
The post-traumatic form of hemosiderotic synovitis is rare and difficult to diagnose due to its resemblance to pigmented villonodular synovitis, which underscores the necessity of the histopathological confirmation of the diagnosis and treatment.
Dr Aisha Wasi, Tarmeem Orthopaedic and Spine Speciality Hospital, Abu Dhabi, United Arab Emirates. E-mail: research.ethics@tarmeem.com
Abstract
Introduction: Hemosiderotic synovitis (HS) is a rare proliferative disease of the synovium, which is mainly associated with haemophilia and hemarthrosis. The non-haemophilic, post-traumatic form of HS is not common and tends to resemble pigmented villonodular synovitis (PVNS) both in clinical aspects and radiographic evaluations. Though HS is reported in adults, literature covering the condition in younger patients is limited, and this may be one of the factors that lead to delays in the diagnosis and consequent inappropriate therapeutic procedures.
Case Report: A 10-year-old male experiencing discomfort, effusion, and restricted knee motion following a football-associated trauma. Magnetic resonance imaging examinations initially raised suspicion of diffuse PVNS. Nonetheless, histopathological assessment established a definitive diagnosis of post-traumatic HS, with no indicators of PVNS or neoplastic changes evident. Management involved arthroscopic synovectomy, which led to substantial clinical and radiological improvements post-surgery, along with no recurrence of symptoms.
Conclusion: Post-traumatic HS manifests itself as an extremely rare condition in children. It is essential to note that it exists, and it is clinically and radiologically similar to PVNS. Histopathological approaches remain the most reliable diagnostic tool. The recording of such cases is important in supplementing the poor paediatric data and promoting the early diagnosis and appropriate therapy modalities.
Keywords: Hemosiderosis, synovitis, pigmented villonodular synovitis, knee joint, child, arthroscopy, histopathology.
A thin white layer, which includes numerous projections in the form of villi, is referred to as the synovium [1]. The synovium also has the role of the transportation of nutrients and the removal of waste and immune modulation. Hemosiderotic synovitis (HS) is a proliferative disease, which is marked by repeated bleeding into the joint cavity causing joint inflammation [2]. The development of hyperplastic vascular tissue takes place under several days after the bleeding. Due to the degradation of the haemoglobin found in the tissue, the release of iron-carrying hemosiderin is discharged inside the tissue [3]. This hemosiderin builds up, resulting in a rusty brown tissue discolouration [2]. The production of proinflammatory cytokines and capacity to prevent the development of human cartilage matrix also relate to the iron deposited [4]. The joint that is mostly affected is the knee, and the most common cause has been cited to relate to a lack of clotting factors. HS clinically and radiographically imitates pigmented villonodular synovitis (PVNS) to cause diagnostic confusion [5]. The HS and PVNS can be distinguished against one another when under histopathological inspection. In the case of PVNS, a histological mosaic of proliferative nodules can be found in the villus, whereas in the case of HS, reactive changes can be observed [6,7]. The frequency of misdiagnosis highlights the importance of conducting thorough case studies in this field. In this case report, we present a diagnostically challenging case from the UAE of a child with a monoarticular knee effusion where magnetic resonance imaging (MRI) findings were highly suggestive of PVNS.
A 10-year-old boy reported having progressive left knee pain, swelling, and limitation of movement 2 months following a traumatic injury during a soccer match. On clinical examination, left knee effusion and painful loss of active and passive knee movement were observed (Fig. 1).

Figure 1: Clinical photographs demonstrating left knee effusion and restricted range of motion associated with hemosiderotic synovitis.
The laboratory tests showed that the patient had a slightly high erythrocyte sedimentation rate, and rheumatology was normal. Radiographic examination depicted no destructive changes with preserved bony architecture. There is slight fullness in the suprapatellar region that indicates effusion of the joint (Fig. 2).
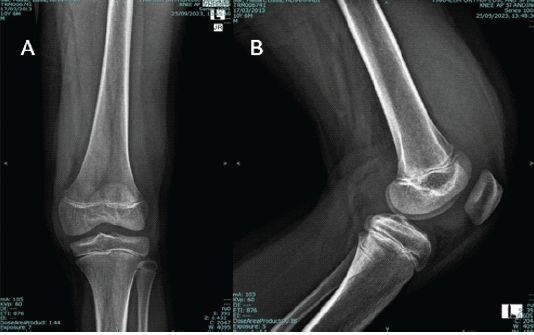
Figure 2: Radiographic examination of the left knee demonstrating preserved bony architecture with no destructive changes. Subtle soft-tissue fullness in the suprapatellar region is suggestive of joint effusion.
