
Extensive proximal humerus ABCs need to be addressed with aggressive tumour clearance combined with stable structural reconstruction. Fibular strut grafting augmented with PHILOS plate fixation provides mechanical stability, facilitates starting mobilisation early, and restores shoulder function while minimising recurrence risk.
Dr. Chinmay S Torne, Department of Orthopaedics, Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra, India. E-mail: shreeghan@gmail.com
Abstract
Introduction: An aneurysmal bone cyst (ABC) is a benign, locally aggressive osteolytic lesion characterised by expansile blood-filled cavities separated by fibrous septa affecting the metaphyseal region of long bones in young individuals and accounting for approximately 1–2% of primary bone tumours. Proximal humerus involvement presents with reconstructive challenges due to the need to preserve shoulder biomechanics and rotator cuff function.
Case Report: A 28-year-old female presented with progressive pain and swelling of the left shoulder for 5 months, with restricted overhead activity. Imaging showed an expansile metaphyseal lytic lesion (Capanna Type II). A prior biopsy was suggestive of ABC. Two trials of selective arterial embolisation failed to improve clinically and radiologically. Management included repeat pre-operative angioembolisation followed by en bloc resection. The defect was reconstructed using a 15-cm non-vascularised ipsilateral fibular strut graft stabilised with a PHILOS plate. Histopathology confirmed the diagnosis of ABC. Serial follow-up demonstrated graft incorporation and union with restoration of painless full shoulder motion.
Conclusion: Large proximal humerus ABCs require meticulous oncologic clearance combined with stable structural reconstruction. Pre-operative embolisation followed by en bloc excision, fibular strut grafting, and PHILOS fixation provides satisfactory functional and radiological outcomes.
Keywords: Aneurysmal bone cyst, proximal humerus, fibular strut graft, PHILOS plate, En bloc resection, shoulder reconstruction.
An aneurysmal bone cyst (ABC) is a benign osteolytic tumour composed of blood-filled cavities separated by septa containing fibroblasts, osteoid tissue, and multinucleated giant cells [1]. Although considered reactive, molecular studies suggest a neoplastic origin in primary lesions [1,2]. ABC mostly affects children and young adults and most commonly involves the metaphysis of long bones [3]. Treatment includes extensive intralesional curettage with or without bone grafting, cement augmentation, cryotherapy, selective arterial embolisation, sclerotherapy, and en bloc resection [4,5,6]. Recurrence rates, particularly in aggressive lesions, following curettage range between 15% and 30% [7,8]. The proximal humerus presents specific challenges due to its biomechanical importance in shoulder girdle mobility and limb function. Extensive lesions with cortical thinning or impending fracture require aggressive management and structural reconstruction of anatomy to restore function [9]. We present a case of a large proximal humerus ABC managed with en bloc resection, fibular strut grafting, and PHILOS fixation.
A 28-year-old female presented with pain and progressive swelling over the left shoulder for 5 months, associated with difficulty performing overhead activities. Examination revealed localised warmth and prominent superficial veins. Distal neurovascular status was intact (Fig. 1).
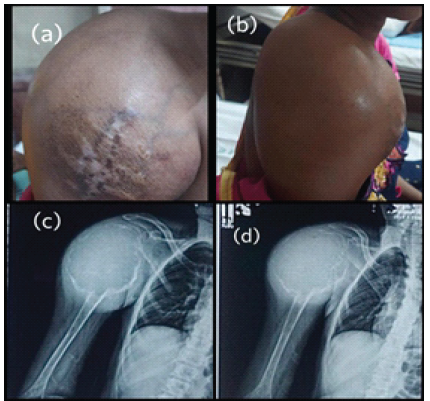
Figure 1: Pre-operative clinical photograph. (a) Anterior aspect (b) Lateral aspect pre-operative radiograph. (c) Anteroposterior view (d) Lateral view.
Plain radiographs showed a well-defined expansile lytic lesion with cortical thinning in the metaphyseal region. Computed tomography confirmed cortical expansion without breach. Magnetic resonance imaging (MRI) demonstrated multiple internal septations and characteristic fluid–fluid levels highly suggestive of ABC. The lesion was classified as Capanna Type II [7] (Fig. 2).
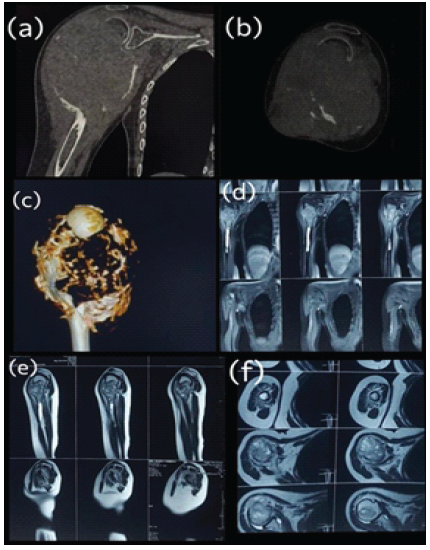
Figure 2: Pre-operative computed tomography (CT) scan. (a) Coronal CT image (b) sagittal CT image. (c) Three-dimensional CT reconstruction. Magnetic resonance imaging (MRI) of the right shoulder (d) coronal MRI image (e) sagittal MRI image (f) axial MRI image.
