
An unusual presentation of an osteoarticular lytic lesion as a solitary bone plasmacytoma of the appendicular skeleton, especially distal to the elbow and knee joint, although very rare, cannot be misdiagnosed if one evaluates the patient with a multidisciplinary approach and keeps a wide spectrum of differential diagnoses in queue.
Dr Ashish Garg, Department of Orthopaedics, Adesh Medical College and Hospital, Kurukshetra, Haryana, India. E-mail: ashishgarg30011993@gmail.com
Abstract
Introduction: Solitary plasmacytoma is an infrequent form of plasma cell (PC) dyscrasia which presents as a single mass of monoclonal PCs, located either intraosseous or extramedullary. Solitary bone plasmacytoma (SBP) is characterised by a mass of neoplastic monoclonal PCs primarily occurring in the axial skeleton without systemic involvement. This case delineated an unusual appendicular-osteoarticular (wrist joint) involvement, which was diagnosed through an exhaustive set of investigations and managed by radiotherapy (RT), which is the standard of care. The rarity of the clinico-radiological presentation makes this case noteworthy.
Case Report: The present case highlights an unusual clinico-radiological finding of SBP involving the left wrist joint in a 45-year-old male patient. The patient presented with non-traumatic, chronic pain and swelling of the left wrist joint with restricted range of motion. Radiological investigations showed multiple osteoarticular lytic lesions, and histopathology revealed binucleated sheets of PCs, “Mott cells” and Russell bodies in bony trabeculae, which clinched the diagnosis as PC dyscrasias. Interestingly, multiple intracytoplasmic crystalline inclusions were found in this case, which is a quite rare entity as per SBP and warrants further investigations to rule out other PC dyscrasias, such as multiple myeloma (MM). Immunofixation electrophoresis was done to confirm the monoclonality, that is, light chain restriction (increased immunoglobulin G kappa), of the tumour. Immunohistochemical marker evaluation was positive for CD138 and CD38. Further investigations were done to rule out MM (details tabulated in the report). The patient was managed with RT as per International Myeloma Working Group (IMWG) guidelines. Being notorious for a higher risk for progression to MM for SBP patients (65–84% at 10 years), we did continuous monitoring of the patient post-radiation therapy as per IMWG guidelines.
Conclusion: SBP of the appendicular skeleton, especially distal to the elbow, as seen in this case, is very rare in adults. In such scenarios, a multidisciplinary approach of extensive radiological, biochemical, histopathological, and immunohistochemical investigations to rule out the differential diagnosis is the key to eschewing misdiagnosis. Prompt treatment and strict follow-up are the prerequisites for a favourable outcome and to prevent progression into MM, which is a more aggressive entity and lies at the other end of the spectrum of PC dyscrasias.
Keywords: Solitary bone plasmacytoma, plasma cell dyscrasia, multiple myeloma, wrist joint, International Myeloma Working Group.
Osteoarticular lytic lesions are still a diagnostic mystery, especially when they occur at unusual sites. The solitary plasmacytoma (SP) is characterised by a localised accumulation of neoplastic monoclonal plasma cells (PCs) without apparent systemic manifestations. It can manifest as extramedullary (extraosseous) plasmacytoma (EMP), that is, in soft tissues or as solitary bone plasmacytoma (SBP), which arises from PC infiltration of the bone marrow. SBP affects <5% of the patients with PC myeloma [1]. The median age of the patients with SP is 55 years. The male-to-female ratio of SP is 2:1 [2]. Thoracic vertebrae are most commonly involved, followed by the skull, the clavicle, and the sternum [3]. Involvement of extremities distal to the elbow and the knee joints is rare [4]. Pain at the site of the parent lesion in the bone is the most common symptom at presentation [4]. A correct diagnosis is important as SBP has a significantly higher risk of progression to multiple myeloma (MM) (65–84% in 10 years) [5,6]. Ruling out other differentials, such as tuberculosis, enchondroma, MM, non-Hodgkin lymphoma, reactive plasmacytosis, and plasmablastic lymphoma, is equally necessary to avoid a wrong diagnosis. Furthermore, to differentiate the overlapping conditions, such as reactive plasmacytosis and other lymphoproliferative disorders, certain histopathological features can be looked upon, such as clonality, cytology, infiltration pattern, and immunophenotype [7]. Although there are 12 cases that have been published till now for SBP in the appendicular skeleton, only one case (SBP of calcaneum) has been completely treated with radiotherapy (RT) alone [8]. This is the second of its kind (first in the upper limb below the elbow joint), where only RT as per the recommended dose resulted in resolution of the disease. Across this case report, the author intends to enlighten the readers about some rare presentations of this rare disease, aiding in the diagnosis if such a state of dilemma exists.
