
Post-discectomy septic spondylodiscitis needs aggressive treatment. Even in the presence of active infection, one can proceed with instrumented stabilization along with antibiotic therapy if needed.
Dr. G M Shafeeq, Fellow Spine Surgery, Max Hospital, Nagpur, Maharashtra, India. E-mail: drgmshafeeq@gmail.com
Abstract
Introduction: Spondylodiscitis is an inflammation (most commonly due to infection) involving the intervertebral disc and adjacent vertebral bodies. It represents a serious spinal condition that can lead to vertebral destruction, spinal instability, neurological deficits, and significant morbidity. Although the primary treatment consists of targeted antibiotic therapy and immobilization, surgical intervention becomes necessary in cases associated with spinal instability, neurological compromise, or failure of conservative treatment. Recent studies have shown that spinal instrumentation can be safely performed in the presence of infection when combined with adequate surgical debridement and appropriate antibiotic therapy, which prevent motion at the pathological site and promote healing.
Case Report: We report two cases of lumbar post-discectomy septic spondylodiscitis with spinal instability managed surgically. The first case involved a patient who developed multilevel lumbar spondylodiscitis following a previous L5–S1 microdiscectomy, presenting with persistent back pain and a discharging sinus. The second patient also had a history of L4-L5 discectomy, complicated by post-operative infection, leading to progressive neurological weakness and inability to ambulate. Both patients underwent surgical debridement, decompression, and pedicle screw stabilisation. Intraoperative cultures revealed Pseudomonas aeruginosa infection in the first case and Escherichia coli in the second case, and targeted antibiotic therapy was initiated.
Outcome: Both patients showed significant post-operative improvement with early ambulation, progressive neurological recovery, reduction of inflammatory markers, and satisfactory wound healing on follow-up.
Conclusion: Surgical stabilisation combined with adequate debridement and targeted antibiotic therapy plays a crucial role in the management of septic spondylodiscitis. Instrumentation provides immediate spinal stability, promotes healing, facilitates early mobilisation, and results in favourable clinical outcomes even in the presence of active infection.
Keywords: Spondylodiscitis, spinal infection, spinal stabilization, pedicle screw fixation, and spinal instrumentation.
Spondylodiscitis is an inflammation (most commonly due to infection) involving the intervertebral disc and adjacent vertebral bodies and represents one of the most serious forms of spinal infection. It accounts for approximately 2–7% of all cases of osteomyelitis, and its incidence has been increasing in recent years due to factors such as an ageing population, increased use of spinal procedures, immunosuppression, and improved diagnostic techniques [1,2]. The infection most commonly occurs through haematogenous spread, although it may also result from direct inoculation during spinal procedures or contiguous spread from adjacent infections [3]. The most frequent causative organisms are pyogenic bacteria, particularly Staphylococcus aureus, followed by Mycobacterium tuberculosis, especially in developing countries. Less commonly, fungal organisms may be responsible [1,4]. Patients typically present with severe back pain, fever, and elevated inflammatory markers, while advanced disease may lead to neurological deficits due to epidural abscess formation or spinal cord compression [2]. Early diagnosis using magnetic resonance imaging (MRI) and appropriate microbiological evaluation has significantly improved the management of this condition [3,5]. The cornerstone of treatment remains targeted antibiotic therapy combined with spinal immobilisation. However, conservative management may not be sufficient in cases associated with mechanical instability, neurological deficits, progressive deformity, epidural abscess, or failure of medical therapy [4,6].
In such situations, surgical intervention with adequate debridement and spinal stabilisation plays an important role in controlling infection, restoring spinal stability, preventing deformity progression, and allowing early mobilisation [6,7]. Recent advances in spinal instrumentation have demonstrated that implant placement is safe even in the presence of active infection when combined with thorough debridement and appropriate antibiotic therapy [7,8]. Even in recent years, the misconception persists that spinal instrumentation is absolutely contraindicated in the presence of active infection, underscoring the importance of these two successful case reports.
