
Clinical-radiological dissociation can occur after failed Monteggia fixation: a clinically stable fibrous ulnar non-union with chronic lateral radial head dislocation may still allow acceptable function. In selected patients with minimal pain and good validated functional scores who decline revision surgery, structured observation with clear counselling and planned surveillance can be a reasonable, preference-sensitive option.
Dr Sai Surya Dinesh Pydi, Department of Orthopaedics, Post Graduate Institute of Medical Education and Research, Chandigarh, India. E-mail: saisuryadinesh111@gmail.com
Abstract
Introduction: Monteggia fracture-dislocations in adults require restoration of ulnar length and alignment to maintain radiocapitellar stability. Fixation failure with refracture and recurrent radial head dislocation is typically managed surgically.
Case Report: A 42-year-old right-hand-dominant male electrician sustained a fall on level ground and presented with pain and swelling around the left elbow and proximal forearm and an inability to mobilise the elbow. He had undergone open reduction and internal fixation for a Monteggia injury 2 years prior. Radiographs demonstrated breakage of an anatomical olecranon plate with refracture at the proximal ulna and lateral radial head dislocation. After swelling subsided, implant removal was performed. Periosteal reaction around the proximal ulna and distal humerus raised concern for infection; however, no intraoperative purulence was seen, and cultures were negative. Definitive reconstruction was advised, but the patient refused repeat surgery and was lost to follow-up. At 2 years' follow-up, radiographs showed persistent proximal ulnar fibrous non-union and chronic lateral radial head dislocation; clinically, he had minimal pain, preserved functional elbow motion, a Mayo Elbow Performance Score of 90, and a QuickDASH of 4.5/100.
Conclusion: This case highlights clinical-radiological dissociation after failed Monteggia fixation. While surgical reconstruction remains standard, selected patients with minimal pain, clinically stable fibrous non-union, and acceptable function, especially with informed refusal of surgery, may be managed with careful observation and counselling regarding potential late deterioration.
Keywords: Monteggia, implant failure, ulnar non-union, fibrous non-union, chronic radial head dislocation, clinical-radiological mismatch, shared decision-making, observation.
Monteggia fracture-dislocations are defined by an ulnar fracture with associated radial head dislocation and represent a complex injury pattern in adults. Stable restoration of ulnar length and alignment is the cornerstone of treatment and is essential for achieving and maintaining radiocapitellar reduction [1]. Reviews emphasise that even minor errors in ulnar reconstruction can compromise the outcome due to the sensitivity of radiocapitellar congruency and forearm mechanics to ulnar length and alignment [2]. Failure of fixation, non-union, and persistent or recurrent dislocation can lead to pain, stiffness, instability, and degenerative change, and revision reconstruction is commonly advocated when these complications are symptomatic [3]. However, non-union does not always correlate with disability, particularly when the non-union is clinically stable and minimally symptomatic. In the specific context of the proximal ulna/olecranon region, surgical texts note that asymptomatic non-union with adequate elbow function may not require intervention and that stable fibrous non-union can be functionally comparable to solid union in selected scenarios [4]. In addition, classic biomechanical work describes a functional arc of elbow motion for activities of daily living (ADLs) [5], and contemporary analyses suggest that the motion requirements for modern tasks may differ from earlier estimates [6]. We report a case of failed Monteggia fixation with implant breakage and refracture, followed by implant removal only, where the patient returned with radiographic non-union and chronic radial head dislocation but preserved function at 2-year follow-up. Although observation of a clinically stable fibrous non-union is recognised in principle, this report contributes an objective quantification of the clinical-radiological dissociation using validated scores (Mayo Elbow Performance Score [MEPS] 90) and a detailed functional description in a manual labourer, along with a pragmatic decision and surveillance framework for patients who decline revision surgery.
A 42-year-old right-hand-dominant male electrician with no known comorbidities presented 2 days after sustaining a fall on level ground, complaining of severe pain and swelling around the left elbow and proximal forearm with an inability to mobilise the elbow. He reported operative fixation for a Monteggia injury 2 years earlier at another hospital and stated that he had regained normal function without deformity or limitation after the initial surgery; prior radiographs and records were unavailable. Examination revealed a swollen elbow with marked tenderness over the elbow and proximal forearm. A laterally palpable globular prominence consistent with the radial head was noted adjacent to the elbow. Active elbow motion was not possible due to pain. Distal perfusion was intact with palpable brachial, radial, and ulnar pulses. Neurological examination revealed no posterior interosseous nerve palsy, and sensory examination was normal in the radial, median, and ulnar nerve distributions. The limb was immobilised in an above-elbow slab with elevation, analgesia, and serial neurovascular assessment. Radiographs demonstrated breakage of an anatomical olecranon plate with refracture at the proximal ulna and associated lateral dislocation of the radial head (Fig. 1a and b).