A 45-year-old male presented with pain and swelling at the left wrist joint, which was insidious in onset and gradually progressing over a period of 9 months. There was no history suggestive of any trauma or any associated systemic disease. Pain was aggravated by movement and relieved by medication. On examination, there was tenderness elicited over the dorsum of the wrist. Diffuse swelling was present over the left wrist joint (Fig. 1).

Figure 1: (a-c) Clinical image showing swelling (white arrow) at the left wrist joint.
The range of motion at the wrist joint was restricted with flexion 0–55°, extension 0–30°, radial deviation 0–8°, and ulnar deviation 0–10° and was painful. Roentgenography revealed multiple punched-out osteolytic lesions at the distal radius, distal ulna, multiple carpal bones, and 2nd–5th metacarpal base (Fig. 2).
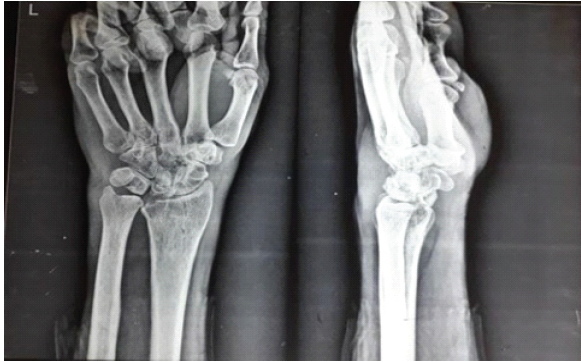
Figure 2: Radiographic anteroposterior and lateral view of the left wrist with hand showing multiple punched out osteolytic lesions at the distal radius, distal ulna, carpals, and base of 2nd–5th metacarpals.
Magnetic resonance imaging (MRI) of the left wrist joint was suggestive of diffuse synovial thickening with multiple large central erosions in the distal radius, distal ulna, multiple carpal bones, and 2nd–5th metacarpal base with associated lytic changes and a small loculated collection measuring 35 mm × 10 mm extending from the joint into the recess along the 2nd inter-metacarpal space (Fig. 3).
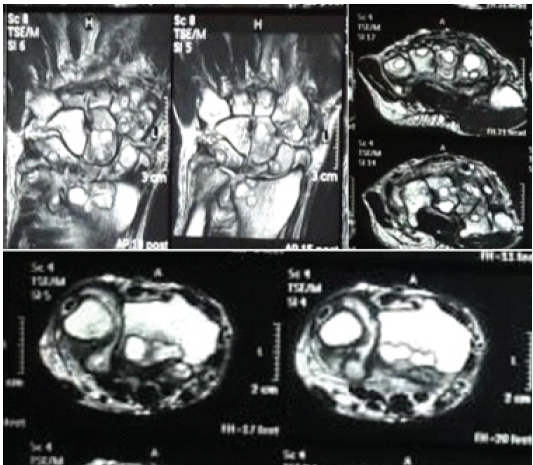
Figure 3: Magnetic resonance imaging (T2 weighted) showing multiple osseous lesions of the distal radius, distal ulna, carpals, and 2nd–5th metacarpal base.
A core needle biopsy was planned for the diagnosis and was taken from the left wrist joint under regional anaesthesia. Bone and synovial tissue samples were sent for histopathological examination, culture, and polymerase chain reaction (PCR) study for tuberculosis. The microscopic appearance of the core biopsy showed fibro-collagenous tissue and bony fragments with viable bony trabeculae consisting of PC infiltrates with occasional binucleated PCs and “Mott cells” (Fig. 4).
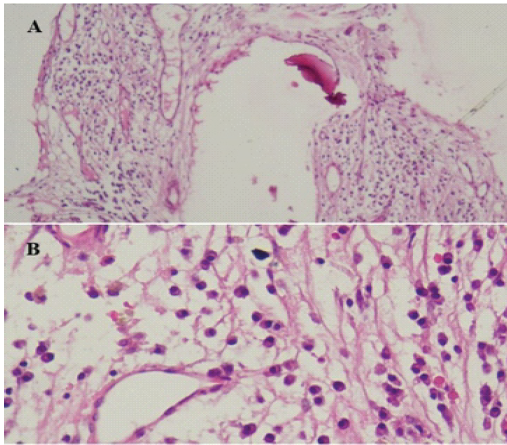
Figure 4: (A and B) Histopathological images on core needle biopsy of distal radius and carpals showing sheets of plasma cells with binucleate forms, Russell bodies in bony trabeculae (×4 and ×40 magnification).