Case 1
A 55-year-old male presented to our department with complaints of severe low back pain and left lower limb symptoms for the past 20 days, associated with pain radiating to the left thigh and numbness in the left lower limb. On detailed history, the patient reported low back pain with left lower limb radiculopathy for approximately 1.5 years, for which he had undergone L5–S1 microdiscectomy for a prolapsed intervertebral disc at another hospital following clinical and radiological evaluation. Following the initial surgery, on the 7th post-operative day, the patient developed discharge from the surgical site, and there was a delay in wound healing. Two weeks after the primary procedure, he underwent surgical wound debridement at the same hospital due to persistent wound complications. Despite this intervention, the wound continued to heal poorly, and the patient experienced persistent low back pain. He was subsequently treated with antibiotic therapy (ciprofloxacin) based on culture and sensitivity reports (Pseudomonas aeruginosa). Over the preceding 20 days, the patient developed progressively worsening low back pain with radiation to the left thigh and associated numbness, significantly limiting his mobility and daily activities. He therefore presented to our institution for further evaluation and management. On clinical examination, the patient was bedridden and unable to turn in bed due to severe pain. Local examination revealed a discharging sinus at the previous surgical site (Fig. 1) with marked tenderness over the lower lumbar spine.

Figure 1: Lower back of the patient with a previous surgical scar with a discharging sinus, when the patient presented to us (after microdiscectomy and a debridement surgery).
Neurological examination of the lower limbs revealed normal motor power, intact sensation, and preserved deep tendon reflexes. Based on clinical findings and radiological evaluation, the patient was diagnosed with chronic multilevel lumbar spondylodiscitis involving L3–L4, L4–L5, and L5–S1 with endplate erosions and spinal instability (Fig. 2, 3, 4).

Figure 2: Degenerative changes at L4 L5, L5 S1 level.
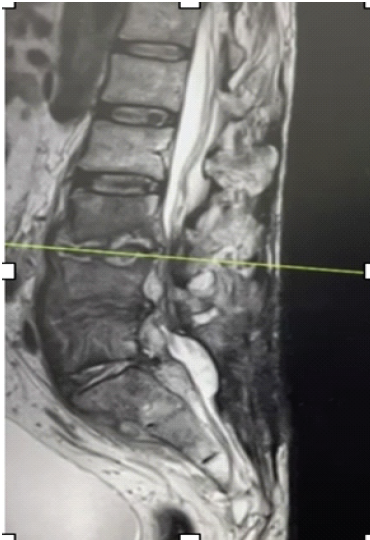
Figure 3: Magnetic resonance imaging T2-weighted sagittal cut showing spondylodiscitis L3L4, L4L5, and L5S1 levels.
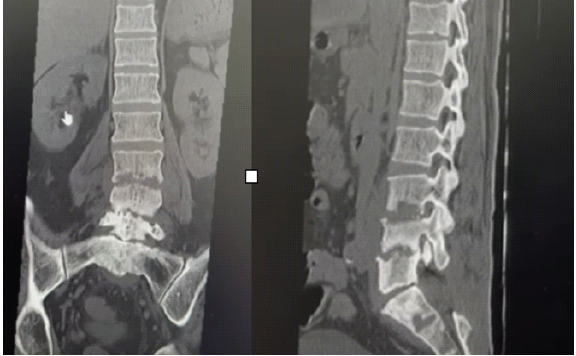
Figure 4: Computed tomography scan, coronal and sagittal cuts showing significant erosions at the end plates of L3, L4, and L5.
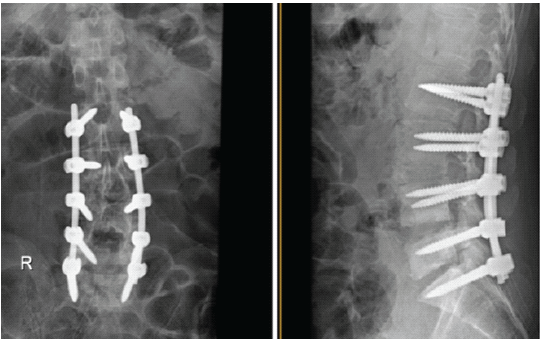
Figure 5: Post-operative X-ray of lumbosacral spine anteroposterior and lateral view showing L2 to S1 pedicle screw stabilization.
Considering the chronic infection and associated instability, the patient underwent surgical debridement, decompression, L2–S1 pedicle screw fixation, and posterolateral fusion (Fig. 5). Postoperatively, the patient showed significant symptomatic improvement and was mobilised on the 2nd postoperative day with walker support. Intraoperative pus culture revealed P. aeruginosa species, and targeted antibiotic therapy (aztreonam and avibactam) was initiated under the guidance of the infectious disease team. During follow-up, the patient demonstrated progressive clinical improvement with pain relief and was eventually able to walk independently without assistive support. Serial inflammatory markers showed a reduction in C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). The surgical wound healed well without further complications (Fig. 6).
