
Our technique demonstrates that the direct posterior approach remains a reliable method of fixation for PCL tibial avulsion fractures and can be adopted more widely in future clinical practice.
Dr. Laura Phieffer, Department of Orthopaedics, The Ohio State University Wexner Medical Center, Columbus, Ohio, USA. E-mail: laura.phieffer@osumc.edu
Abstract
Introduction: Posterior cruciate ligament (PCL) with tibial avulsion injuries commonly occurs following high-energy trauma. While the posteromedial approach is traditionally favoured for fixation, emerging evidence suggests that a direct posterior approach may be a safe and effective alternative for select fracture patterns.
Case Report: We report the case of a 26-year-old polytrauma patient with no significant prior medical or surgical history who presented after a motorcycle accident with a PCL tibial avulsion injury resulting in a posterolateral and tibial intercondylar eminence fracture with a central articular posterior rim involvement. We performed a direct posterior approach, as described by Abbott-Carpenter. Fixation was achieved with FiberWire sutures for the ligamentous avulsion and cannulated screws for the bony fragments. The post-operative recovery was notable for a transient tibial nerve neuropraxia that resolved before discharge, and the patient progressed well in rehabilitation with favourable clinical outcomes at follow-up.
Conclusion: PCL tibial avulsion injuries associated with posterior rim fracture commonly result from hyperflexion mechanisms, classically described as dashboard-type injuries. The fracture morphology and ligamentous involvement determine the optimal surgical approach. This case highlights a less commonly reported fixation strategy using FiberWire sutures and cannulated screws through a direct posterior approach. Our findings contribute to the growing body of evidence that the direct posterior approach to repairing PCL tibial avulsion injury is safe and effective with minimal complications.
Keywords: Posterior cruciate ligament avulsion, posterior rim fractures, fiberwire suture, cannulated screw.
The posterior cruciate ligament (PCL) is a key ligamentous structure that stabilises the knee by attaching to the posterior intercondylar tibia and preventing posterior translation of the tibia. PCL injuries may occur in isolation or in association with tibial avulsion fractures, which result from high-energy mechanisms. Common injury patterns occur in motorcycle accidents and motor vehicle collisions involving a direct blow to the anterior tibia, hyperflexion of the knee, or less commonly, hyperextension of the knee, leading to forceful avulsion of the PCL from its tibial attachment. These injuries require adequate fixation to prevent chronic posterior knee instability, early osteoarthritis, and fracture nonunion [1]. Operative treatment for PCL tibial avulsion injury may be performed through open or arthroscopic techniques. Although no single method has emerged as the gold standard of fixing these injuries, the choice of surgical approach is primarily guided by fracture morphology, degree of displacement, and associated ligamentous injuries. The posteromedial approach, first described by Burks and Schaffer in 1990 [2], remains widely used due to the favourable safety profile, as it involves the interval between the semimembranosus and medial gastrocnemius while avoiding the tibial and popliteal neurovascular structures [3]. Alternative approaches, including posteromedial oblique, limited posterolateral, and modified open posterior approaches, have been described, with each offering varying degrees of exposure and visualisation of the avulsed fragment [4]. Emerging evidence also supports the direct posterior approach, originally described by Abbott and Carpenter [5], which involves the interval between medial and lateral gastrocnemius muscles. Although historically less commonly used due to perceived risk to tibial and popliteal neurovascular structures, recent studies, including a case series from Talebian et al. [6], have demonstrated that this approach can be performed safely with minimal complications while allowing direct visualisation of the fracture pattern. Despite these advantages, there remain limited studies evaluating the outcome and techniques of the direct posterior approach, likely due to the proximity to the popliteal and tibial neurovascular structures. This case report contributes to the existing literature by describing the successful use of a direct posterior approach for fixation of a PCL tibial avulsion injury.