Figure 1: (a) anteroposterior and (b) lateral radiographs at presentation showing breakage of the anatomical olecranon plate with proximal ulnar refracture and lateral radial head dislocation.
There was a periosteal reaction around the ulnar fracture region and the distal humerus, raising concern for an infective or inflammatory process; however, there was no fever, no wound concerns, and no clinical features of infection. After swelling subsided over the next 3 days, implant removal was performed. Intraoperatively, there was no purulence, sinus tract, or grossly infected tissue. Tissue/implant cultures were obtained and returned negative. The elbow was immobilised for 3 weeks after implant removal. Following slab removal, definitive reconstruction, revision fixation of the proximal ulna with biological augmentation, and consideration of procedures addressing chronic radiocapitellar incongruity were advised. Despite counselling, the patient declined repeat surgery and was lost to follow-up. He reported continued ability to perform occupational and daily activities since the earlier follow-up, without progression of deformity or instability symptoms. There was no documented interim follow-up between implant removal and this presentation. Two years after implant removal, he returned for follow-up evaluation. Radiographs showed a persistent proximal ulnar non-union consistent with a likely fibrous non-union and persistent radial head dislocation (Fig. 2a and b).
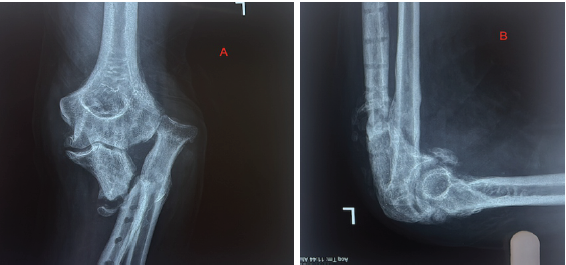
Figure 2: Radiographs obtained at 2-year follow-up after implant removal. (a) anteroposterior and (b) lateral views demonstrating proximal ulnar non-union and persistent radial head dislocation.
Notably, clinical findings did not match the radiographic appearance. He reported no pain at rest (Visual Analogue Scale [VAS] 0) and mild pain during heavier work (VAS 3) while performing ADLs and occupational tasks, including cycling, bathing, holding objects, and electrical work. He could lift approximately 4–5 kg. On examination, there was varus alignment with the radial head palpable laterally. Elbow motion ranged from full extension (0°) to 130° of flexion (Fig. 3a and b).

Figure 3: (a) Full extension and (b) 130° flexion range of motion of the elbow at 2 years.
Forearm rotation revealed 80° of supination with markedly restricted pronation of 10° (Fig. 4a and b). Mediolateral instability was demonstrable on stress testing but was not symptomatic in daily activities. The non-union site was clinically quiescent, without tenderness or appreciable pathological motion. The MEPS was 90 (excellent). QuickDASH at 2 years was 4.5/100.
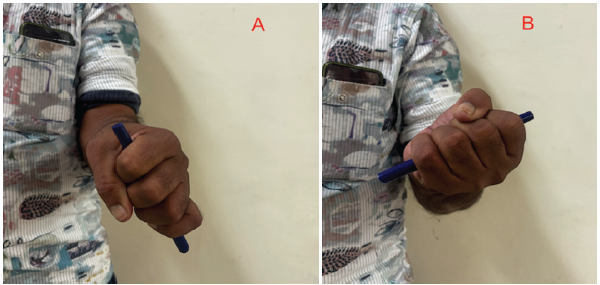
Figure 4: (a) Pronation and (b) supination of the elbow at 2-year follow-up post-implant removal.