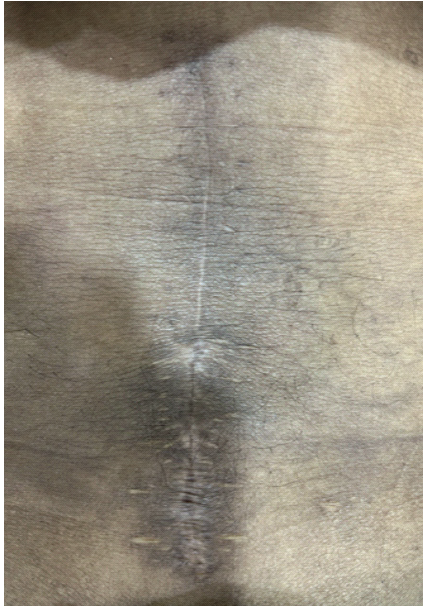
Figure 6: At 1-month follow-up, showing a well-healed surgical scar.
Case 2
A 41-year-old male presented with severe low back pain and progressive weakness of both lower limbs, resulting in difficulty performing routine daily activities. The patient had a history of low back pain with left lower limb radiculopathy approximately 6 months earlier, for which he had undergone an L4-L5 discectomy at another hospital. However, he continued to experience persistent pain following the surgery, and a repeat MRI evaluation was performed. Based on the findings, the patient underwent a second surgical procedure consisting of a repeat discectomy of the recurrent disc, 15 days after the primary surgery. During the post-operative period (20 days after the first surgery), the patient developed features of surgical site infection and subsequently underwent two wound washout procedures under anaesthesia at the same hospital. Despite these interventions, the surgical wound failed to heal properly, and the patient developed severe low back pain with progressive difficulty in ambulation. There were no associated bowel or bladder complaints. On clinical examination, an unhealed surgical wound with a discharging sinus was present over the lumbar region with local tenderness over the lumbar spine (Fig. 7).

Figure 7: Lower back of the patient with a previous surgical scar with a discharging sinus, when the patient presented to us (after 2 times microdiscectomy and 2 times washout surgery).
The patient was unable to walk due to severe pain and lower limb weakness. The straight leg-raising test was positive at 50° on the right side and 40° on the left side. Neurological examination revealed significant asymmetric motor weakness in both lower limbs, and sensory examination was normal. Knee, ankle, and plantar reflexes were normal bilaterally. Distal pulses were palpable. Based on clinical and radiological findings, the patient was diagnosed with L4-L5 spondylodiscitis with spinal instability (Figs. 8 and 9).
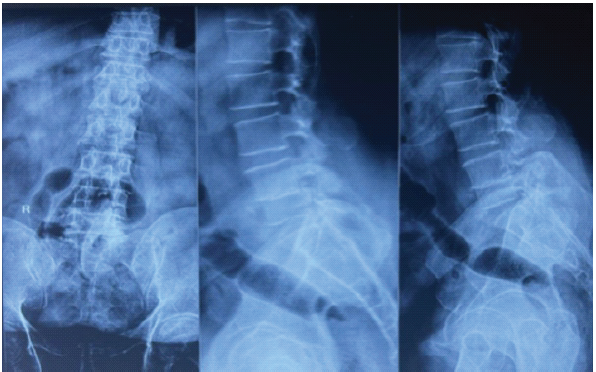
Figure 8: X-ray lumbar spine anteroposterior and lateral (flexion and extension) view showing degenerative changes and instability at the L4–L5 level.

Figure 9: Magnetic resonance imaging LS spine T2-weighted sagittal cut showing L4 L5 spondylodiscitis with dural compression and listhesis.
Considering the persistent infection, neurological deficit, and spinal instability, the patient underwent surgical debridement, decompression, pedicle screw fixation, and interbody fusion with antibiotic-coated bone stimulant granules (Figs. 10 and 11).