Interestingly, multiple intracytoplasmic crystalline inclusions (CI) were found in this case, which is a rare finding in SBP, and such a finding in histopathology warrants further investigations in the direction of PC dyscrasias, such as MM. MRI of the whole spine and pelvis was done to rule out other intraosseous lesions. There was no evidence of granuloma in the biopsy. PCR confirmed the absence of mycobacteria from the synovial tissue. In view of the above findings, a provisional diagnosis of plasmacytoma was made. A complete clinical, haematological, biochemical, and radiological work-up was advised to exclude MM as shown in Table 1.
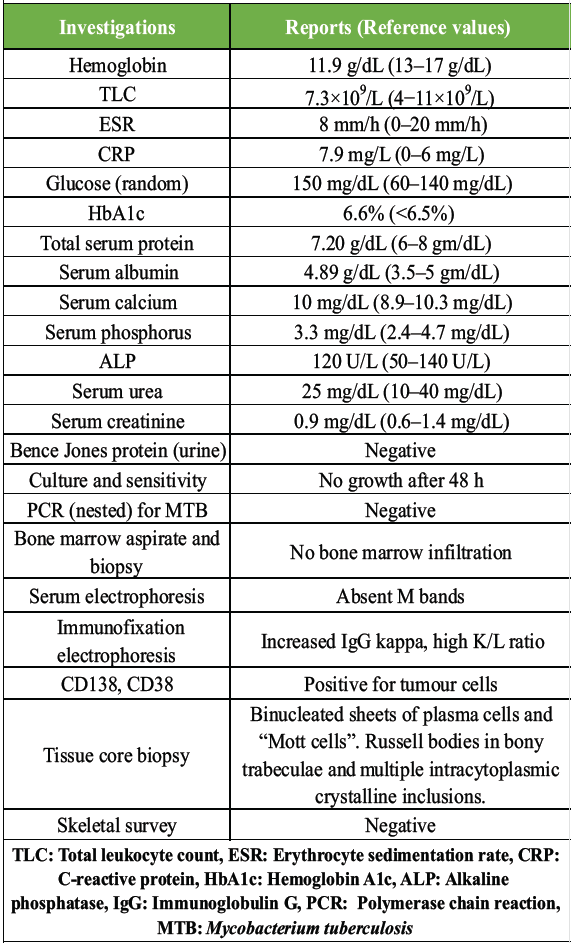
Table 1: Hematological, biochemical, and radiological work-up of the patient
Based on the above findings, a diagnosis of SBP of the left wrist joint, including the distal radius, the ulna, the carpals, and the base of the 2nd to 5th metacarpals, was made. The patient was given RT in a radiation dose of 50 Gy for a total duration of 4 weeks. As recommended by the International Myeloma Working Group (IMWG), post-RT repeat biopsy, serum immunofixation electrophoresis, and serum protein electrophoresis (performed at 3 months, 6 months, and 12 months) were done, which showed a few PCs with resolved serum monoclonal protein and degenerative changes indicating resolution of the disease. The patient was followed up with repeat radiographs at the immediate post-RT session and at 6 months, which showed sclerosis at the site of lesions (Figs. 5 and 6).

Figure 5: (a and b) Radiographs of the left wrist with hand antero-posterior and lateral view post-radiotherapy showing sclerosis of lesions.

Figure 6: (a and b) Radiographs of the left wrist with hand anteroposterior and lateral view at 6-month follow-up showing resolution of the sclerotic lesions.
As per IMWG recommendation [11], repeat computed tomography (CT) and MRI scans of the wrist joint were performed at 12 months post-RT, which showed complete regression of the lytic lesions (Fig. 7). Patient-rated wrist evaluation (PRWE) and pain assessment on the basis of Visual Analogue Scale (VAS) score were assessed before (PRWE = 80, VAS = 7) and after (PRWE = 10, VAS = 1) treatment of 12 months for documenting wrist joint function and quality of daily activities.
