
BPOP (Nora’s lesion) can closely resemble some of the malignant bone tumours; diagnosis necessitates imaging and histology, and wide excision with long-term follow-up lowers the risk of recurrences.
Dr. Sarah Aldubaisi, Department of Orthopedics, King Abdulaziz Airbase Armed Forces Hospital, Dhahran, Saudi Arabia. E-mail: sarah.aldubaisi@gmail.com
Abstract
Introduction: Bizarre parosteal osteochondromatous proliferation (BPOP), also known as Nora’s lesion, is a rare, benign bone tumor predominantly affecting the small bones of the hands and feet. It presents as a diagnostic challenge due to its radiologic and histologic resemblance to malignant bone lesions, such as osteosarcoma and parosteal chondrosarcoma.
Case report: This case series describes the clinical presentation, imaging features, surgical management, and post-operative outcomes of three patients with BPOP involving the small bones of the hand. Radiological imaging, including magnetic resonance imaging and computed tomography scans, played a crucial role in identifying periosteal-based lesions with cortical involvement. Histopathological examination confirmed the diagnosis, distinguishing it from more aggressive conditions. Surgical excision with wide margins was the primary treatment and resulted in favorable outcomes without evidence of recurrence during follow-up. Despite its benign nature, BPOP has a high recurrence rate, emphasizing the importance of long-term monitoring.
Conclusion: This series contributes to the growing literature on BPOP, highlighting the need for accurate diagnosis and appropriate surgical techniques. Future research into the genetic background of BPOP may provide further insights into its pathogenesis and its recurrence, potentially guiding more effective management strategies.
Keywords: Bizarre parosteal osteochondromatous proliferation, Nora’s lesion, benign bone tumor, hand lesions.
Due to its clinical and radiological similarities with both benign and malignant bone lesions, bizarre parosteal osteochondromatous proliferation (BPOP), a rare benign osseous lesion that usually affects the hands and feet, can pose diagnostic difficulties. This lesion is referred to as Nora’s lesion [1], having been first described by Nora in 1983. The primary target of BPOP is the small bones in the extremities, such as the metatarsals in the foot or the phalanges and metacarpals in the hand. BPOP often presents as an exophytic lesion originating from the cortical surface of the bone [1]. The significance of BPOP lies in its predilection to mimic more aggressive conditions, such as osteochondromas, parosteal osteosarcomas, and myositis ossificans, both clinically and radiologically [1]. This often leads to diagnostic dilemmas, especially since its presentation can be confused with that of low-grade malignancies. While histopathology ultimately confirms the diagnosis, the characteristic radiological features—such as the “stuck-on” appearance without continuity between the lesion and the medullary cavity—serve as key characteristics. Nevertheless, misdiagnosis is common, and patients are sometimes initially diagnosed with osteosarcoma or other aggressive tumors based on radiologic findings alone [2]. BPOP typically affects patients in their second to fourth decades of life, though cases have been reported in both older and younger individuals. The lesion has no known gender predilection and presents as a slow-growing mass that is often painless, although some patients report discomfort or pain following repetitive trauma or aggressive activity. The lesion’s growth may lead to functional limitations, particularly if it affects the hand or wrist, where precision and dexterity are critical. Radiologically, BPOP presents as a well-demarcated, sessile, or pedunculated bony growth on the cortical surface. While the lesion’s cortical base is often intact, it may exhibit a thin rim of soft tissue or periosteal reaction, which can be misleading and suggest a more aggressive neoplastic process. Magnetic resonance imaging (MRI) findings are often heterogeneous, with areas of mineralization interspersed with softer, fibrocartilaginous tissue. Despite these characteristic findings, distinguishing BPOP from other surface-based osteochondral lesions can be challenging [3]. Histologically, BPOP exhibits features that can vary, making it difficult to differentiate from more aggressive lesions. The lesion typically consists of disorganized cartilage, bone, and fibrous tissue, with bizarre-looking cells, particularly chondrocytes, embedded within a disorganized matrix. This cellular atypia may mimic features of low-grade osteosarcoma, potentially leading to overdiagnosis [4]. However, the lack of invasion into the surrounding bone and soft tissues helps differentiate BPOP from malignant lesions. Chromosomal studies have also revealed distinct translocations, such as t (1;17) (q32;q21), which are not present in other, more common osteochondral tumors [5]. This unique molecular signature supports the idea that BPOP is a distinct entity, although rare, within the spectrum of benign bone proliferations. Despite its benign nature, BPOP is notorious for its high recurrence rate, with some studies reporting recurrences in up to 50% of cases following surgical excision [6]. Recurrence tends to occur within the first few years after surgery, and it remains unclear whether this is due to incomplete excision, the lesion’s biological behavior, or both. As such, long-term follow-up is essential, although the lesion does not metastasize or undergo malignant transformation. Surgical excision remains the primary treatment; however, the optimal approach, including wide resection versus conservative excision, remains a topic of ongoing debate [1]. Given the rarity of BPOP, the literature is sparse, with most reports consisting of small case series or individual case reports. As a result, standardized treatment protocols have not been established, and much of the management is based on institutional experience and surgeon preference. Continued reporting and investigation into this lesion are crucial for improving diagnostic accuracy and treatment outcomes.
