
Persistent unexplained thigh pain in previously irradiated femurs following limb-salvage surgery may indicate impending biomechanical failure requiring early reconstructive intervention.
Dr. Abhijith Annasamudram, Department of Orthopaedic Surgery, Montefiore Einstein, Bronx, NY, USA. E-mail: aannasamud@montefiore.org
Abstract
Introduction: Femoral fractures following combined surgery and radiotherapy for soft-tissue sarcomas of the anterior thigh are uncommon but clinically challenging complications. Reported outcomes vary widely, with internal fixation frequently complicated by delayed union, non-union, or mechanical failure, particularly in the setting of irradiated bone and additional patient- or treatment-related risk factors.
Case Report: In this report, we describe two patients with high-grade anterior thigh soft-tissue sarcomas treated with limb-sparing surgery and radiotherapy who subsequently developed femoral fractures within the irradiated field. Both patients underwent intramedullary nail fixation and progressed to non-union with fixation failure, necessitating salvage with distal femur endoprosthetic reconstruction. One patient achieved durable limb salvage following reconstruction, whereas the second developed progressive soft-tissue compromise and periprosthetic infection, ultimately requiring above-knee amputation.
Conclusion: These cases highlight the complexity of managing femoral fractures in irradiated bone and underscore the limitations of fixation strategies reliant on biologic healing in high-risk patients. Persistent, unexplained thigh pain may represent an early warning sign of impending mechanical failure. Early risk stratification and timely consideration of reconstructive strategies that provide immediate mechanical stability may help mitigate morbidity in select patients following limb-salvage treatment for soft-tissue sarcoma.
Keywords: Soft-tissue sarcoma, radiation-associated femoral fracture, nonunion, distal femur replacement, limb salvage.
Limb-salvage surgery combined with radiotherapy is the standard of care for high-grade soft-tissue sarcomas of the extremities. Although this approach provides excellent local tumour control, radiation-induced injury to bone and surrounding soft tissues may predispose patients to insufficiency fractures, delayed union, non-union, and fixation failure [1,2,3]. Management of femoral fractures in this setting is particularly challenging due to compromised bone biology, altered biomechanics, and diminished healing capacity resulting from prior oncologic treatment. We present two cases of radiation-associated femoral nonunion following limb-salvage treatment for thigh sarcoma, illustrating divergent clinical courses and reconstructive outcomes.
Case 1:
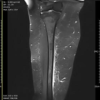
A 58-year-old male with a history of type 2 diabetes mellitus, hypertension, hyperlipidaemia, gout, and morbid obesity (body mass index [BMI] 46.20 kg/m2) who presented with several months of progressive atraumatic right thigh pain and swelling. Magnetic resonance imaging demonstrated a large heterogeneous intramuscular mass involving the anterior compartment of the thigh concerning a high-grade soft-tissue sarcoma. Open biopsy confirmed a dedifferentiated liposarcoma characterised by high-grade pleomorphic spindle cells with MDM2 amplification. Following multidisciplinary tumour board discussion, neoadjuvant radiotherapy followed by wide local excision was recommended. The patient completed neoadjuvant external beam radiotherapy to a total dose of 50 Gy delivered in 25 fractions and subsequently underwent wide local resection through an anteromedial approach with en bloc resection of the involved anterior compartment musculature. Limited anterior and medial periosteal stripping of the femur was required to achieve oncologic clearance without posterior or lateral cortical disruption. Primary closure was achieved without flap reconstruction. Final pathology demonstrated a high-grade dedifferentiated liposarcoma with marked treatment effects and R0 margins. Five months postoperatively, surveillance imaging revealed bilateral pulmonary metastases, prompting initiation of systemic chemotherapy with the AIM regimen (doxorubicin, ifosfamide, and mesna), followed by staged pulmonary metastasectomies. Postoperatively, the patient achieved full postoperative recovery with full weight-bearing, full knee range of motion, and independent ambulation using a cane, which was a return to his baseline function. Eight months following surgical resection, he developed progressive distal thigh pain. Interval magnetic resonance imaging demonstrated a large postoperative