A 26-year-old male with no significant past medical or surgical history presented as a polytrauma patient following a motorcycle collision. At the time of presentation, he was found to have a closed left femoral diaphysis fracture, a left proximal tibial avulsion fracture with PCL injury (Fig. 1), and a closed right radial and ulnar fracture, confirmed by radiographs and computed tomography. In the emergency department, the right wrist was closed reduced, and a femoral traction pin was placed. The following day, the patient underwent open reduction and internal fixation of the left femur with an intramedullary nail and fixation of the right radial and ulnar fractures with a dorsal spanning plate. Subsequent magnetic resonance imaging of the left knee demonstrated a large PCL tibial avulsion involving a posterolateral fragment extending to the tibial intercondylar eminence, with associated central articular posterior rim involvement (Fig. 1). A direct posterior method was selected to better visualise and fix the posterolateral tibial rim fracture, as this fracture pattern may limit screw trajectory and visualisation when addressed through a posteromedial approach. Under general anaesthesia, the patient was positioned prone with the knee flexed 15–20°. A tourniquet was placed on his left proximal thigh. A lazy S-shaped curvilinear skin incision was made along the popliteal crease. The small saphenous and sural nerves were identified (Fig. 2). Dissection continued between the lateral and medial gastrocnemius muscles (Fig. 3), allowing the early identification of the tibial nerve and popliteal vessels, which were tagged with vessel loops and maintained under constant visualisation throughout retraction (Fig. 3). Venous tributaries to the medial gastrocnemius were carefully mobilised and protected by medial retraction (Fig. 4). The popliteus muscle and posterior joint capsule were incised to expose the avulsed fragments (Fig. 5). Under fluoroscopic guidance, the posterolateral fragment was provisionally reduced with a Kirschner wire, followed by definitive fixation with a 4.0-mm cannulated screw. The tibial eminence was subsequently reduced and fixed with an additional 4.0-mm cannulated screw. Repair of the PCL was performed using FiberWire suture and secured to the posterior tibial metaphysis with a 3.5 mm cannulated screw (Fig. 6). Final reduction and screw placement were confirmed under fluoroscopy (Fig. 7). The tourniquet was subsequently deflated. The wound was irrigated, and the medial gastrocnemius was repaired, followed by layered closure of the fascia, subcutaneous tissue, and skin. Postoperatively, the patient was placed in a hinged knee brace, locked in extension during weight-bearing and unlocked at rest to allow range of motion. On post-operative day 2, the patient reported symptoms consistent with tibial nerve neuropraxia, which resolved before discharge. The patient was discharged on post-operative day 3 to inpatient physical rehabilitation, where he demonstrated functional improvement. Two-week post-operative radiographs demonstrated stable fixation without hardware complications. At the 6-month follow-up, the patient reported no concerns, and radiographs showed reduction and intact hardware, and the knee brace was discontinued.