A biopsy performed elsewhere was confirmatory of ABC. The patient underwent two sessions of selective arterial embolisation without clinical or radiological improvement. Pre-operative embolisation was repeated to reduce intraoperative blood loss, as ABCs are highly vascular lesions [6] (Fig. 3).
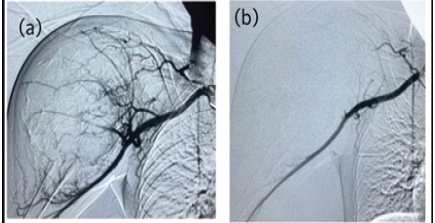
Figure 3: (a) Pre-embolization angiographic image (b) post-embolization angiographic image.
Through a standard deltopectoral approach, en bloc excision of the lesion was performed up to healthy bleeding bone margins. A 15-cm ipsilateral non-vascularised fibular strut graft was harvested (Fig. 4).
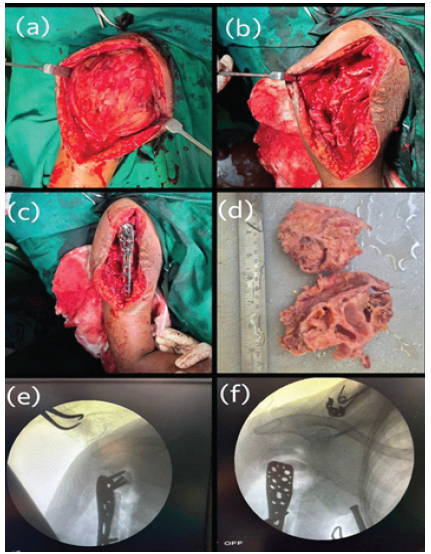
Figure 4: Intraoperative images. (a) Intraoperative photograph of the deltopectoral approach. (b) Complete curettage and removal of the lesion. (c) PHILOS plate fixation with fibular strut graft support. (d) Gross specimen of the lesion. (e and f) Intraoperative C-arm images.
The graft was inserted to reconstruct the defect and restore structural integrity. Fixation was achieved using a PHILOS plate under fluoroscopic guidance, providing angular stability and anatomical alignment [10] (Fig. 5).
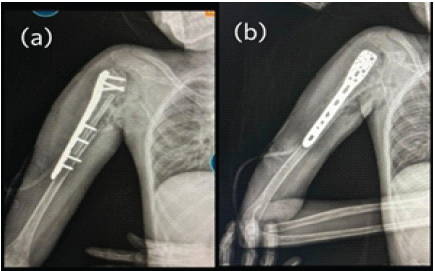
Figure 5: Post-operative radiograph. (a) Anteroposterior view (b) lateral view.
Histopathological examination confirmed ABC. Postoperatively, protected mobilisation was initiated early, followed by progressive range-of-motion exercises based on radiographic healing (Fig. 6).
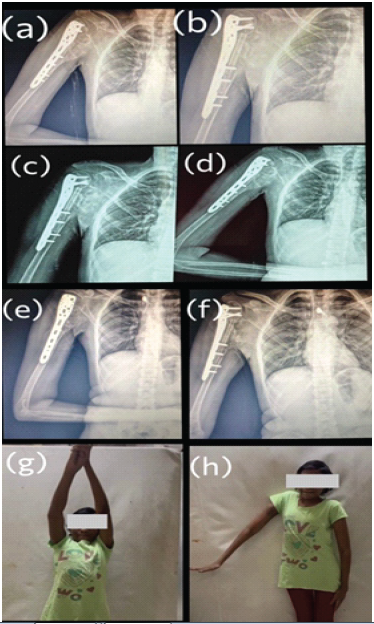
Figure 6: Follow-up radiographs at 1, 3 and 6 months showing maintained fixation of the proximal humerus with PHILOS plate and fibular strut graft, with no evidence of recurrence of Aneurysmal Bone Cyst. (a),(c),(e) Anteroposterior view (b),(d),(f) Lateral view(c, d) Clinical photographs demonstrating satisfactory functional range of motion of the right shoulder at 6 months postoperatively
ABC is a locally aggressive lesion with significant recurrence potential if inadequately treated [8]. While intralesional curettage remains common, extensive lesions with cortical compromise may require en bloc resection to minimise recurrence risk [4]. Selective arterial embolisation reduces intraoperative blood loss and serves as adjunctive or primary treatment in select cases [6]. However, in large lesions unresponsive to embolisation, definitive surgical excision remains the mainstay of management. Structural reconstruction following proximal humerus resection is essential to maintain shoulder biomechanics. Non-vascularised fibular strut grafting provides immediate mechanical support and promotes biological incorporation [11]. The PHILOS plate offers angular stability, particularly in metaphyseal bone with a compromised cortex, allowing early mobilisation and favourable functional recovery [10]. Donor site complications following fibular harvest are reported to be lower when proper technique is used [12]. In our case, the combination of oncologic clearance and stable biomechanical reconstruction resulted in graft incorporation, union, and restoration of full shoulder function without recurrence during follow-up. Limitations of the study include the single-case nature and limited follow-up duration.