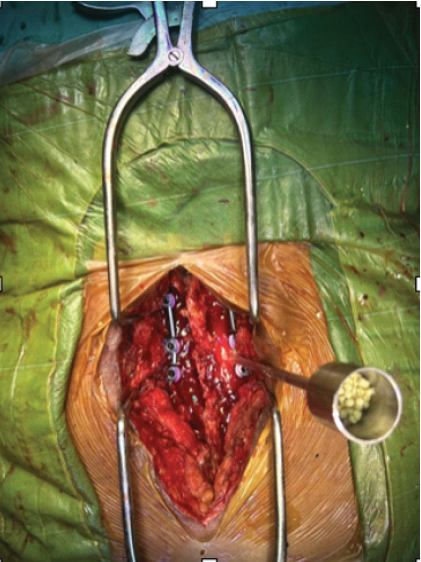
Figure 10: Filling of disc space with antibiotic-coated bone stimulant granules.
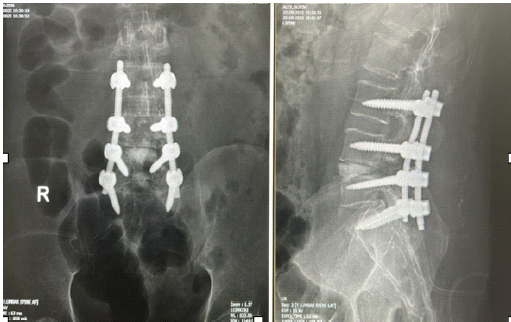
Figure 11: Post-operative X-ray lumbosacral spine anteroposterior and lateral views showing pedicle screw stabilization L3 to S1 with bone stimulants in L4L5 disc space.
Intraoperative samples were sent for microbiological analysis, and cultures revealed Escherichia coli growth. The patient was started on targeted antibiotic therapy (tigecycline for 7 days followed by doxycycline and clarithromycin for 3 weeks) according to culture sensitivity under the guidance of the infectious disease department. On follow-up, the surgical wound healed well, and the patient showed significant symptomatic improvement. Inflammatory markers, including CRP and ESR, demonstrated progressive reduction, indicating a favourable response to treatment.
Spondylodiscitis is an infection involving the intervertebral disc and adjacent vertebral bodies. It may be pyogenic (most common), tubercular, or fungal (rare). The primary treatment consists of appropriate antibiotic therapy according to culture and sensitivity, combined with spinal immobilisation. However, spinal stabilization becomes crucial in selected cases, particularly when there is spinal instability, neurological compromise, or failure of conservative treatment [1,2]. Infection of the spinal motion segment can lead to vertebral body destruction, disc space collapse, progressive kyphotic deformity, mechanical instability, and neural compression [3]. If instability progresses, patients may develop severe mechanical back pain, progressive deformity, and neurological deficits [4]. Spinal stabilisation is indicated in several clinical situations. One of the most important indications is mechanical instability, which may occur due to vertebral body collapse >50%, progressive kyphotic deformity, or severe mechanical pain that does not respond to conservative management [3,5]. Another major indication is the presence of neurological deficits, such as spinal cord or cauda equina compression, or when an epidural abscess causes neurological compromise [2,6]. Surgical stabilisation is also considered in cases of failure of conservative treatment, including persistent pain, persistent infection, or progressive vertebral destruction despite adequate antibiotic therapy [1,7]. Furthermore, extensive bony destruction, including multilevel involvement or posterior element involvement, may require stabilisation to restore the structural integrity of the spine [5]. The main goals of spinal stabilisation in spondylodiscitis include restoring spinal alignment, preventing progression of deformity, allowing early mobilisation, reducing mechanical pain, protecting neural elements, and improving antibiotic penetration by restoring mechanical stability [2,6]. Historically, surgeons avoided spinal instrumentation in the presence of infection due to concerns that implants could act as a nidus for persistent infection. However, current evidence suggests that instrumentation is safe in spinal infections when combined with adequate debridement and appropriate antibiotic therapy [8]. Instrumentation provides several advantages, including immediate spinal stability, promotes healing, early mobilisation, improved deformity correction, and better clinical outcomes compared to non-instrumented surgery [7,9]. Recent literature suggests that early stabilisation in spondylodiscitis can reduce hospital stay, improve functional outcomes, decrease deformity progression, and facilitate infection clearance [4,10].
Spinal stabilisation plays a crucial role in the management of spondylodiscitis by preventing motion at the pathological level, promoting healing, preventing progression of deformity, protecting neural structures, and facilitating early ambulation of the patient. Restoration of spinal stability also helps reduce mechanical pain and improves the overall functional outcome. Historically, the use of spinal instrumentation in the presence of infection was considered controversial; however, current evidence suggests that instrumentation can be safely performed when combined with thorough surgical debridement and appropriate antibiotic therapy. Therefore, surgical stabilisation together with targeted antimicrobial treatment is one of the effective strategies for managing spondylodiscitis.