Knee MRI revealed a large knee joint effusion with diffuse low signal intensity villous synovial hypertrophy, as well as a large popliteal cyst with the same appearance, which supports the diagnosis of diffuse-form PVNS (Fig. 3).
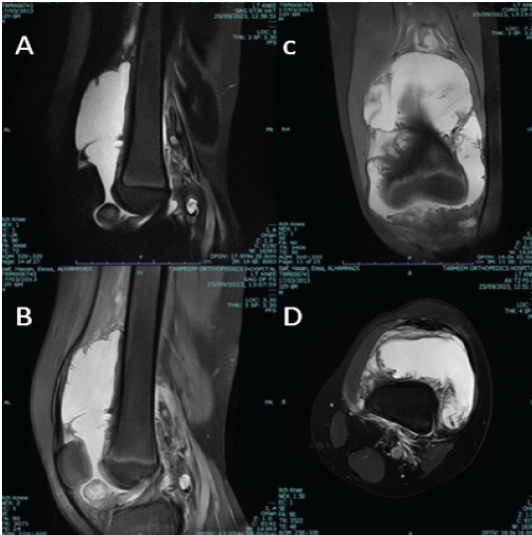
Figure 3: Magnetic resonance imaging of the left knee before synovectomy. (a and b) Sagittal proton density fat-saturated images demonstrate a large joint effusion with diffuse villous synovial hypertrophy of low signal intensity. (c) Coronal view showing extensive synovial thickening with low-signal areas due to hemosiderin deposition. (d) Axial view revealing circumferential synovial proliferation with joint effusion.
Total arthroscopic synovectomy was performed without complications. Intraoperatively, a large effusion containing yellow clots was observed. The histopathological assessment confirmed the diagnosis as post-traumatic non-haemophilic HS (Fig. 4).
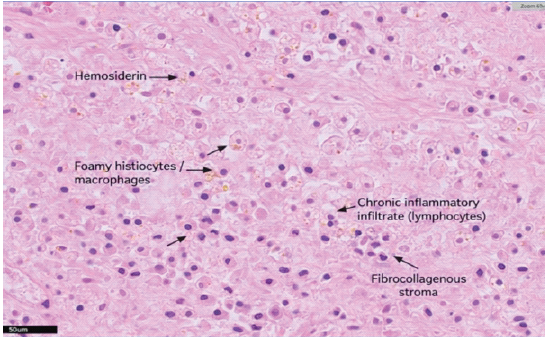
Figure 4: Histopathological section of synovial tissue (hematoxylin and eosin stain, ×400) demonstrating hemosiderin-laden macrophages, foamy histiocytes/macrophages, chronic inflammatory infiltrate (lymphocytes), and fibrocollagenous stroma, consistent with hemosiderotic synovitis. No evidence of stromal proliferation, multinucleated giant cells, or xanthoma cells characteristic of pigmented villonodular synovitis is seen.
A characteristic rusty-brown gross appearance of the synovium, indicative of haemosiderin deposition, was also evident (Figs. 5 and 6). The patient showed significant clinical and radiological improvement postoperatively with no evidence of recurrence.
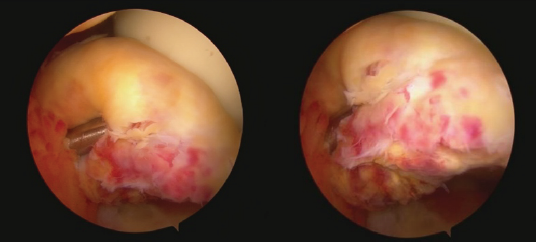
Figure 5: Arthroscopic view of the left knee joint revealing hypertrophied synovium with brownish discoloration from hemosiderin deposition and the presence of intra-articular effusion containing yellowish clots.

Figure 6: Excised synovial tissue specimen obtained during arthroscopic synovectomy, showing brownish discoloration due to hemosiderin deposition.