This report demonstrates a clinically meaningful clinical-radiological dissociation after failed Monteggia fixation: persistent radiographic non-union and chronic radial head dislocation coexisting with good function, low pain, and an excellent MEPS. The prevailing principle in adult Monteggia injuries is that radiocapitellar stability is restored primarily by reconstituting ulnar anatomy. The AO surgery reference explicitly states that anatomical reduction and stable fixation of the ulna are mandatory to ensure stable relocation of the radial head [1]. Building on this concept, Calderazzi et al., in their review, emphasised that these injuries do not tolerate technical error and that minor mistakes in reconstruction can compromise functional outcomes [2]. These established principles explain why implant failure with refracture and recurrent dislocation is usually approached with revision ulnar fixation, deformity correction, and biological augmentation rather than observation [2,3]. Forearm non-union is particularly concerning because forearm function depends on stability and coordinated rotation. Boussakri et al. described aseptic diaphyseal non-union of the radius and ulna as a major complication, reporting that it accounts for roughly 2–10% of forearm fractures and commonly requires stable internal fixation and bone grafting to restore function [7]. This conventional expectation contrasts with our patient’s outcome and raises the question of why function remained acceptable. A plausible explanation is that the non-union behaved as a clinically stable fibrous non-union, effectively functioning as a “functional union”. Importantly, in the proximal ulna/olecranon region, authoritative surgical texts note that asymptomatic non-union with adequate elbow function may require no intervention and that stable, undisplaced fibrous non-union can provide function comparable to a united fracture in selected circumstances [4]. Although our patient was not completely asymptomatic (VAS 3 with work), he had no tenderness at the fracture site and no clinically detectable motion, suggesting sufficient stability to allow functional use. Preserved elbow motion likely contributed most to his perceived success. Morrey et al.’s classic biomechanical work identified a functional elbow arc of 30° to 130° for most ADL and a functional forearm rotation arc of approximately 50° of pronation and 50° of supination [5]. Our patient exceeded the flexion–extension requirement (0°–130°), which likely enabled many ADLs and work tasks. His pronation was severely restricted (10°), yet he still compensated sufficiently to function as an electrician. Contemporary work by Sardelli et al. suggests that functional elbow range of motion (ROM) requirements may differ for modern tasks, reinforcing the concept that measured limitations do not always translate to unacceptable disability [6]. In addition, although mediolateral instability was demonstrable on stress testing, it was not symptomatic in daily activities, highlighting that examination-elicited laxity does not always equate to functional instability; dynamic neuromuscular control can mitigate symptoms in real-world settings. Chronic radial head dislocation in adults is uncommon, and its management is heterogeneous. Bordet et al. described that in chronic isolated adult radial head dislocation, treatment options may range from reconstructive strategies to therapeutic abstention (observation) in selected patients, depending on symptoms and functional demands [8]. Comprehensive reviews of Monteggia fracture-dislocations emphasise that adult injuries have a higher risk of complications and poorer outcomes compared to paediatric patterns, reinforcing the importance of anatomical ulnar restoration and careful follow-up [9]. Furthermore, large adult series have demonstrated substantial complication rates and functional impairment following Monteggia fractures, supporting reconstruction as the conventional strategy when instability or malalignment persists [10]. This perspective is relevant here: Despite radiographic abnormality, our patient’s pain and function were acceptable, and he refused definitive reconstruction after counselling. From a pragmatic standpoint, delayed reconstruction in chronic settings may entail complex procedures and carries risks such as stiffness, persistent instability, and uncertain preservation of the patient’s existing functional arc. In a patient with low pain and excellent functional score, the benefit of achieving radiographic union becomes preference-sensitive, supporting shared decision-making. When a patient declines revision surgery, observation may be considered reasonable in carefully selected circumstances: when pain is minimal; the non-union is clinically stable without tenderness or pathological motion; objective function is acceptable as assessed by validated scores such as MEPS or QuickDASH; there is no progression of deformity on serial radiographs; and the patient declines operative intervention after informed counselling. Based on the above literature and our case trajectory, we propose a pragmatic observation-versus-reconstruction approach for patients with failed Monteggia fixation who decline revision surgery. Conversely, revision reconstruction should be recommended in the presence of worsening pain, functional decline, symptomatic instability, progressive deformity, neurovascular symptoms, radiographic deterioration or arthrosis, or concern for infection. Patients managed non-operatively should undergo structured follow-up, ideally at 6–12 month intervals, including assessment of symptoms, elbow and forearm ROM, and functional outcome scores. Repeat radiographs may be obtained annually or earlier if symptoms change, and clear clinical or radiographic triggers for re-discussion of surgical management should be documented and communicated to the patient. This report has limitations. We lacked radiographs from the index injury and surgery, preventing confirmation of the initial Monteggia subtype, postoperative alignment, and whether the original fracture had united. Serial imaging between implant removal and the later follow-up visits was unavailable. Follow-up remains limited to 2 years; longer surveillance is still needed to assess late degenerative sequelae. Nevertheless, objective reporting of pain, motion, stress-instability findings, and validated functional scoring supports the central observation that radiographic non-union and chronic dislocation can coexist with acceptable function in selected patients.