Active post-operative spondylodiscitis is not a contraindication for instrumented stabilisation if combined with surgical debridement and appropriate antibiotic therapy.
References
- 1. Berbari EF, Kanj SS, Kowalski TJ, Darouiche RO, Widmer AF, Schmitt SK, et al. 2015 Infectious diseases society of America (IDSA) clinical practice guidelines for the diagnosis and treatment of native vertebral osteomyelitis in adults. Clin Infect Dis 2015;61:e26-46. [Google Scholar] [PubMed]
- 2. Kehrer M, Pedersen C, Jensen TG, Lassen AT. Increasing incidence of pyogenic spondylodiscitis: A 14-year population-based study. J Infect 2014;68:313-20. [Google Scholar] [PubMed]
- 3. Tali ET. Spinal infections. Eur J Radiol 2004;50:120-33. [Google Scholar] [PubMed]
- 4. Butler JS, Shelly MJ, Timlin M, Powderly WG, O’Byrne JM. Nontuberculous pyogenic spinal infection in adults: A 12-year experience from a tertiary referral center. Spine 2006;31:2695-700. [Google Scholar] [PubMed]
- 5. Ledermann HP, Schweitzer ME, Morrison WB, Carrino JA. MR imaging findings in spinal infections: Rules or myths? Radiology 2003;228:506-14. [Google Scholar] [PubMed]
- 6. Hadjipavlou AG, Mader JT, Necessary JT, Muffoletto AJ. Hematogenous pyogenic spinal infections and their surgical management. Spine (Phila Pa 1976) 2000;25:1668-79. [Google Scholar] [PubMed]
- 7. Dimar JR, Carreon LY, Glassman SD, Campbell MJ, Hartman MJ, Johnson JR. Treatment of pyogenic vertebral osteomyelitis with anterior debridement and fusion followed by delayed posterior spinal fusion. Spine (Phila Pa 1976) 2004;29:326-32; discussion 332. [Google Scholar] [PubMed]
- 8. Rayes M, Colen CB, Bahgat DA, Higashida T, Guthikonda M, Rengachary S, et al. Safety of instrumentation in patients with spinal infection. J Neurosurg Spine 2010;12:647-59. [Google Scholar] [PubMed]
- 9. Suess O, Weise L, Brock M, Kombos T. Debridement and spinal instrumentation as a single-stage procedure in bacterial spondylitis. Zentralbl Neurochir 2007;68:123-32. [Google Scholar] [PubMed]
- 10. Lambert A, Charles YP, Ntilikina Y, et al. Percutaneous instrumentation combined with antibiotic treatment in spondylodiscitis. Orthop Traumatol Surg Res 2019;105:1165-70. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2025 Case Report – Surgical Management and Neurological Recovery in an 18-Year-Old Male with C4-C5 Cervical Spine Fracture
July 1, 2025 Case Report – Surgical Management and Neurological Recovery in an 18-Year-Old Male with C4-C5 Cervical Spine Fracture February 1, 2025 Computed Tomography Guided Biopsy and Gene X-pert MTB/Rif Ultra can be Deceptive in Spondylodiscitis – A Rare Case Report of Hodgkin’s Lymphoma Mimicking Spondylodiscitis
February 1, 2025 Computed Tomography Guided Biopsy and Gene X-pert MTB/Rif Ultra can be Deceptive in Spondylodiscitis – A Rare Case Report of Hodgkin’s Lymphoma Mimicking Spondylodiscitis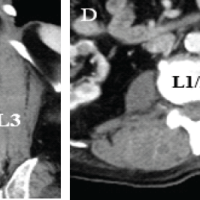 January 1, 2025 A Rare Case of the Ipsilateral Paraspinal Muscle Abscess Communicating with a Psoas Major Abscess: A Case Report
January 1, 2025 A Rare Case of the Ipsilateral Paraspinal Muscle Abscess Communicating with a Psoas Major Abscess: A Case Report December 1, 2024 Management of Thoracolumbar Spinal Tuberculosis by Decompression and Posterior Stabilization with Pedicle Screw Fixation
December 1, 2024 Management of Thoracolumbar Spinal Tuberculosis by Decompression and Posterior Stabilization with Pedicle Screw Fixation