seroma and a subcutaneous, 2 cm soft-tissue lesion in the anterior distal thigh. The lesion was localised to the subcutaneous tissues, was tender to palpation, and demonstrated no overlying skin changes, erythema, or warmth. Given its focal nature and superficial location, it was initially considered a possible contributor to the patient’s localised pain. However, in the absence of radiographic features suggestive of impending fracture or osseous compromise and with preservation of full weight-bearing, knee range of motion, and overall functional status, prophylactic fixation was deferred. Ten months after index surgery, the patient sustained a low-energy trauma while ambulating, resulting in a distal femoral shaft fracture. Preoperative imaging and intraoperative biopsy from the fracture site demonstrated no evidence of recurrent or metastatic sarcoma. The fracture was treated surgically with retrograde intramedullary nailing. At 12 months from index surgery, following systemic therapy, the patient underwent staged bilateral pulmonary metastasectomies, achieving complete resection of metastatic disease. Despite excellent reduction, substantial bony apposition, and stable fixation, the patient presented at a 15-month follow-up with acute pain and an inability to bear weight. Imaging confirmed implant failure through one of the distal interlocking screws, confirming non-union at the fracture site. He was indicated for removal of hardware and reconstruction using a right distal femur, replacing a rotating hinge endoprosthesis as definitive management. Surgical goals included durable limb salvage, independent of fracture healing, and immediate postoperative weight-bearing. The symptomatic anterior distal thigh soft-tissue lesion was excised concurrently, with final pathology demonstrating a well-circumscribed benign epithelial neoplasm consistent with spiradenoma, a painful sweat gland tumour, explaining the patient’s localised anterior thigh pain and confirming the absence of malignant disease.
Case 2:
A 52-year-old male with a medical history significant for morbid obesity (BMI 43.53 kg/m2), hypertension, obstructive sleep apnoea, and metastatic alveolar soft part sarcoma of the anterior thigh presented with progressive lower-extremity pain and functional decline. His oncologic history dated back more than two decades, when he underwent wide resection of anterior thigh sarcoma followed by combined brachytherapy, external beam radiation therapy, and multiagent chemotherapy (doxorubicin, ifosfamide, and dacarbazine). Pulmonary nodules developed 2 years after his initial diagnosis, and he was managed with resection, inhaled doxorubicin on a clinical trial, liposomal doxorubicin, and capecitabine. Eight years from diagnosis, he initiated sunitinib, and his disease remained clinically quiescent with ongoing oncologic surveillance. Approximately 1 year before presentation (20 years after initial sarcoma excision), he sustained a low-energy traumatic event resulting in a closed, extra-articular distal femoral fracture within the previously irradiated field. He underwent intramedullary nail fixation at an outside institution but experienced persistent pain and progressive functional limitation. Subsequent evaluation demonstrated femoral nonunion with implant failure, including fracture of the nail and a distal interlocking screw. Given the history of prior radiation exposure and failed fixation, he underwent removal of hardware with an open biopsy followed by distal femur endoprosthetic reconstruction. His pathology was negative for recurrence of sarcoma or infection. Although early post-operative recovery was initially satisfactory, his course was complicated by progressive ipsilateral lower-extremity lymphoedema, increasing pain, swelling, and eventually malodorous wound drainage consistent with deep infection. The initial debridement surgery revealed significant necrotic, poorly vascularised soft tissues in the previously radiated field and extensive purulence throughout the thigh and leg compartments. His periprosthetic joint infection was due to klebsiella pneumoniae and enterococcus faecalis. Due to polymicrobial infection, compromised soft-tissue envelope, and poor healing potential, he elected to proceed with an above-knee amputation. His immediate post-operative course was smooth; he was discharged to an inpatient rehabilitation facility for post-operative recovery and functional rehabilitation for 2 weeks and then transitioned home. He completed an oral regimen of Augmentin for 2 weeks as an outpatient. Gabapentin was initiated for phantom limb discomfort, and he weaned from narcotics within 3 weeks.
