
Lipoma Arborescens can masquerade as pigmented villonodular synovitis intraoperatively during a total knee arthroplasty. Total synovectomy results in a favorable outcome with minimal recurrence, unlike pigmented villonodular synovitis
Dr. Nirav Rajesh Gupta, Apex Superspeciality Hospital, Mumbai, Maharashtra, India. E-mail: drniravortho@gmail.com
Abstract
Introduction: Lipoma arborescens (LA) is a rare benign synovial lesion characterised by villous fatty proliferation. Intraoperatively, it may mimic pigmented villonodular synovitis (PVNS) due to a similar frond-like, vascular synovial appearance.
Case Report: We report a 74-year-old male with bilateral grade 4 knee osteoarthritis who underwent total knee arthroplasty. Diffuse villous synovial tissue was encountered intraoperatively, with unexpected bleeding despite tourniquet use. Histopathology confirmed LA. Intra-articular administration of tranexamic acid effectively controlled the bleeding.
Conclusion: The clinical outcome is favourable in most cases, unlike with PVNS.
Keywords: Lipoma arborescens, total knee arthroplasty, pigmented villonodular synovitis, frond-like growth, synovial hypertrophy
Lipoma arborescens (LA) is a rare non-neoplastic synovial lesion marked by villous sub-synovial fatty proliferation, typically in the suprapatellar pouch of the knee [1]. It has an unknown aetiology and is hypothesised to arise secondary to chronic irritation such as osteoarthritis, rheumatoid arthritis, or trauma [2]. Clinically, patients present with progressive swelling, effusion, and limitation in knee motion. Although histologically distinct, inflamed LA closely resembles pigmented villonodular synovitis (PVNS) intraoperatively due to villous morphology and bleeding tendency [3]. PVNS, also known as diffuse tenosynovial giant cell tumour, is a proliferative disorder of the knee characterised by hemosiderin-laden macrophages, multinucleated giant cells, and hypervascular synovium. PVNS can cause pain, stiffness, and joint destruction, with recurrence rates up to 46% even after total synovectomy [4]. This can complicate surgical management during a total knee arthroplasty (TKA), making it important to differentiate from its mimickers.
A 75-year-old male presented to the outpatient department with progressive bilateral knee pain, varus deformity, and restricted range of motion of 5 years’ duration, with the left side affected more than the right. Standing anteroposterior and lateral radiographs of both knees revealed grade 4 osteoarthritis (Kellgren–Lawrence grading) with bone-on-bone attrition, worse on the left (Fig. 1a and b).

Figure 1: Pre-operative anteroposterior (a) and lateral (b) radiograph of the knee. It is suggestive of Grade 4 osteoarthritis with bone-on-bone attrition, left more than right.
The patient was planned for bilateral TKA as per standard guidelines. The left side, being more painful, was operated on first, and post-knee arthrotomy, a diffuse thickened, villous, yellow-brown synovial tissue hypertrophy was noted, mimicking a PVNS (Fig. 2).
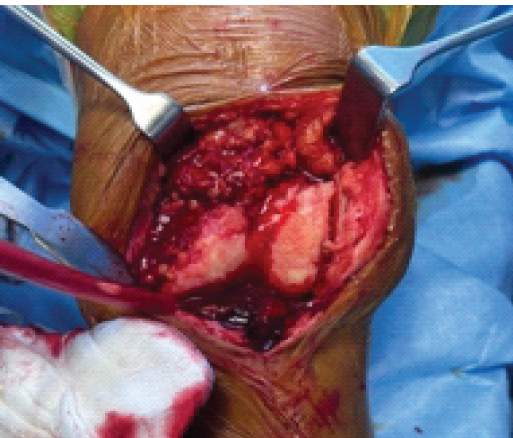
Figure 2: Intraoperative picture of the left knee. Diffuse thickened villous hypertrophy of synovium with active bleeding can be seen. Note tourniquet was inflated at 300 mmHg pressure. Constant suction and mopping were necessary while clicking the photo to get a clear image.
Despite a properly inflated tourniquet at 300 mmHg, significant bleeding occurred from the hypertrophic synovium and adjacent tissues. Intra-articular tranexamic acid (TXA), 1 g, was injected, and total synovectomy was performed once the bleeding was controlled. Further, a posterior-stabilised TKA was completed as routine. A drain was inserted. The other side’s TKA surgery was postponed. Excised synovial tissue was sent for histopathological examination. Postoperatively, intravenous TXA, 1 g 12 hourly, was given for 3 days. In-bed knee mobilisation was started on the same evening, and the patient was made to walk the next morning. This helped in preventing deep vein thrombosis, as blood thinners could not be used. Drain output was recorded as 180 mL, 140 mL, and 70 mL on the 1st, 2nd, and 3rd day, respectively. The drain was removed on the 3rd day. The histopathological examination revealed villous synovial fronds with subsynovial replacement by mature adipocytes and mild chronic inflammation, but no haemosiderin deposits, multinucleated giant cells, or stromal hypercellularity, confirming a diagnosis of LA (Fig. 3).
