
A calcaneal aneurysmal bone cyst, though rare, should be considered in young patients with chronic heel pain, and extended curettage with bone grafting provides good outcomes with low recurrence.
Dr. Elandevan Gunasekaran, Department of Orthopaedics, All India Institute of Medical Sciences, Guntur, Andhra Pradesh, India. E-mail: elandevangunasekaran@gmail.com
Abstract
Introduction: Aneurysmal bone cyst (ABC) is a benign but locally aggressive osteolytic lesion that commonly affects long bones and vertebrae. Involvement of the calcaneum is rare and presents a unique diagnostic and therapeutic challenge due to its weight-bearing nature.
Case Report: A 23-year-old male presented with pain in the left heel for 6 months, insidious in onset and progressive in nature, aggravated by weight-bearing. Clinical examination revealed localised tenderness over the calcaneum. Radiographs showed an expansile osteolytic lesion with cortical thinning. Magnetic resonance imaging demonstrated a multiloculated cystic lesion with multiple fluid–fluid levels suggestive of ABC. The patient underwent extended curettage and autologous cancellous bone grafting and bone substitutes. Histopathological examination confirmed the diagnosis of ABC. At the 6-month follow-up, the patient was asymptomatic with no evidence of recurrence.
Conclusion: Calcaneal ABC is a rare entity that should be considered in young patients presenting with chronic heel pain. Imaging aids in diagnosis, but histopathology is mandated. Extended curettage with bone grafting is an effective treatment option with good functional outcomes and low recurrence rates.
Keywords: Aneurysmal bone cyst, calcaneum, curettage, bone graft, heel pain.
An aneurysmal bone cyst (ABC) is a benign expansile lesion accounting for approximately 1% of all primary bone tumours [1,2]. It commonly affects children and young adults [2,3]. ABC may arise as a primary lesion or secondarily in association with other bone pathologies, including giant cell tumour, chondroblastoma, and fibrous dysplasia [4]. The most common sites of involvement are long bones and the vertebral column; however, occurrence in the foot is rare, accounting for a small proportion of cases. Among foot bones, calcaneal involvement is particularly uncommon, comprising approximately 1–2% of all ABCs [5,6]. Due to its location in a weight-bearing bone, calcaneal ABC presents unique clinical and therapeutic challenges [7]. Clinically, patients with calcaneal ABC typically present with heel pain, which may be insidious in onset and progressive in nature. Unlike the ABCs of long bones, pathological fractures are less common in the calcaneum. Radiologically, ABC appears as an expansile lytic lesion with cortical thinning, while magnetic resonance imaging often demonstrates fluid–fluid levels, which are highly suggestive but not pathognomonic [8]. The differential diagnosis includes unicameral bone cyst, chondroblastoma, and giant cell tumour, necessitating histopathological confirmation. Given its rarity and potential for recurrence, optimal management of calcaneal ABC remains a subject of discussion. We report a rare case of calcaneal ABC in a young adult and highlight its clinical presentation, diagnostic approach, and management.
A 23-year-old male presented with complaints of pain in the right heel for 6 months. The pain was insidious in onset, progressive, and aggravated by walking and weight-bearing. There was no history of trauma or constitutional symptoms. On examination, there was localised tenderness over the calcaneum without swelling or skin changes. Ankle and subtalar movements were preserved but painful. Radiographs revealed an expansile osteolytic lesion in the calcaneum with cortical thinning (Fig. 1).

Figure 1: Pre-operative radiograph. Anteroposterior, lateral, and Harris view radiographs of the right foot showing an expansile osteolytic lesion involving the calcaneum with well-defined margins and cortical thinning, suggestive of a benign cystic lesion.
Magnetic resonance imaging (MRI) showed a multiloculated lesion with multiple fluid–fluid levels, suggestive of ABC (Fig. 2).
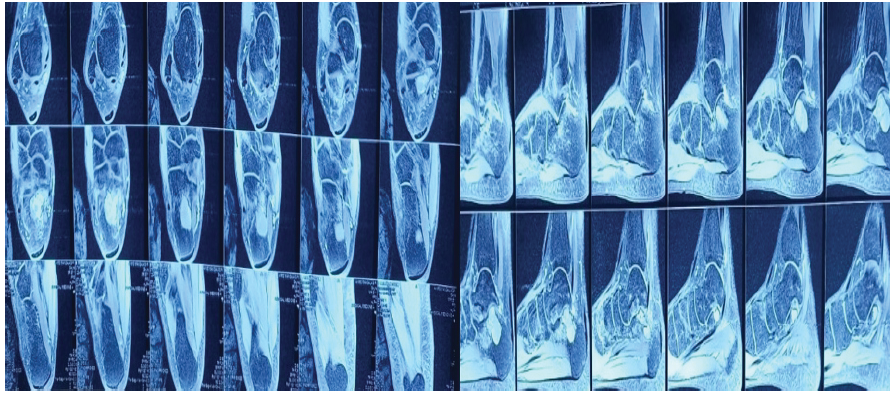
Figure 2: Magnetic resonance imaging of the right foot demonstrating a multiloculated cystic lesion in the calcaneum with multiple fluid–fluid levels, characteristic of an aneurysmal bone cyst.