Femoral fractures following limb-salvage surgery combined with radiotherapy for soft-tissue sarcoma are uncommon but clinically consequential. Reported fracture incidence ranges from 2% to 22%. This may be impacted by heterogeneity in radiation dose, treatment technique, extent of surgical exposure, and patient-specific risk factors [1,2,3,4]. Femoral fracture risk has been reported to be related to several variables, including anatomic location, limb-sparing surgery, length of resection, and degree or extent of periosteal disruption [1,4,5,6]. Larger contemporary series further confirmed that femoral fracture remains an important late complication despite advances in multidisciplinary sarcoma care [2,3,5,7]. Previously published reports relevant to fracture risk, radiation-associated bone injury, fixation failure, and reconstructive outcomes are summarised in Table 1.
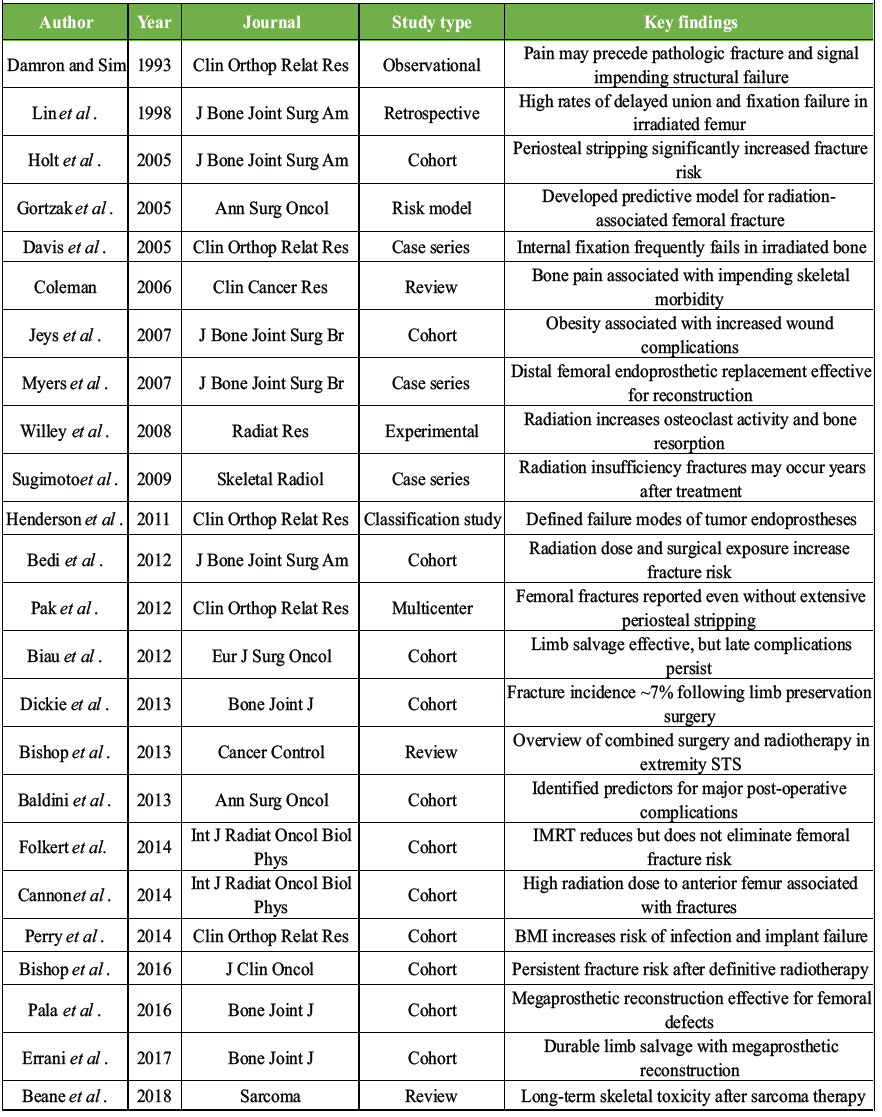
Table 1: Literature review of reported femoral fractures following limb-salvage surgery and radiotherapy for extremity soft-tissue sarcoma
Radiation-associated skeletal injury is mediated through several well-described biological mechanisms. Ionising radiation suppresses osteoblast proliferation and differentiation, increases osteoclast-mediated resorption, and damages the microvascular supply required for cortical bone viability and fracture healing [8,9,10]. These biological effects culminate in reduced bone mineral density, impaired remodelling, and diminished reparative capacity. Experimental work by Willey et al. demonstrated an early increase in osteoclast activity after radiation exposure, providing a mechanistic basis for the progressive bone fragility seen clinically in irradiated femora [9]. Clinically, insufficiency fractures may occur months to years after treatment, underscoring the durable nature of radiation-induced skeletal toxicity [8,11]. Radiation dose and dose distribution also influence fracture risk. Prior work has shown that fracture risk increases with higher cumulative radiation exposure, particularly when the anterior femoral cortex is included within the high-dose field [2,3,5,12,13,14]. Because the anterior cortex is subjected to greater tensile stress during ambulation, this region may be particularly vulnerable after radiation-induced weakening. Although modern radiotherapy techniques such as intensity-modulated radiotherapy (IMRT) have improved dose conformality and reduced exposure to uninvolved bone, femoral fractures continue to occur, suggesting that surgical factors and host-related variables remain important contributors to skeletal toxicity [3,12,14]. Surgical technique remains another critical determinant of fracture risk. Preservation of the periosteum and maintenance of cortical vascularity are important for cortical viability after radiation exposure. Multiple series have demonstrated that extensive periosteal stripping during tumour resection substantially increases the likelihood of subsequent femoral fracture [1,5,6,10]. At the same time, more recent literature suggests that periosteal injury should not be viewed in isolation. Pak et al. showed that femoral fractures can occur even without extensive periosteal stripping, emphasising that fracture risk is multifactorial and likely reflects the combined effects of radiation injury, altered biomechanics, surgical exposure, and host characteristics [7]. Predictive modelling studies have similarly suggested that cumulative risk is better explained by the interaction of several moderate-risk variables rather than