PCL injuries account for approximately 20% of ligamentous injuries [3]. Operative management of PCL tibial avulsion fractures is indicated to reduce fracture non-union and worsening posterior knee displacement, with surgical fixation leading to superior fracture union rates and clinical outcomes compared to non-operative treatment [7]. Although the posteromedial approach described by Burks and Schaffer remains commonly used, emerging literature supports the direct posterior approach as an effective alternative to repair PCL tibial avulsion injuries. The choice between arthroscopic and open fixation remains debated. Although arthroscopic fixation has been associated with improved post-operative knee outcomes, it carries a higher rate of complications such as arthrofibrosis [8]. Conversely, some studies conclude that the clinical outcomes for open and arthroscopic approaches are comparable [7,9], with the open approach offering advantages in terms of reduced complications, shorter operative time, and lower cost [10]. Comparative studies of the direct posterior approach suggest additional benefits; Prakash et al. [11] found that this approach had improved screw placement angle, resulting in better interfragmentary compression at the avulsion site. However, this biomechanical advantage did not lead to statistically significant differences in clinical outcomes, including fracture union time, post-operative range of motion, or functional scores, when compared with the posteromedial approach. In addition, a cadaveric study supports that the direct posterior approach provides greater freedom and flexibility in accessing the PCL tibial insertion [12]. There also remains debate over the technique for fixation, ranging from open reduction with internal fixation using plate-and-screw constructs to cannulated cancellous screws and suture-based techniques [13,14,15]. A prospective study by Keyhani et al. [16] demonstrated reliable outcomes using cannulated cancellous screws through the direct posterior approach, further supporting the safety of this technique. Our technique combines cannulated screw fixation for bony fragments with FiberWire suture repair for the ligamentous avulsion, providing stable fixation and excellent visualisation of complex fracture patterns. Fracture patterns involving the posterolateral tibial rim or combined eminence fragments may limit screw trajectory and visualisation through a posteromedial approach. The primary advantages of this approach include excellent visualisation of the posterolateral fragment and tibial eminence, allowing for adequate reduction and resulting in favourable clinical outcomes. The transient tibial neuropraxia observed in our patient likely resulted from retractor placement and resolved spontaneously. In future cases, this risk can be mitigated by tagging key neurovascular structures and using gentle retraction. Despite increasing evidence supporting its safety, the direct posterior approach to the knee remains underutilised. This is likely due to limited surgeon familiarity with the approach, particularly given the proximity of critical tibial nerve and popliteal vascular structures, as well as limited exposure during residency training. Further comparative studies evaluating the clinical outcomes between direct posterior and posteromedial approaches, along with increased training exposure, may promote broader adoption of this approach. In appropriate cases, the direct posterior approach has the potential to alter current practice patterns and be used as frequently as the posteromedial approach.
This case demonstrates that the combined fixation using FiberWire sutures and cannulated screws through a direct posterior approach provides a safe and reliable fixation for a PCL tibial avulsion fracture with posterior rim involvement. The choice between arthroscopic and open fixation depends on associated injuries, such as the presence of intra-articular injuries, the ease of fracture reduction, and optimal visualisation through the open approach. Although this approach remains underutilised due to surgeons’ comfort, neurovascular risk, and lack of exposure in residency training, growing evidence supports its safety. The direct posterior approach offers a valuable alternative that challenges conventional strategies for addressing posterior knee injuries.
Our technique demonstrates that the direct posterior approach remains a reliable method of fixation for PCL tibial avulsion fractures and can be adopted more widely in future clinical practice.
References