Differential diagnoses included unicameral bone cyst, chondroblastoma, giant cell tumour, and telangiectatic osteosarcoma. The patient underwent extended curettage and bone grafting. A cortical window was made, and the lesion was thoroughly curetted (Fig. 3).

Figure 3: Intraoperative image – Curettage. Intraoperative photograph showing cortical window over the calcaneum and exposure of the cystic cavity during curettage.
Extended curettage was performed using a high-speed burr. The cavity was filled with an autologous cancellous bone graft from the iliac crest and bone substitute (Figs. 4 and 5).

Figure 4: Intraoperative image – cavity. Intraoperative image demonstrating the evacuated cystic cavity following thorough curettage and extended removal of lesion contents.

Figure 5: Bone grafting. Intraoperative photograph showing filling of the calcaneal defect with autologous cancellous bone graft harvested from the iliac crest.
Histopathological examination showed blood-filled spaces separated by fibrous septa containing fibroblasts, multinucleated giant cells, and reactive bone, confirming ABC. Post-operatively, the patient was put on a below-knee Plaster of Paris cast for 6 weeks, followed by gradual mobilisation (Fig. 6). At the 6-month follow-up, the patient was pain-free, with no evidence of recurrence, and had returned to normal activities.
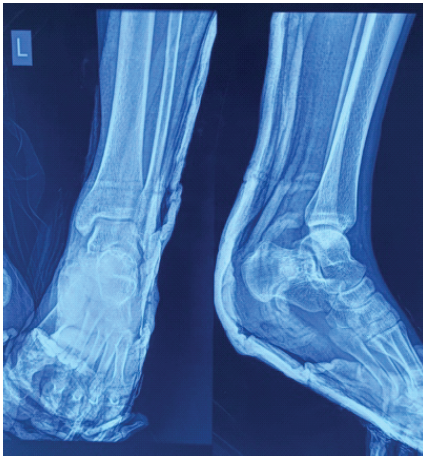
Figure 6: Post-operative radiograph showing the calcaneum filled with bone graft material with restoration of structural integrity.
ABC is a benign but locally aggressive lesion that poses diagnostic and therapeutic challenges, particularly when occurring in rare locations, such as the calcaneum. Although ABC commonly affects long bones and vertebrae, involvement of the calcaneum is uncommon, accounting for approximately 1–2% of cases. Due to its rarity and overlapping radiological features with other cystic lesions, diagnosis can be difficult. Clinically, calcaneal ABC typically presents with heel pain, as seen in our case, rather than a pathological fracture, which is more common in long bones [9]. Radiographically, ABC appears as an expansile osteolytic lesion with cortical thinning, while MRI findings of fluid–fluid levels are highly suggestive but not specific [10]. Hence, differentiation from entities such as unicameral bone cyst, chondroblastoma, giant cell tumour, and telangiectatic osteosarcoma is essential [11]. Histopathological examination remains the gold standard for definitive diagnosis, demonstrating characteristic blood-filled spaces and multinucleated giant cells [12]. The management of calcaneal ABC is influenced by its location in a weight-bearing bone. While various treatment modalities, such as sclerotherapy and embolisation, have been described, intralesional curettage with bone grafting remains the most widely accepted approach [13,14]. In our case, extended curettage using a high-speed burr was performed to reduce recurrence risk, followed by bone grafting to restore structural integrity and support early mobilisation. Recurrence rates for ABC range from 10% to 30%, with higher rates reported following incomplete removal [15]. The use of extended curettage techniques has been shown to significantly decrease recurrence. Our patient demonstrated excellent clinical and radiological outcomes at 6 months’ follow-up, with no evidence of recurrence. This case highlights the importance of considering ABC in the differential diagnosis of calcaneal lesions and supports extended curettage with bone grafting as an effective treatment modality in achieving favourable outcomes.
Calcaneal ABC is a rare entity presenting with chronic heel pain. Accurate diagnosis requires correlation of clinical, radiological, and histopathological findings. Extended curettage with bone grafting and guarded mobilisation is an effective treatment modality with good functional outcomes.
- Consider ABC in young patients with persistent heel pain
- MRI fluid–fluid levels are suggestive but not definitive
- Histopathology is mandatory for diagnosis
- Extended curettage with bone grafting is the treatment of choice.