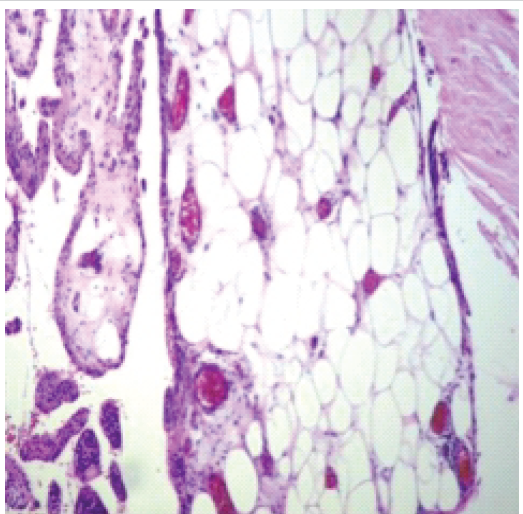
Figure 3: Histopathological examination. Fibrocollagenous and fibroadipose tissue lined by synovial epithelium exhibiting papillary hyperplasia and subepithelial stroma suggestive of lipoma arborescens can be seen. No hemosiderin or multinucleated giant cells were seen ruling out pigmented villonodular synovitis.
After 7 days, the right side TKA was planned. In anticipation of similar findings on the right side, pre-operative intravenous TXA was given 30 min before the incision. In addition, 1 g TXA was injected intra-articularly. A similar but milder villonodular synovial tissue was noted in the right suprapatellar pouch post-arthrotomy (Fig. 4). Total synovectomy was repeated, and TKA was performed uneventfully (Fig. 5a and b). Drain output was similar (130 mL → 90 mL → 50 mL). At the 1-year follow-up, the patient had an excellent outcome with no recurrence of LA.
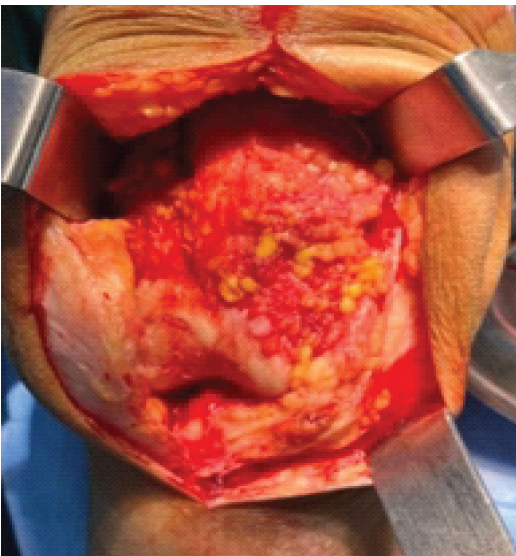
Figure 4: Intraoperative picture of the right knee. A less extensive villous hypertrophy of the synovium compared to the left side can be seen. The bleeding is not active as pre-operative tranexamic acid was administered intravenously and intra-articularly.
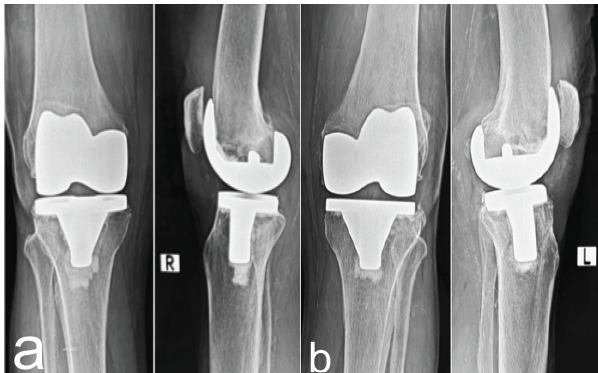
Figure 5: Post-operative X-rays. It shows corrected varus deformity and optimal prosthesis alignment at 1-year follow-up, right knee (a) and left knee (b).
Synovial lipomatosis was first reported and documented in literature by Hoffa in 1904, who described the condition as “giant synovial osteochondromatosis” [5]. “Arborescens” in Latin means “tree-like appearance”, describing the villous and frond-like morphology seen in this condition [6]. Two etiological types of LA have been described, primary and secondary, depending on the age of onset and the underlying precipitating condition. The secondary type is more common and is defined as lipomatosis associated with a chronic synovial irritation due to degenerative disease, meniscal injury, trauma or synovitis and is usually seen in elderly patients, as in our case [7,8]. Detailed radiological examination helps to differentiate it from its mimickers. The absence of articular surface erosions and sclerosis on plain radiographs serves as an important clue in ruling out PVNS and gouty arthropathy [1]. Probe compression during an ultrasound (USG) demonstrates the soft consistency of the lesion as opposed to the non-compressible and firm nature of PVNS. A computed tomography shows the absence of ossified loose bodies in the hypertrophied synovium and high-attenuating soft tissue, differentiating LA from closely mimicking synovial osteochondromatosis and PVNS, respectively [1]. Magnetic resonance imaging (MRI) is usually diagnostic, with LA showing high signal intensity villous foci on both T1-weighted (T1W) and T2-weighted (T2W) images. They suppress short tau inversion recovery (STIR) or fat saturation sequences, similar to those of any subcutaneous fat. The remaining non-fatty component displays a heterogeneous high signal intensity on T2W or STIR sequences and intermediate-to-low signal intensity on T1W sequences. The absence of artefacts related to hemosiderin deposits on gradient imaging differentiates it from PVNS, an otherwise closely mimicking entity [1]. In our case, a USG or MRI was not performed, as the presentation was dominated by the findings of osteoarthritis. PVNS is a benign but locally aggressive lesion that requires more extensive resection and still carries a high recurrence rate, especially with diffuse types, older ages, and knee involvement, complicating the outcomes of TKA with postoperative stiffness and reduced motion [9]. Adjuvant radiotherapy may help in reducing local recurrence [10]. LA, on the other hand, has a very low risk of recurrence and a favourable outcome as seen in our case.