any single feature alone [15]. Patient-related characteristics further influence both fracture risk and reconstructive outcomes. Morbid obesity, present in both currently reported cases, increases mechanical loading across the femur and may magnify cantilever stresses in already compromised bone [16,17]. In addition, radiation fibrosis and loss of functional musculature may alter force transmission and reduce dynamic stabilisation of the femur. Obesity is associated with increased wound complications, infection, and implant failure following limb-salvage surgery and megaprosthetic reconstruction, underscoring additional risks with which it is associated [16,17]. A clinically important observation in both of the currently presented cases was the presence of persistent unexplained thigh pain preceding either fracture or fixation failure. Pain has been recognised as an early clinical indicator of impending structural compromise in oncologic bone disease, even when imaging findings are subtle [18,19]. In the setting of a previously irradiated femur, persistent focal pain should therefore prompt heightened suspicion for evolving biomechanical failure and may justify closer surveillance, additional imaging, or earlier intervention. Management of femoral fractures in irradiated bone remains particularly challenging because internal fixation relies on biologic healing in a host environment where fracture repair is impaired [4,8,20]. Earlier reports of fixation in irradiated femora documented substantial rates of delayed union, non-union, and mechanical failure [4,20]. These limitations help explain why intramedullary fixation may be insufficient in selected high-risk patients, even when alignment and implant position are satisfactory at the index fracture surgery. For this reason, several authors have advocated consideration of endoprosthetic reconstruction in select patients with radiation-associated femoral fracture or failed fixation [21,22,23,24]. Endoprosthetic reconstruction provides immediate mechanical stability, allows early weight-bearing, and eliminates dependence on fracture healing [22,23,24]. Long-term studies of distal femoral and megaprosthetic reconstruction have demonstrated that this approach can provide durable limb salvage, although outcomes remain heavily dependent on host biology, soft-tissue envelope quality, and infection risk [17,21,22,23,24]. The present report adds to the literature in several important ways. First, it describes two distinct clinical trajectories after radiation-associated femoral fractures in patients treated for thigh soft-tissue sarcoma: one successfully salvaged with distal femoral endoprosthetic reconstruction and another progressing to infection and eventual amputation. Second, these cases highlight persistent unexplained thigh pain as a potential early warning sign of impending mechanical compromise in irradiated bone. Finally, the cases emphasise the limitations of fixation strategies that rely on biologic fracture healing in previously irradiated bone and support consideration of reconstructive options that provide immediate mechanical stability in appropriately selected high-risk patients. Taken together, these cases illustrate a spectrum of outcomes associated with radiation-related femoral fracture after limb-salvage treatment for soft-tissue sarcoma. These divergent outcomes underscore the need for careful risk stratification, vigilance for early clinical warning signs, and individualised decision-making when treating femoral fractures in irradiated bone.