HS is most commonly caused due to hereditary factors such as deficiency of clotting factors. Other causes of HS are also through the use of oral anticoagulants and degenerative and inflammatory arthritis, such as osteoarthritis, psoriatic arthritis, and collagen vascular diseases [7]. Post-traumatic non-haemophilic synovitis is a rare subtype of the HS, which develops as a result of intra-articular blood loss as a consequence of trauma. It resembles PVNS in both clinical and radiological appearance, as represented in this case. The rusty brown gross appearance also resembles it under both conditions. Histopathological examination is essential for differentiation between the two conditions [8]. Early diagnosis is the key to the management of this type of HS. A radiologist’s familiarity with this rare condition is an essential factor of early diagnosis and avoiding unnecessary invasive intervention. The present case depicts the development of HS in the absence of bleeding disorder and a positive history of trauma, defining it as a post-traumatic non-haemophilic HS. This emphasises the importance of considering HS in differential diagnosis in cases of joint effusion and pain, even in the absence of blood disorders. The MRI results showed the diffuse PVNS, the most frequent alternative diagnosis. This similarity is possible because the two disorders are characterised by reduced signal intensity in all the sequences, and these are characterised by the accumulation of hemosiderin in the synovium [5,9]. As it has been pointed out, imaging is not able to reliably differentiate between PVNS and HS; hence, additional confirmation with the help of histopathology should be emphasised [10]. Histopathology continues to serve as the gold standard of diagnosis in such cases. As opposed to PVNS, multicellular stromal cell proliferation, multinucleated giant cells, and foam cells, HS typically involves reactive synovial overgrowth with haemosiderin-laden macrophages and fibrosis without tumour-like characteristics [3,6]. Moreover, in the case of PVNS, the synovial thickening and nodular proliferation can be visualised around the posterior compartment predominantly along with an association with a popliteal cyst (Baker’s cyst). However, in the case of HS, the synovial thickening is found in the suprapatellar region, as depicted in this case. This case was confirmed by post-traumatic non-haemophilic HS on histologic evaluation. Such distinction is of clinical importance since PVNS is aggressive locally and often recurrent, whereas HS is caused due to reactive processes and often predicts a better outcome. The choice of management tends to be based on the severity and clinical progression. Arthroscopic synovectomy was done on this case, and it resulted in a clinical and radiological improvement with no recurrence after a short period of observation. Synovectomy is effective in controlling haemorrhage and synovial proliferation [11,12]. HS recurses much less frequently than PVNS, especially after root causes (such as injury or instability) have been addressed. In the present case, the onset of symptoms was followed by a history of trauma sustained during football, which supports the traumatic aetiology leading to synovial proliferation and the subsequent haemosiderin deposition. While haemophilia and recurrent bleeding into joints are the classic associations of HS, post-traumatic HS has been observed in people without haemophilia [4]. It is important to note that the precipitating factor does not necessarily have to be a major injury [5,7]. Hence, detailed history-taking is essential to identify possible sources of minor yet repetitive microtrauma, such as sports overuse, twisting injuries, frequent kneeling, physiotherapy manipulation, or vigorous massage around the joint [7,8,9]. From an epidemiological standpoint, the non-haemophilic variant of HS is still uncommon, especially in children. The actual incidence is not fully established due to scarce published data and most reports consisting of only isolated cases or smaller series [5,7,9,12]. Due to these reasons, along with hemosiderin-related low signal intensity, it sheds light on why HS can be misdiagnosed as PVNS, highlighting the importance of histopathological confirmation [6,10]. To the best of our knowledge, this is the reporting of the first associated case of post-traumatic HS mimicking PVNS in a non-haemophilic child of the United Arab Emirates; hence, we need to be aware and have histopathological validation in under-reported groups. This report supplements the scarcity of literature on post-traumatic HS among paediatric patients, particularly in this region. Prior case reports outline similar cases in which children manifested HS post-knee trauma; in all cases, histopathological assessment was crucial for the diagnosis [5,7,8,12]. This emphasises the need to consider HS as a potential factor that leads to long-term monoarthritis in non-haemophilic children by clinicians and radiologists. Early detection and surgery would prevent the degeneration of the joint and permanent immobility.
Post-traumatic HS represents an extremely rare diagnosis, particularly common among children. The importance of awareness on this unusual subtype is in the fact that it is a difficult diagnosis and leads to diagnostic confusion because it radiologically mimics PVNS. Therefore, histopathology is necessary to distinguish between PVNS and HS, where HS exhibits reactive synovial hyperplasia of haemosiderin-containing macrophages, whereas PVNS is characterised by stromal proliferation, giant cells, and foam cells. In our case, MRI findings inclined to indicate PVNS, but histopathology indicated HS. Arthroscopic synovectomy treatment was administered to the patient successfully, and the patient had a good outcome without any trace of recurrence.
The post-traumatic variant of hemosiderotic synovitis can mimic pigmented villonodular synovitis even in non-haemophilic children, and awareness of this entity can prevent misdiagnosis and guide appropriate surgical and histopathological management.