Large proximal humerus ABCs need to be addressed with both oncologic and reconstructive challenges. Pre-operative embolisation followed by en bloc resection, non-vascularised fibular strut grafting, and PHILOS fixation provides reliable graft incorporation, mechanical stability, and satisfactory functional outcomes. Long-term follow-up is essential to monitor for recurrence.
Large aneurysmal bone cysts of the proximal humerus that fail non-operative measures such as selective arterial embolisation may require en bloc excision for adequate local control. Reconstruction using a non-vascularised fibular strut graft combined with PHILOS plate fixation provides stable biological reconstruction, facilitates early mobilisation, and can result in satisfactory functional and radiological outcomes.
References
- 1. Cottalorda J, Bourelle S. Current treatments of primary aneurysmal bone cysts. J Pediatr Orthop B. 2006;15:155-67. [Google Scholar] [PubMed]
- 2. Oliveira AM, Perez-Atayde AR, Inwards CY. USP6 and CDH11 oncogenes identify the neoplastic cell in primary aneurysmal bone cysts. Cancer Res 2004;64:1920-3. [Google Scholar] [PubMed]
- 3. Leithner A, Windhager R, Lang S, Haas OA, Kainberger F, Kotz R. Aneurysmal bone cyst. A population-based epidemiologic study and literature review. Clin Orthop Relat Res 1999;363:176-9. [Google Scholar] [PubMed]
- 4. Papagelopoulos PJ, Choudhury SN, Frassica FJ, Bond JR, Unni KK, Sim FH. Treatment of aneurysmal bone cysts of the pelvis and sacrum. J Bone Joint Surg Am 2001;83:1674-81. [Google Scholar] [PubMed]
- 5. Rastogi S, Varshney MK, Trikha V, Khan SA, Choudhury B, Safaya R. Treatment of aneurysmal bone cysts with percutaneous sclerotherapy using polidocanol. A review of 72 cases with long-term follow-up. J Bone Joint Surg Br 2006;88:1212-6. [Google Scholar] [PubMed]
- 6. Rossi G, Rimondi E, Bartalena T, Gerardi A, Alberghini M, Staals EL, et al. Selective arterial embolisation of 36 aneurysmal bone cysts of the skeleton with N-2-butyl cyanoacrylate. Skeletal Radiol 2010;39:161-7. [Google Scholar] [PubMed]
- 7. Capanna R, Campanacci DA, Manfrini M. Unicameral and aneurysmal bone cysts. In: Campanacci M, editor. Bone and Soft Tissue Tumours. 2nd Vienna: Springer; 1999. p. 735-88. [Google Scholar] [PubMed]
- 8. Gibbs CP Jr., Hefele MC, Peabody TD, Montag AG, Aithal V, Simon MA. Aneurysmal bone cyst of the extremities. Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-8. [Google Scholar] [PubMed]
- 9. Wright JG, Yandow S, Donaldson S, Marley L. Aneurysmal bone cyst of the humerus in children. J Pediatr Orthop 2000;20:54-9. [Google Scholar] [PubMed]
- 10. Gardner MJ, Boraiah S, Helfet DL, Lorich DG. Indirect medial reduction and strut support of proximal humerus fractures using an endosteal implant. J Orthop Trauma 2008;22:195-200. [Google Scholar] [PubMed]
- 11. Ring D, Jupiter JB, Sanders RA. Complex nonunion of fractures of the proximal humerus. Use of autogenous fibular strut graft and plate fixation. J Bone Joint Surg Am 2000;82:773-83. [Google Scholar] [PubMed]
- 12. Younger EM, Chapman MW. Morbidity at bone graft donor sites. J Orthop Trauma 1989;3:192-5. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Reverse Shoulder Arthroplasty with Virtual Implant Positioning System in the Management of Massive Rotator Cuff Tear with Rotator Cuff Arthropathy
August 1, 2026 Reverse Shoulder Arthroplasty with Virtual Implant Positioning System in the Management of Massive Rotator Cuff Tear with Rotator Cuff Arthropathy July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report
July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis
July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis July 1, 2026 Masquelet Technique Combined with Non-vascularized Fibular Strut Graft for Reconstruction of a Large Tibial Bone Defect in a Skeletally Immature Patient: A Case Report
July 1, 2026 Masquelet Technique Combined with Non-vascularized Fibular Strut Graft for Reconstruction of a Large Tibial Bone Defect in a Skeletally Immature Patient: A Case Report