References
- 1. Mankin HJ, Hornicek FJ, Ortiz-Cruz E, Villafuerte J, Gebhardt MC. Aneurysmal bone cyst: A review of 150 patients. J Clin Oncol 2005;23:6756-62. [Google Scholar] [PubMed]
- 2. Leithner A, Windhager R, Lang S, Haas OA, Kainberger F, Kotz R. Aneurysmal bone cyst. A population based epidemiologic study and literature review. Clin Orthop Relat Res 1999;363:176-9. [Google Scholar] [PubMed]
- 3. Cottalorda J, Bourelle S. Current treatments of primary aneurysmal bone cysts. J Pediatr Orthop B 2006;15:155-67. [Google Scholar] [PubMed]
- 4. Chakarun CJ, Forrester DM, Gottsegen CJ, Patel DB, White EA, Matcuk GR Jr. Giant cell tumor of bone: Review, mimics, and new developments in treatment. Radiographics 2013;33:197-211. [Google Scholar] [PubMed]
- 5. Rapp TB, Ward JP, Alaia MJ. Aneurysmal bone cyst. J Am Acad Orthop Surg 2012;20:233-41. [Google Scholar] [PubMed]
- 6. Sharma S, Gupta N, Singh R, Sharma V. Aneurysmal bone cyst of calcaneum: A rare case report. J Clin Orthop Trauma 2015;6:204-7. [Google Scholar] [PubMed]
- 7. Kulkarni AG, Shah SP, Kulkarni SG. Aneurysmal bone cyst of calcaneum: A rare case report. Indian J Orthop 2013;47:309-12. [Google Scholar] [PubMed]
- 8. Vaishya R, Agarwal AK, Vijay V. Aneurysmal bone cyst of calcaneum: A case report and review of literature. J Orthop Case Rep 2017;7:45-8. [Google Scholar] [PubMed]
- 9. Singh J, James SL, Kroon HM, Woertler K, Davies AM. Tumour and tumour-like lesions of the calcaneus: A pictorial review. Insights Imaging 2011;2:627-37. [Google Scholar] [PubMed]
- 10. Papagelopoulos PJ, Choudhury SN, Frassica FJ, Bond JR, Unni KK, Sim FH. Treatment of aneurysmal bone cysts of the pelvis and sacrum. J Bone Joint Surg Am 2001;83:1674-81. [Google Scholar] [PubMed]
- 11. Mascard E, Gomez-Brouchet A, Lambot K. Bone cysts: Unicameral and aneurysmal bone cyst. Orthop Traumatol Surg Res 2015;101 1 Suppl:S119-27. [Google Scholar] [PubMed]
- 12. Mendenhall WM, Zlotecki RA, Gibbs CP, Reith JD, Scarborough MT. Aneurysmal bone cyst. Am J Clin Oncol 2006;29:311-5. [Google Scholar] [PubMed]
- 13. Varshney MK, Rastogi S, Khan SA, Trikha V. Is sclerotherapy better than intralesional excision for treating aneurysmal bone cysts? Clin Orthop Relat Res 2010;468:1649-59. [Google Scholar] [PubMed]
- 14. Rastogi S, Varshney MK, Trikha V, Khan SA, Choudhury B. Treatment of aneurysmal bone cysts with percutaneous sclerotherapy using polidocanol. J Bone Joint Surg Br 2006;88:1212-6. [Google Scholar] [PubMed]
- 15. Park HY, Yang SK, Sheppard WL, Hegde V, Zoller SD, Nelson SD, et al. Current management of aneurysmal bone cysts. Curr Rev Musculoskelet Med 2016;9:435-44 [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2025 Aneurysmal Bone Cyst of Talus: A Case Report
September 1, 2025 Aneurysmal Bone Cyst of Talus: A Case Report July 1, 2025 Aneurysmal Bone Cyst of Thoracic Spine in an Elderly Treated by Two Stage 360° Surgical Excision and Reconstruction with Expandable Cage – A Case Report
July 1, 2025 Aneurysmal Bone Cyst of Thoracic Spine in an Elderly Treated by Two Stage 360° Surgical Excision and Reconstruction with Expandable Cage – A Case Report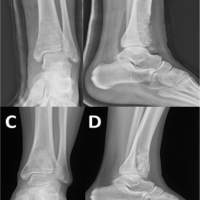 June 10, 2024 Response of Recurrent Aggressive Aneurysmal Bone Cyst of Distal Tibia to Denosumab Treatment
June 10, 2024 Response of Recurrent Aggressive Aneurysmal Bone Cyst of Distal Tibia to Denosumab Treatment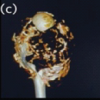 July 1, 2026 Aneurysmal Bone Cyst of the Proximal Humerus Managed with En Bloc Resection, Fibular Strut Grafting, and PHILOS Fixation: A Case Report
July 1, 2026 Aneurysmal Bone Cyst of the Proximal Humerus Managed with En Bloc Resection, Fibular Strut Grafting, and PHILOS Fixation: A Case Report