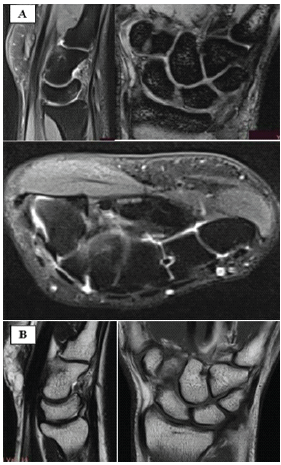
Figure 7: Post-radiotherapy magnetic resonance imaging with (a) T1 weighted sagittal, coronal, and axial views and (b) T2 weighted sagittal and coronal views after 12 months showing complete regression of the lytic lesions.
PC neoplasms can present in different clinical forms. SP is characterised by a single mass of monoclonal PCs with no or minimal bone marrow plasmacytosis [5]. It can present as EMP, that is, soft tissue involvement, or SBP, defined by the presence of a single lytic lesion due to monoclonal PC infiltration. SBP occurs more commonly in men than in women (M:F – 2:1) and presents a decade earlier than MM. SBP is a rare condition that comprises 70% of all SP cases and occurs primarily in red marrow-containing bones, such as the vertebrae, the femur, the pelvis, and the ribs, and very rarely in the appendicular skeleton below the elbow and the knee joint [1,6]. Ozsahin et al. in his cohort of 206 patients found 16 cases (8%) involving the upper extremity and 10 cases (5%) involving the lower extremity [9]. The Mayo Clinic showed the upper extremity lesions in 2% and the lower extremity lesions in 4% of the total cohort of 46 patients [3]. According to the literature, only six cases (out of twelve) of SBP in the appendicular skeleton below the elbow and the knee joint are published to date in the best of our search (Table 2).
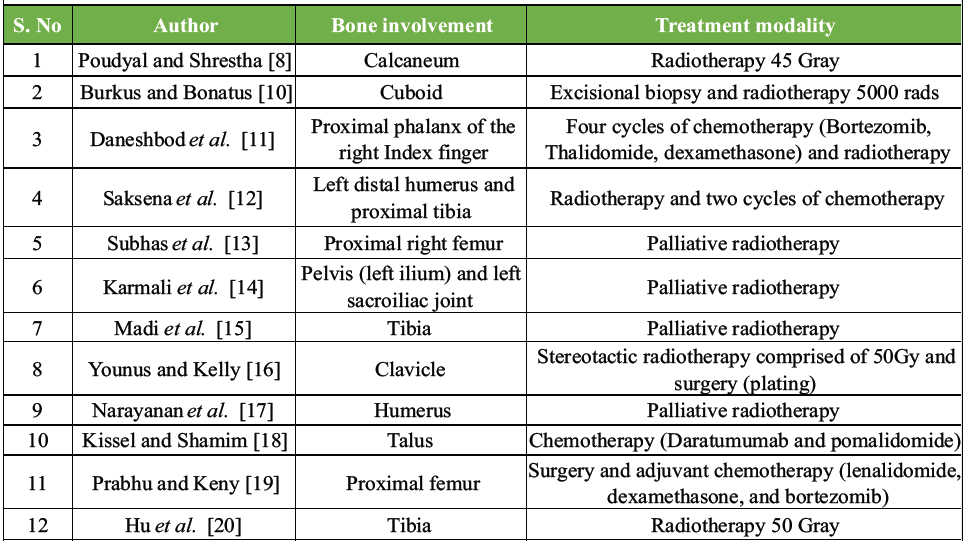
Table 2: Published articles of Solitary bone plasmacytoma in appendicular skeleton: Resource (PubMed and Google Scholar)
According to the IMWG updated criteria for the diagnosis of SBP, a biopsy-proven lesion of bone or soft tissue with evidence of monoclonal PCs <10%, a normal skeletal survey, and a whole-body MRI (or CT), including spine and pelvis, is a prerequisite [6]. IMWG also advocates for the absence of end-organ damage, such as hypercalcemia, renal insufficiency, anaemia, or bony lesions (CRAB), that can be attributed to a lymphoplasmacytic proliferative disorder [5]. As there were no bone marrow infiltrations, we ruled out the differential diagnosis of occult early-stage MM, that is, monoclonal gammopathy of undetermined significance and smouldering MM, which are asymptomatic blood dyscrasias diagnosed incidentally on blood investigations showing <10% and 10–60% bone marrow PCs, respectively [4]. As bone marrow aspiration count may underestimate the degree of bone marrow plasmacytosis in up to 30% of cases, it should be viewed in conjunction with the trephine section/core needle biopsy for immunohistological marker examinations for PC dyscrasias [21]. Another study recommends that SP diagnosis is currently based on a tissue biopsy and histological and immunohistochemical confirmation of the presence of a homogenous infiltrate of the monoclonal PCs, which typically express CD138 and/or CD38 [22]. Monoclonality needs to be proven by kappa/lambda light chain restriction or by a PCR-based approach [22]. Interestingly, a fair number of intracytoplasmic CI bodies (CI) were seen, which were positive for kappa and negative for lambda, and PCs also showed kappa restriction. However, due to the rarity of the disease, CI doesn’t have a significant correlation regarding prognosis [23]. Furthermore, the prognostic value of cytogenetic abnormalities detected by fluorescence in situ hybridisation diminishes over time as the disease undergoes clonal evolution and does not always allow low clonal cell detection for minimal residual disease [24]. Histopathological analysis alone is not sufficient for making a diagnosis; all the above investigations are mandatory to exclude MM. As per recommendations, all suspicious patients should undergo bone marrow aspiration and bone marrow biopsy