These two cases illustrate the spectrum of radiation-associated femoral fractures following limb-salvage treatment for high-grade soft-tissue sarcoma. Case 1 demonstrates successful salvage with distal femur replacement following fixation failure, whereas Case 2 underscores the potential for catastrophic complications, including infection and limb loss, despite aggressive reconstructive efforts. Persistent unexplained thigh pain should prompt heightened suspicion for biomechanical compromise in irradiated extremities. Early risk stratification and timely consideration of reconstructive strategies that minimise reliance on biological healing may help reduce morbidity in select high-risk patients.
Persistent, unexplained thigh pain in a previously irradiated extremity following limb-sparing sarcoma resection should raise concern for underlying biomechanical compromise, even when imaging does not demonstrate an overt fracture. In high-risk patients – particularly those with substantial radiation exposure, morbid obesity, or significant post-radiation fibrosis – early consideration of prophylactic stabilisation or definitive reconstruction may help prevent fracture and avert the cascade of complications associated with fixation failure, infection, and limb loss.
References
- 1. Holt GE, Griffin AM, Pintilie M, Wunder JS, Catton C, O’Sullivan B, et al. Fractures following radiotherapy and limb-salvage surgery for lower extremity soft-tissue sarcomas. A comparison of high-dose and low-dose radiotherapy. J Bone Joint Surg Am 2005;87:315-9. [Google Scholar] [PubMed]
- 2. Dickie CI, Parent AL, Griffin AM, Fung S, Chung PW, Catton CN, et al. Bone fractures following external beam radiotherapy and limb-preservation surgery for lower extremity soft tissue sarcoma: Relationship to irradiated bone length, volume, tumor location and dose. Bone Joint J 2013;95-B:395-401. [Google Scholar] [PubMed]
- 3. Bishop AJ, Zagars GK, Torres KE. Fracture risk after definitive radiotherapy for extremity soft tissue sarcoma. J Clin Oncol 2016;34:3883-9. [Google Scholar] [PubMed]
- 4. Lin PP, Schupak KD, Boland PJ, Brennan MF, Healey JH. Pathologic femoral fractures after limb-sparing treatment of soft-tissue sarcomas. J Bone Joint Surg Am 1998; 80:810-6. [Google Scholar] [PubMed]
- 5. Bedi M, King DM, White J. Risk factors for fracture after limb-sparing surgery and radiation therapy for soft tissue sarcomas of the extremities. J Bone Joint Surg Am 2012;94:e55. [Google Scholar] [PubMed]
- 6. Baldini EH, Lapidus MR, Wang Q. Predictors for major complications after surgery and radiotherapy for extremity soft-tissue sarcoma. Ann Surg Oncol 2013;20:1494-9. [Google Scholar] [PubMed]
- 7. Pak S, Mavrogenis AF, Savvidou OD. Femoral fractures after treatment of soft tissue sarcoma. Clin Orthop Relat Res 2012;470:3406-15. [Google Scholar] [PubMed]
- 8. Sugimoto M, Takahashi S, Mitsuya M. Radiation-induced insufficiency fractures of the femur. Skeletal Radiol 2009;38:661-8. [Google Scholar] [PubMed]
- 9. Willey JS, Lloyd SA, Robbins ME, Bourland JD, Smith-Sielicki H, Bowman LC, et al. Early increase in osteoclast number in mice after whole-body irradiation with 2 Gy X rays. Radiat Res 2008;170:388-92. [Google Scholar] [PubMed]
- 10. Bishop AJ, Guadagnolo BA, Zagars GK. The role of surgery and radiation therapy in the management of extremity soft tissue sarcoma. Cancer Control 2013;20:95-103. [Google Scholar] [PubMed]
- 11. Beane JD, Yang JC, White D. Long-term skeletal toxicity following sarcoma treatment. Sarcoma 2018; 2018:1-8. [Google Scholar] [PubMed]