This case highlights that LA can masquerade as PVNS intraoperatively, particularly in osteoarthritic knees with chronic inflammation. MRI and histopathology are crucial for accurate diagnosis. Intra-articular TXA provides a valuable haemostatic adjunct during TKA when unexpected synovial bleeding is encountered. Combined synovectomy and TKA yields excellent outcomes with minimal recurrence in LA.
Surgeons should be aware of the mimickers of villous synovial hypertrophy. Histopathological diagnosis helps in targeted treatment and alleviates the associated anxiety among the patients. Overall prognosis is better explained, and compliance improves.
References
- 1. Sanamandra SK, Ong KO. Lipoma arborescens. Singapore Med J 2014;55:5-10; quiz 11. [Google Scholar] [PubMed]
- 2. Tsifountoudis I, Kapoutsis D, Tzavellas AN, Kalaitzoglou I, Tsikes A, Gkouvas G. Lipoma arborescens of the knee: Report of three cases and review of the literature. Case Rep Med 2017;2017:3569512. [Google Scholar] [PubMed]
- 3. Patel AC, Jain K, Chugh S, Buddha K. Lipoma arborescens: A rare cause of knee swelling. J Orthop Case Rep 2022;12:56-60. [Google Scholar] [PubMed]
- 4. Mollon B, Lee A, Busse JW, Griffin AM, Ferguson PC, Wunder JS, et al. The effect of surgical synovectomy and radiotherapy on the rate of recurrence of pigmented villonodular synovitis of the knee: An individual patient meta-analysis. Bone Joint J 2015;97-B:550-7. [Google Scholar] [PubMed]
- 5. Thavasianantham K, Raagul TS, Ganesh A, Elangovan P, Haemanath P, Regunathan PS. Unusual presentation of synovial lipomatosis mimicking septic arthritis of the knee: A case report. Cureus 2024;16:e58075. [Google Scholar] [PubMed]
- 6. Yan CH, Wong JW, Yip DK. Bilateral knee lipoma arborescens: A case report. J Orthop Surg (Hong Kong) 2008;16:107-10. [Google Scholar] [PubMed]
- 7. Al-Ismail K, Torreggiani WC, Al-Sheikh F, Keogh C, Munk PL. Bilateral lipoma arborescens associated with early osteoarthritis. Eur Radiol 2002;12:2799-802. [Google Scholar] [PubMed]
- 8. Plotkin BE, Varma R. Lipoma arborescens of the knee in a 17-year-old man. Radiology Case Reports 2008;3:164. [Google Scholar] [PubMed]
- 9. Aljuhani W, Alamri A, Altorbak B, Alabbasi J, Ahmed F. Patient outcomes after resection of pigmented villonodular synovitis in patients in King Abdulaziz Medical City. Cureus 2024;16:e68248. [Google Scholar] [PubMed]
- 10. Heyd R, Micke O, Berger B, Eich HT, Ackermann H, Seegenschmiedt MH; German Cooperative Group on Radiotherapy for Benign Diseases. Radiation therapy for treatment of pigmented villonodular synovitis: results of a national patterns of care study. Int J Radiat Oncol Biol Phys. 2010 Sep 1;78(1):199-204. doi: 10.1016/j.ijrobp.2009.07.1747. Epub 2010 May 18. PMID: 20488628. [Google Scholar] [PubMed] [CrossRef]





Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report
August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report August 1, 2026 Intrawound Vancomycin and Povidone-Iodine Treatment to Reduce Infection Rates in Arthroplasty
August 1, 2026 Intrawound Vancomycin and Povidone-Iodine Treatment to Reduce Infection Rates in Arthroplasty July 1, 2026 Post-traumatic Hemosiderotic Synovitis Mimicking Pigmented Villonodular Synovitis in a Non-hemophilic Child: First Reported Case from the United Arab Emirates
July 1, 2026 Post-traumatic Hemosiderotic Synovitis Mimicking Pigmented Villonodular Synovitis in a Non-hemophilic Child: First Reported Case from the United Arab Emirates July 1, 2026 Megaprosthetic Total Knee Arthroplasty for Supracondylar Refracture in a Post-traumatic Osteoarthritic Knee: A Case Report
July 1, 2026 Megaprosthetic Total Knee Arthroplasty for Supracondylar Refracture in a Post-traumatic Osteoarthritic Knee: A Case Report