproducibility, long-term durability, and superiority of this combined joint-preserving procedure.
Combined medial opening wedge HTO with medial meniscus posterior root repair appears to be a safe and effective joint-preserving procedure that provides satisfactory functional and radiological outcomes in appropriately selected patients.
In patients with varus knee osteoarthritis and a medial meniscus posterior root tear, simultaneous correction of mechanical alignment and restoration of meniscal integrity is essential. A combined approach using high tibial osteotomy and root repair provides superior biomechanical restoration and should be considered in appropriately selected patients.
References
- 1. Noyes FR, Barber-Westin SD. High tibial osteotomy for varus gonarthrosis: Indications and technique. J Bone Joint Surg Am 2010;92:1316-32. [Google Scholar] [PubMed]
- 2. Allaire R, Muriuki M, Gilbertson L, Harner CD. Biomechanical consequences of a tear of the posterior root of the medial meniscus. Similar to total meniscectomy. Am J Sports Med 2008;36:192-7. [Google Scholar] [PubMed]
- 3. LaPrade RF, Ho CP, James E, Crespo B, LaPrade CM, Matheny LM. Diagnostic accuracy and outcomes of medial meniscus posterior root tears. Am J Sports Med 2014;42:2563-9. [Google Scholar] [PubMed]
- 4. Feucht MJ, Kühle J, Bode G, Mehl J, Schmal H, Südkamp NP, et al. Arthroscopic transtibial pullout repair for posterior medial meniscus root tears: A systematic review of clinical, radiographic, and second-look arthroscopic results. Knee Surg Sports Traumatol Arthrosc 2015;23:119-25. [Google Scholar] [PubMed]
- 5. Staubli AE, De Simoni C, Babst R, Lobenhoffer P. TomoFix: A new LCP-concept for open wedge osteotomy of the medial proximal tibia–early results in 92 cases. Injury 2003;34:B55-62. [Google Scholar] [PubMed]
- 6. El-Azab HM, Morgenstern M, Ahrens P, Schuster T, Imhoff AB, Lorenz SG. Limb alignment after open-wedge high tibial osteotomy and its effect on clinical outcome. Am J Sports Med 2011;39:509-15. [Google Scholar] [PubMed]
- 7. Miniaci A, Ballmer FT, Ballmer PM, Jakob RP. Proximal tibial osteotomy. A new fixation device. Clin Orthop Relat Res 1989;246:250-9. [Google Scholar] [PubMed]
- 8. Paley D, Herzenberg JE, Tetsworth K, McKie J, Bhave A. Deformity planning for frontal and sagittal plane corrective osteotomies. Orthop Clin North Am 1994;25:425-65. [Google Scholar] [PubMed]
- 9. Lobenhoffer P, Agneskirchner JD. Improvements in valgus high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 2003;11:132-8. [Google Scholar] [PubMed]
- 10. Brosset T, Pasquier G, Migaud H, Gougeon F. Opening wedge high tibial osteotomy without bone grafting. Orthop Traumatol Surg Res 2011;97:705-11. [Google Scholar] [PubMed]
- 11. Takeuchi R, Ishikawa H, Aratake M, Bito H, Saito I, Kumagai K, et al. Medial opening wedge high tibial osteotomy with early full weight bearing. Arthroscopy 2009;25:46-53. [Google Scholar] [PubMed]
- 12. Schröter S, Ihle C, Mueller J, Lobenhoffer P, Stöckle U, Van Heerwaarden R. Digital planning of high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 2013;21:189-96. [Google Scholar] [PubMed]
- 13. Bode G, Von Heyden J, Pestka JM, Schmal H, Südkamp NP, Niemeyer P. Prospective 5-year survival rate data following open-wedge valgus high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 2015;23:1949-55. [Google Scholar] [PubMed]
- 14. Lee OS, Ahn S, Lee YS. Effect of pes anserinus release on postoperative pain and medial stability in medial opening wedge high tibial osteotomy. Arch Orthop Trauma Surg 2021;141:273-80. [Google Scholar] [PubMed]
- 15. Nakamura R, Kuroda K, Takahashi M, Katsuki Y. Open wedge high tibial osteotomy with pes anserinus preservation. Arthrosc Tech 2022;11:e69-78. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Outcome of Medial Open Wedge High Tibial Osteotomy for Knee Osteoarthritis: A Case Series
February 1, 2026 Outcome of Medial Open Wedge High Tibial Osteotomy for Knee Osteoarthritis: A Case Series October 1, 2025 One-stage Anterior Cruciate Ligament Reconstruction with Medial Open Wedge High Tibial Osteotomy – A Surgical Technique
October 1, 2025 One-stage Anterior Cruciate Ligament Reconstruction with Medial Open Wedge High Tibial Osteotomy – A Surgical Technique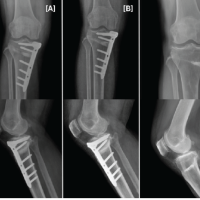 January 1, 2025 Tibial Nerve injury in Medial Open Wedge-High Tibial Osteotomy – A Rare Complication with 14-Year Follow-Up
January 1, 2025 Tibial Nerve injury in Medial Open Wedge-High Tibial Osteotomy – A Rare Complication with 14-Year Follow-Up August 1, 2026 Bicruciate Ligament Avulsions, Lateral Meniscus Dual Root Avulsions – “Tibial Avulsion Tetrad” – with Menisco-capsular Injury – Floating Meniscus in Innocuous Looking Proximal Tibia Fracture
August 1, 2026 Bicruciate Ligament Avulsions, Lateral Meniscus Dual Root Avulsions – “Tibial Avulsion Tetrad” – with Menisco-capsular Injury – Floating Meniscus in Innocuous Looking Proximal Tibia Fracture