- 12. Folkert MR, Singer S, Brennan MF. Femoral fracture risk after intensity-modulated radiation therapy for thigh soft tissue sarcoma. Int J Radiat Oncol Biol Phys 2014; 90:147-153. [Google Scholar] [PubMed]
- 13. Biau DJ, Ferguson PC, Chung P, Griffin AM, Catton CN, O’Sullivan B, et al. Local recurrence of extremity soft tissue sarcoma after limb-sparing surgery. Eur J Surg Oncol 2012;118:5867-77. [Google Scholar] [PubMed]
- 14. Cannon DM, Ballo MT, Zagars GK. Complications of combined modality therapy for extremity soft tissue sarcoma. Int J Radiat Oncol Biol Phys 2014;88:143-149. [Google Scholar] [PubMed]
- 15. Gortzak Y, Lockwood GA, Mahendra A. Prediction model for femoral fracture after limb-salvage surgery and radiotherapy for soft tissue sarcoma. Ann Surg Oncol 2005;12:999-1005. [Google Scholar] [PubMed]
- 16. Jeys L, Grimer RJ, Carter SR, Tillman RM. Risk factors for wound complications after limb salvage surgery for bone and soft tissue tumors. J Bone Joint Surg Br 2007;89:238-42. [Google Scholar] [PubMed]
- 17. Perry KI, Berry DJ, Harmsen WS. Divergent effects of body mass index on risk of wound complications and implant failure after megaprosthesis reconstruction. Clin Orthop Relat Res 2014;472:3045-51. [Google Scholar] [PubMed]
- 18. Damron TA, Sim FH. Clinical and radiological indicators of impending pathologic fracture after limb-sparing surgery and radiotherapy for bone and soft tissue tumors. Clin Orthop Relat Res 1993;293:207-15. [Google Scholar] [PubMed]
- 19. Coleman RE. Clinical features of metastatic bone disease and risk of skeletal morbidity. Clin Cancer Res 2006;12:6243s-9. [Google Scholar] [PubMed]
- 20. Davis AM. Fixation failure following radiation-associated fractures. Clin Orthop Relat Res 2005;438:71-78. [Google Scholar] [PubMed]
- 21. Henderson ER, Groundland JS, Pala E. Failure mode classification for tumor endoprostheses. Clin Orthop Relat Res 2011;469:3006-13. [Google Scholar] [PubMed]
- 22. Myers GJ, Abudu AT, Carter SR, Tillman RM, Grimer RJ. Endoprosthetic replacement of the distal femur for bone tumours: Long-term results. J Bone Joint Surg Br 2007;89:521-6. [Google Scholar] [PubMed]
- 23. Pala E, Trovarelli G, Angelini A. Megaprosthetic reconstruction for periprosthetic fractures of the femur. Bone Joint J 2016;98-B:1112-9. [Google Scholar] [PubMed]
- 24. Errani C, Tsukamoto S, Leone G. Megaprosthetic reconstruction of the distal femur. Bone Joint J 2020; 102-B:276-282. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Not All Red Flags Indicate Malignancy: A Case Report of a Benign Lipoma Mimicking Soft-tissue Sarcoma
August 1, 2026 Not All Red Flags Indicate Malignancy: A Case Report of a Benign Lipoma Mimicking Soft-tissue Sarcoma August 1, 2026 Successful Salvage of Infected Tibial Shaft Non-union After Implant Removal with Ilizarov External Fixation: A Case Report
August 1, 2026 Successful Salvage of Infected Tibial Shaft Non-union After Implant Removal with Ilizarov External Fixation: A Case Report August 1, 2026 Extensive Giant Cell Tumor Involving Entire Tibia with Talar Extension and Pulmonary Metastases: Successful Limb Preservation with Denosumab and Angioembolization
August 1, 2026 Extensive Giant Cell Tumor Involving Entire Tibia with Talar Extension and Pulmonary Metastases: Successful Limb Preservation with Denosumab and Angioembolization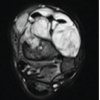 August 1, 2026 Low-Grade Myxofibrosarcoma of the Leg Presenting as a Pathological Pilon Fracture: A Case Report
August 1, 2026 Low-Grade Myxofibrosarcoma of the Leg Presenting as a Pathological Pilon Fracture: A Case Report