Although revision reconstruction is commonly recommended after failed Monteggia fixation with refracture, non-union, and recurrent radial head dislocation, this case demonstrates that a clinically stable fibrous non-union with persistent dislocation can coexist with excellent 2-year function and low pain. In carefully selected patients, particularly those who refuse surgery after counselling, structured observation with objective functional monitoring may be an acceptable alternative, with clear education regarding potential late deterioration and options for delayed reconstruction.
Radiographic non-union and chronic lateral radial head dislocation after failed Monteggia fixation may not always correlate with disability. In selected patients with minimal pain, a clinically stable fibrous non-union, and excellent functional scores who decline revision surgery, structured observation with counselling regarding late deterioration and a planned surveillance strategy can provide acceptable outcomes while preserving current function.
References
- 1. AO Foundation. Radial Head Stabilisation (Monteggia Fracture-Dislocation). AO Surgery Reference. Available from: https://surgeryreference.aofoundation.org [Last accessed on 2025 December 30]. [Google Scholar] [PubMed]
- 2. Calderazzi F, Galavotti C, Nosenzo A, Menozzi M, Ceccarelli F. How to approach Monteggia-like lesions in adults: A review. EFORT Open Rev 2018;3:207-14. [Google Scholar] [PubMed]
- 3. Delpont M, Louahem D, Cottalorda J. Monteggia injuries. Orthop Traumatol Surg Res 2018;104:S113-20. [Google Scholar] [PubMed]
- 4. Morrey BF. Nonunion of the olecranon and proximal ulna. In: Morrey BF, Sanchez-Sotelo J, editors. The Elbow and its Disorders. 4th ed. Philadelphia, PA: Saunders Elsevier; 2009. p. 478-85. [Google Scholar] [PubMed]
- 5. Morrey BF, Askew LJ, Chao EY. A biomechanical study of normal functional elbow motion. J Bone Joint Surg Am 1981;63:872-7. [Google Scholar] [PubMed]
- 6. Sardelli M, Tashjian RZ, MacWilliams BA. Functional elbow range of motion for contemporary tasks. J Bone Joint Surg Am 2011;93:471-7. [Google Scholar] [PubMed]
- 7. Boussakri H, Elibrahimi A, Bachiri M, Elidrissi M, Shimi M, Elmrini A. Nonunion of fractures of the ulna and radius diaphyses: clinical and radiological results of surgical treatment. Malays Orthop J. 2016;10(2):27-34. [Google Scholar] [PubMed]
- 8. Bordet A, Le Mentec O, Arcens M, Trouilloud P, Baulot E, Martz P. Chronic isolated radial head dislocation in adults: Technical note and literature review. Orthop Traumatol Surg Res 2021;107:102829. [Google Scholar] [PubMed]
- 9. Eathiraju S, Mudgal CS, Jupiter JB. Monteggia fracture-dislocations. Hand Clin 2007;23:165-77. [Google Scholar] [PubMed]
- 10. Ring D, Jupiter JB, Simpson NS. Monteggia fractures in adults. J Bone Joint Surg Am 1998;80:1733-44. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Early Mechanical Dissociation of Helical Blade-Barrel Interface in Proximal Femoral Nail: A Case Report
June 1, 2026 Early Mechanical Dissociation of Helical Blade-Barrel Interface in Proximal Femoral Nail: A Case Report May 1, 2026 The Impact of Medial Cortical Reduction on the Outcomes of Fixation in Unstable Intertrochanteric Fractures
May 1, 2026 The Impact of Medial Cortical Reduction on the Outcomes of Fixation in Unstable Intertrochanteric Fractures April 1, 2026 Failure of a Modular Femoral Revision Stem in Hip Arthroplasty: A Rare Complication and Literature Review.
April 1, 2026 Failure of a Modular Femoral Revision Stem in Hip Arthroplasty: A Rare Complication and Literature Review. December 1, 2025 Tibialization of Fibula in an Implant Failure Non-Union Poliotic Limb: A Case Report
December 1, 2025 Tibialization of Fibula in an Implant Failure Non-Union Poliotic Limb: A Case Report