to evaluate PC morphology and degree of infiltration [22]. Core needle biopsy and/or fine needle aspiration cytology often helps in the early provisional diagnosis, as in the present case. According to the literature, electrophoresis of serum and urine samples reveals monoclonal protein in 24–72% of patients with SBP [1]. As per IMWG criteria, along with a radiological skeletal survey or CT, MRI or positron emission tomography (PET) is required as a mandatory investigation to rule out additional lesions [22]. The National Comprehensive Cancer Network guidelines primarily recommend whole-body MRI for the follow-up of SBP over PET-CT [25]. The MRI appearance of SBP is consistent with that of a focal area of bone marrow replacement, but in this case, MRI findings were suggestive of diffuse synovial thickening with multiple large central erosions in bone, pointing toward an infective aetiology instead of a neoplastic nature, which had not been reported yet in the best of our search. Definitive local RT is the treatment of choice for SBP [22]. Surgical treatment in plasmacytoma is considered when the lesion involves a distinct location, such as the spine, which presents with neurological compromise or anatomical instability. Furthermore, adding chemotherapy did not offer any extra advantage over RT [26]. A study suggests that a total fractionated dosage of 40–50 Gy must be given along with a margin of at least 2 cm should be employed [22]. Serial and frequent measurements of myeloma protein for at least 6 months after treatment are required to confirm disease radiosensitivity [6]. To assess the response of treatment, criteria recommended by IMWG are widely followed, according to which the initial radiological abnormalities on MRI or CT should regress or stabilise during an observation time of at least 12 months to label the patient as having a complete response (CR) [22]. In this case, there was complete resolution of lytic lesions, confirmed by CT and MRI done after 12 months. Liebross et al., in their cohort of 1354 patients, defined the response to therapy as a >75% reduction of serum myeloma protein production, reduction of bone marrow plasmacytosis to <5%, and stable lytic bone lesions with sclerosis and bone remineralisation on post-therapy radiographs [6]. There is a higher risk for progression to MM for SBP patients (65–84% at 10 years) compared to EMP patients (25–35% at 10 years) [22,27,28]. Similarly, IMWG also reported the progression rate as 60% for bone lesions and 20% for soft tissue within 3 years [5]. As per recommended prognostic criteria, our patient has a 9% chance of progression to MM as serum monoclonal protein after radiation therapy gets resolved, as compared to a 71% rate of progression in those with persistent monoclonal proteins [1,6,22]. On CT examination post-RT, there was complete resolution of the lytic lesions over the distal radius and ulna, the carpals, and the base of the 2nd–5th metacarpals.
SBP of the appendicular skeleton, especially distal to the elbow, as seen in this case, is very rare in adults. Interestingly, this case initially appeared to be of inflammatory/infective aetiology based on chronicity of the symptoms and radiological scanning (showing a small loculated collection and multiple erosive and lytic lesions) but was proven to be a neoplastic condition of the wrist joint on the histopathological examination, immunohistochemical tests, and immunoelectrophoresis. It stands much later in the queue of the differentials and warrants an exhaustive armamentarium of investigations. To avoid missing such cases, one should not restrict themselves to the most common diagnosis only and evaluate the patient by keeping other differential diagnoses in the queue.