References
- 1. O’Connell JX. Pathology of the synovium. Am J Clin Pathol 2000;114:773-84. [Google Scholar] [PubMed]
- 2. Humphrey PA, Dehner LP, Pfeifer JD. The Washington Manual of Surgical Pathology. Philadelphia, PA: Lippincott Williams and Wilkins; 2008. p. 804. [Google Scholar] [PubMed]
- 3. France MP, Gupta SK. Nonhaemophilic hemosiderotic synovitis of the shoulder. A case report. Clin Orthop Relat Res 1991;262:132-6. [Google Scholar] [PubMed]
- 4. Roosendaal G, Vianen ME, Wenting MJ, Van Rinsum AC, Van Den Berg HM, Lafeber FP, et al. Iron deposits and catabolic properties of synovial tissue from patients with haemophilia. J Bone Joint Surg Br 1998;80:540-5. [Google Scholar] [PubMed]
- 5. Khasawneh RA, Mohaidat ZM, Gharaibeh MM, Hdeeb A. Post-traumatic hemosiderotic synovitis of the knee mimicking pigmented villonodular synovitis on magnetic resonance imaging (MRI) in a child: A case report. Am J Case Rep 2021;22:e931992. [Google Scholar] [PubMed]
- 6. Murphey MD, Rhee JH, Lewis RB, Fanburg-Smith JC, Flemming DJ, Walker EA. Pigmented villonodular synovitis: Radiologic-pathologic correlation. RadioGraphics 2008;28:1493-518. [Google Scholar] [PubMed]
- 7. Jayalakshmi V, Chikhale NP, Mishra A, Cherian S. Nonhemophilic hemosiderotic synovitis of the knee: A case report and review of literature. Indian J Pathol Microbiol 2014;57:473-5. [Google Scholar] [PubMed]
- 8. Yalçin N, Bektaşer B, Ciçekli O, Uğraş S, Doğan M. An unusual cause of recurrent joint effusions: Nonhemophilic hemosiderotic synovitis of the knee. Acta Orthop Traumatol Turc 2010;44:162-5. [Google Scholar] [PubMed]
- 9. Zeiss J, Booth RL Jr., Woldenberg LS, Saddemi SR. Post-traumatic synovitis presenting as a mass in the suprapatellar bursa of the knee. MRI appearance. Clin Imaging 1993;17:81-5. [Google Scholar] [PubMed]
- 10. Sannananja B, Shah HU, Laxman V, Nagesh C. PVNS or pseudoaneurysm: MRI problem-solving or misleading? Indian J Radiol Imaging 2015;25:60-2. [Google Scholar] [PubMed]
- 11. Sim FH. Synovial proliferative disorders: Role of synovectomy. Arthrosc 1985;1:198-204. [Google Scholar] [PubMed]
- 12. Jain VK, Singh RK, Kumar S, Netam SS, Jain SG, Shah PJ. Hemosiderotic synovitis: Highlighting the role of the T2* weighted sequence in skeletal MRI. Egypt J Radiol Nucl Med 2016;47:1511-3. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Management of a Rare Combined Osseoligamentous Knee Injury: Tibial Plateau Fracture with High-Grade Posterior Cruciate Ligament Tear Treated by Arthroscopic Reconstruction and Osteosynthesis – A Case Report
April 1, 2026 Management of a Rare Combined Osseoligamentous Knee Injury: Tibial Plateau Fracture with High-Grade Posterior Cruciate Ligament Tear Treated by Arthroscopic Reconstruction and Osteosynthesis – A Case Report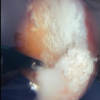 February 1, 2026 Gouty Arthritis Versus Chondrocalcinosis in a Stiff Knee, A Diagnostic Dilemma – A Case Report
February 1, 2026 Gouty Arthritis Versus Chondrocalcinosis in a Stiff Knee, A Diagnostic Dilemma – A Case Report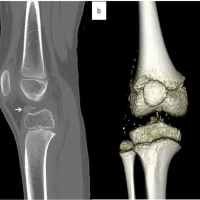 March 10, 2024 Pediatric Synovial Osteochondromatosis of the Knee with Leg Length Discrepancy: A Case Report
March 10, 2024 Pediatric Synovial Osteochondromatosis of the Knee with Leg Length Discrepancy: A Case Report July 1, 2026 Lipoma Arborescens of the Knee: An Intraoperative Mimicker of Pigmented Villonodular Synovitis in Bilateral Knee Osteoarthritis – A Case Report
July 1, 2026 Lipoma Arborescens of the Knee: An Intraoperative Mimicker of Pigmented Villonodular Synovitis in Bilateral Knee Osteoarthritis – A Case Report