- 1. Katsman A, Strauss EJ, Campbell KA, Alaia MJ. Posterior cruciate ligament avulsion fractures. Curr Rev Musculoskel Med 2018;11:503-9. [Google Scholar] [PubMed]
- 2. Burks RT, Schaffer JJ. A simplified approach to the tibial attachment of the posterior cruciate ligament. Clin Orthop Relat Res 1990;254:216-9. [Google Scholar] [PubMed]
- 3. Abdallah AA, Arafa MS. Treatment of posterior cruciate ligament tibial avulsion by a minimally invasive open posterior approach. Injury 2017;48:1644-9. [Google Scholar] [PubMed]
- 4. Medvecky MJ, Noyes FR. Surgical approaches to the posteromedial and posterolateral aspects of the knee. J Am Acad Orthop Surg 2005;13:121-8. [Google Scholar] [PubMed]
- 5. Abbott LC, Carpenter WF. Surgical approaches to the knee joint. J Bone Joint Surg 1945;27:277. [Google Scholar] [PubMed]
- 6. Talebian P, Aref Daneshi S, Soleimani M. Direct posterior approach to posterior cruciate ligament bony avulsion fractures: A case series introducing a new surgical technique. Ann Med Surg (Lond) 2012;85:598-602. [Google Scholar] [PubMed]
- 7. Gopinatth V, Mameri ES, Casanova FJ, Khan ZA, Jackson GR, McCormick JR, et al. Systematic review and meta-analysis of clinical outcomes after management of posterior cruciate ligament tibial avulsion fractures. Orthop J Sports Med 2023;11:23259671231188383. [Google Scholar] [PubMed]
- 8. Hooper PO 3rd, Silko C, Malcolm TL, Farrow LD. Management of posterior cruciate ligament tibial avulsion injuries: A systematic review. Am J Sports Med 2018;46;734-42. [Google Scholar] [PubMed]
- 9. Song JG, Nha KW, Lee SW. Open posterior approach versus arthroscopic suture fixation for displaced posterior cruciate ligament avulsion fractures: Systematic review. Knee Surg Relat Res 2018;30:275-83. [Google Scholar] [PubMed]
- 10. Sundararajan SR, Joseph JB, Ramakanth R, Jha AK, Rajasekaran S. Arthroscopic reduction and internal fixation (ARIF) versus open reduction internal fixation (ORIF) to elucidate the difference for tibial side PCL avulsion fixation: A randomised controlled trial (RCT). Knee Surg Sports Traumatol Arthrosc 2021;29:1251-7. [Google Scholar] [PubMed]
- 11. Prakash J, Jaiman A, Chopra RK. Posteromedial versus direct posterior approach for posterior cruciate ligament avulsion – a comparative study. J Orthop Trauma Rehabil 2020;27:166-72. [Google Scholar] [PubMed]
- 12. Ambra LF, Franciozi CE, Werneck LG, De Queiroz AA, Yamada RK, Granata GS Jr., et al. Posteromedial versus direct posterior approach for posterior cruciate ligament reinsertion. Orthopaedics 2016;39:e1024-7. [Google Scholar] [PubMed]
- 13. Khalifa AA, Elsherif ME, Elsherif E, Refai O. Posterior cruciate ligament tibial insertion avulsion, management by open reduction and internal fixation using plate and screws through a direct posterior approach. Injury 2021;52:594-601. [Google Scholar] [PubMed]
- 14. Forkel P, Imhoff AB, Achtnich A, Willinger L. All-arthroscopic fixation of tibial posterior cruciate ligament avulsion fractures with a suture-button technique. Oper Orthop Traumatol 2020;32:236-47. [Google Scholar] [PubMed]
- 15. Joshi S, Bhatia C, Gondane A, Rai A, Singh S, Gupta S. Open reduction and internal fixation of isolated posterior cruciate ligament avulsion fractures: Clinical and functional outcome. Knee Surg Relat Res 2017;29:210-6. [Google Scholar] [PubMed]
- 16. Keyhani S, Soleymanha M, Salari A. Treatment of posterior cruciate ligament tibial avulsion: A new modified open direct lateral posterior approach. J Knee Surg 2022;35:862-7. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Medial Epicondyle Fractures Treated with Diverse Fixation Techniques: A Case Series
February 1, 2026 Medial Epicondyle Fractures Treated with Diverse Fixation Techniques: A Case Series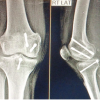 November 1, 2025 Posterior Approach for Single-stage Fixation of Medial Hoffa with Posterior Cruciate Ligament Avulsion: A Rare Case Report
November 1, 2025 Posterior Approach for Single-stage Fixation of Medial Hoffa with Posterior Cruciate Ligament Avulsion: A Rare Case Report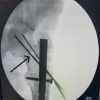 October 1, 2025 Miss-a-nail Technique of Femur Neck Fracture with Femur Interlocking Nail in Situ: A Technical Description
October 1, 2025 Miss-a-nail Technique of Femur Neck Fracture with Femur Interlocking Nail in Situ: A Technical Description January 1, 2025 A Rare Case Report: Managing PCL Avulsion Fracture with a Fracture of the Proximal Tibial Shaft
January 1, 2025 A Rare Case Report: Managing PCL Avulsion Fracture with a Fracture of the Proximal Tibial Shaft