- Since unusual presentation of SBP of the appendicular skeleton, especially distal to the elbow, is extremely rare, diagnosis may be missed radiographically as it is an infrequent site of involvement (2–4%) and warrants an exhaustive armamentarium of investigations
- Correct diagnosis and prompt treatment are pivotal as it is notorious for progression into more aggressive MM (65–84% at 10 years)
- In this case, multidisciplinatory approach in terms of extensive radiological, biochemical, histopathological, and immunohistochemical investigations to rule out the differential diagnosis was the key to eschew misdiagnosis.
References
- 1. Dimopoulos MA, Moulopoulos LA, Maniatis A, Alexanian R. Solitary plasmacytoma of bone and asymptomatic multiple myeloma. 2000;96. [Google Scholar] [PubMed]
- 2. Kilciksiz S, Karakoyun-Celik O, Agaoglu FY, Haydaroglu A. A review for solitary plasmacytoma of bone and extramedullary plasmacytoma. Sci World J. 2012;2012:1–6. [Google Scholar] [PubMed]
- 3. Frassica DA, Frassica FJ, Schray MF, Sim FH, Kyle RA. Solitary plasmacytoma of bone: Mayo clinic experience. Int J Radiat Oncol Biol Phys. 1989;16:43–8. [Google Scholar] [PubMed]
- 4. The International Myeloma Working Group. Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: a report of the International Myeloma Working Group. Br J Haematol. 2003;121:749–57. [Google Scholar] [PubMed]
- 5. Rajkumar SV, Dimopoulos MA, Palumbo A, Blade J, Merlini G, Mateos M-V, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15:e538–48. [Google Scholar] [PubMed]
- 6. Liebross RH, Ha CS, Cox JD, Weber D, Delasalle K, Alexanian R. Solitary bone plasmacytoma: Outcome and prognostic factors following radiotherapy. Int J Radiat Oncol Biol Phys. 1998;41:1063–7. [Google Scholar] [PubMed]
- 7. Wei A, Juneja S. Bone marrow immunohistology of plasma cell neoplasms. J Clin Pathol; 2003;56:406–11. [Google Scholar] [PubMed]
- 8. Poudyal S, Shrestha S. Solitary plasmacytoma of the calcaneum: A case report. JNMA J Nepal Med Assoc. 2019;57:373–5. [Google Scholar] [PubMed]
- 9. Ozsahin M, Tsang RW, Poortmans P, Belkacémi Y, Bolla M, Dinçbas F O, et al. Outcomes and patterns of failure in solitary plasmacytoma: A multicenter rare cancer network study of 258 patients. Int J Radiat Oncol Biol Phys. 2006;64:210–7. [Google Scholar] [PubMed]
- 10. Burkus JK, Bonatus TJ. Solitary plasmacytoma of the cuboid. Foot Ankle. 1988;8:344–9. [Google Scholar] [PubMed]
- 11. Daneshbod Y, Nowshadi PA, Negahban S, Aledavood A, Ramzi M, Fanaie S, et al. Solitary plasmacytoma of the index finger. J Clin Pathol. 2014;67:828–31. [Google Scholar] [PubMed]
- 12. Saksena A, Mahajan N, Agarwal S, Jain S. Solitary bone plasmacytoma: An interesting case report with unusual clinico-cytological features. J Cytol. 2014;31:158-60. [Google Scholar] [PubMed]
- 13. Subhas N, Bauer TW, Joyce MJ, Sundaram M. The “mini brain” appearance of plasmacytoma in the appendicular skeleton. Skeletal Radiol. 2008;37:771–4. [Google Scholar] [PubMed]
- 14. Karmali S, Barros A, Rosa B, Campos P, Gonçalves R, Da Costa DS, et al. Solitary bone plasmacytoma of the Pelvis: A rare tumor. Rare Tumors. 2016;8:39–41. [Google Scholar] [PubMed]
- 15. Madi S, Pandey V, Sharma A, Monappa V. Case of solitary plasmacytoma of tibia. BMJ Case Rep. 2018 Oct 7;2018:bcr2018227546. [Google Scholar] [PubMed]
- 16. Younus A, Kelly A. Solitary plasmacytoma of the clavicle: A case report and literature review. East Afr Orthop J. 2022;16:49-55. [Google Scholar] [PubMed]
- 17. Narayanan G, Nambiar R, Kumar BS. Solitary Plasmacytoma of the Humerus. IJBS 2017; 9(3):99-100. [Google Scholar] [PubMed]
- 18. Kissel BG, Shamim MS. A rare case of a pathologic fracture of the talus due to a solitary plasmacytoma. Foot Ankle Surg Tech Rep Cases. 2022;2:100147. [Google Scholar] [PubMed]
- 19. Prabhu RM, Keny SA. Rare Case of a Solitary bone plasmacytoma of the proximal femur managed with surgery and adjuvant chemotherapy: A case report. J Orthop Case Rep 2021;11:24-8. [Google Scholar] [PubMed]
- 20. Hu X, Li D, Hu X, Li S, Wang P. Solitary plasmacytoma of the tibia: Literature review and case report. Front Oncol. 2026;16:1503479. [Google Scholar] [PubMed]
- 21. Al-Quran SZ, Yang L, Magill JM, Braylan RC, Douglas-Nikitin VK. Assessment of bone marrow plasma cell infiltrates in multiple myeloma: The added value of CD138 immunohistochemistry. Hum Pathol. 2007;38:1779–87. [Google Scholar] [PubMed]
- 22. Caers J, Paiva B, Zamagni E, Leleu X, Bladé J, Kristinsson SY, et al. Diagnosis, treatment, and response assessment in solitary plasmacytoma: Updated recommendations from a European Expert Panel. J Hematol Oncol. 2018;11:10. [Google Scholar] [PubMed]
- 23. Guo S, Zhang L, Wang YF, Sun BC, Zhang LY, Zhang J, et al. Prognostic factors associated with solitary plasmacytoma. OncoTargets Ther. 2013;6:1659–66. [Google Scholar] [PubMed]
- 24. Atli EI, Gurkan H, Kirkizlar HO, Atli E, Demir S, Yalcintepe S, et al. Pros and cons for fluorescent in situ hybridization, karyotyping and next generation sequencing for diagnosis and follow-up of multiple myeloma. Balkan J Med Genet. Macedonian Academy of Sciences and Arts; 2021;23:59–64. [Google Scholar] [PubMed]
- 25. Hatipoğlu U, Seyhan M, Ulas T, Dal MS, Altuntaş F. Solitary plasmacytomas: Current Status in 2025. Hematol Rep 2025;17:32. [Google Scholar] [PubMed]
- 26. Knobel D, Zouhair A, Tsang RW, Poortmans P, Belkacémi Y, Bolla M, et al. Prognostic factors in solitary plasmacytoma of the bone: A multicenter rare cancer network study. BMC Cancer. 2006;6:118. [Google Scholar] [PubMed]
- 27. De Waal EG, Leene M, Veeger N, Vos HJ, Ong F, Smit WG, et al. Progression of a solitary plasmacytoma to multiple myeloma. A population-based registry of the northern Netherlands. Br J Haematol. 2016;175:661–7. [Google Scholar] [PubMed]
- 28. Tsang RW, Gospodarowicz MK, Pintilie M, Bezjak A, Wells W, Hodgson DC, et al. Solitary plasmacytoma treated with radiotherapy: Impact of tumor size on outcome. Int J Radiat Oncol Biol Phys. 2001;50:113–20. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Solitary Plasmacytoma and its Progression into Multiple Myeloma – A Case Report
March 1, 2026 Solitary Plasmacytoma and its Progression into Multiple Myeloma – A Case Report November 1, 2025 Multiple Myeloma Presenting as Cauda Equina Syndrome: A Rare and Early Spinal Manifestation
November 1, 2025 Multiple Myeloma Presenting as Cauda Equina Syndrome: A Rare and Early Spinal Manifestation December 1, 2024 Kingella kingae Induced Septic Arthritis in the Knee Revealing an Unexpected Diagnosis of Multiple Myeloma, a Case Report
December 1, 2024 Kingella kingae Induced Septic Arthritis in the Knee Revealing an Unexpected Diagnosis of Multiple Myeloma, a Case Report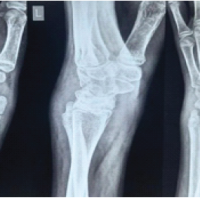 December 1, 2024 Tuberculous Tenosynovitis of the Wrist: A Rare Case Report
December 1, 2024 Tuberculous Tenosynovitis of the Wrist: A Rare Case Report