Objectives:
Considering the three cases that are provided as a framework for this study, the goal of this case series is to describe the clinical presentation and imaging features of BPOP in the small bones of the hand. In addition, the study aims to assess the diagnostic challenges associated with BPOP, particularly the difficulty in distinguishing it from more aggressive bone lesions, such as osteosarcoma, through clinical, radiological, and histological evaluation. A key objective is to evaluate the surgical management of BPOP, focusing on the techniques used for lesion excision and the subsequent post-operative recovery process. In doing so, this study will also examine the outcomes, including recurrence rates and functional recovery, while highlighting the importance of long-term follow-up and regular imaging to monitor for potential recurrence. Furthermore, this case series aims to contribute to the existing literature by providing detailed case reports, thereby offering insights to enhance the overall understanding of this rare condition. Finally, based on the findings from these cases, we aim to propose recommendations for improving the management of BPOP. These suggestions will enhance diagnostic accuracy through the use of advanced imaging, histopathological analysis, and potential genetic studies, as well as surgical strategies to reduce recurrence rates and improve patient outcomes.
First case:
A 43-year-old female photographer presented with a 9-month history of progressively worsening pain and swelling in the left middle finger, resulting in restricted finger movement. The patient had no history of trauma but had a significant family history of cancer on her maternal side, including liver cancer, gastric cancer, and breast cancer. The patient was initially evaluated at another hospital and subsequently referred to the orthopedic oncology clinic due to suspicion of a malignant lesion. On physical examination, there was swelling in the proximal phalanx of the left middle finger, with tenderness on both dorsal and volar aspects. In addition, the affected finger demonstrated a markedly restricted range of motion (ROM). Systemic examination did not reveal any lymphadenopathy or other concerning abnormalities.
Radiological findings:
A periosteal lesion affecting the metaphyseal and diaphyseal regions of the proximal phalanx was seen on plain radiographs of the left hand. A computed tomography (CT) scan showed a periosteal-based lesion with a periosteal response generating minor bone erosion dorsally on the middle phalanx. A soft tissue mass across the dorsum of the proximal phalanx was seen on MRI; T1-weighted images showed low signal intensity, whereas T2-weighted images showed heterogeneous high signal intensity. Fine dorsal cortical erosions were seen at the metacarpophalangeal (MCP) joint where the mass expanded. High metabolic activity was indicated by the strong radiotracer uptake at the lesion site, as seen on a whole-body bone scan.
Biopsy and pathology:
An open biopsy was performed, revealing an osteogenic lesion with features suspicious of osteosarcoma initially. The specimen was transferred to an international referral facility for a second opinion, and it was identified as a BPOP lesion.
Surgical intervention:
Due to the significant symptoms and functional impairment, the decision was made to proceed with surgical excision. The tumor was approached dorsally, and an extensor tendon-splitting technique was used to access the lesion. During surgery, the mass was fully encapsulated and covered the proximal phalanx’s medial and lateral sides as well as its dorsum. To achieve adequate hemostasis, the tumor was removed, and the bone surfaces were waxed and shaved to preserve a smooth bone surface.
Post-operative course:
The patient had a smooth surgical recovery and began physical therapy early to restore a complete ROM. Gradually, she was able to fully extend and flex her middle finger while maintaining a strong hold. The patient had no symptoms at the 2-year follow-up period, and radiographs showed no signs of tumor recurrence.
Histopathological findings:
The diagnosis of BPOP was confirmed by histopathology analysis of the resected bone lesion, which revealed distinctive characteristics of Nora’s lesion, such as highly cellular, disordered, and uneven cartilage with an increase in strange-looking fibroblasts and spindle-shaped cells in the intertrabecular gaps.
Second case:
A 40-year-old healthy lady was referred to the orthopedic oncology clinic with a 2-year history of progressive swelling over the right hand’s fifth metacarpal bone. The swelling was hard, non-mobile, and measured approximately 3 × 3 cm. Although the patient did not experience significant pain, she reported an inability to fully extend her little finger, raising concerns about extensor tendon involvement. There was no history of trauma, and her distal neurovascular examination was intact.
Radiological findings:
Radiographic imaging, including MRI and CT scans, revealed a lesion consistent with a BPOP (Fig. 1a, b, c, and d). The lesion involved the right fifth metacarpal shaft, and its progression over time warranted surgical intervention.
Surgical intervention:
The patient underwent excision of the right fifth metacarpal lesion. A 4 cm dorsal skin incision was made over the bony mass. During dissection, the lesion was found to be splitting the extensor digiti minimi (EDM) tendon (Fig. 2a). The tendon was protected, and the lesion was excised using a microsaw, followed by bone resurfacing with a rasp (Fig. 2b). The EDM tendon was then repaired. A volar slab was applied to protect the tendon’s repair and ensure its full healing before initiating the ROM.
Post-operative course:
In the weeks following the surgery, the patient demonstrated a good ROM in the affected hand, including excellent flexion and extension of the little finger. Post-operative radiographs confirmed the complete removal of the lesion without any complications. At subsequent follow-up visits, the patient continued to show no signs of recurrence with excellent functional outcomes.
Third case:
A 31-year-old healthy housekeeper woman who had had swelling on the ulnar side of her right hand, at the level of the fifth metacarpal neck, for 2 years. The patient stated that the swelling had progressively increased in size and that, while she did not feel any pain, she did feel uncomfortable while doing her daily activities using her hands. There was no history of trauma or related constitutional symptoms. Upon examination, there was a hard, non-mobile mass on the dorsal aspect of the right fifth metacarpal neck measuring approximately 3 × 2 cm. There were no overlying skin changes or signs of infection. The patient had a full ROM at the MCP joint, with no tenderness or neurovascular deficits.
Radiological findings:
Plain radiographs revealed a bony mass arising from the dorsal aspect of the fifth metacarpal neck (Fig. 3a). MRI showed features consistent with BPOP (Fig. 3b).
Surgical intervention:
Surgical excision was planned due to the patient’s symptoms and the mass’s growing nature. A dorsal longitudinal skin incision was made directly over the lesion. The subcutaneous tissues were dissected, and the EDM tendon was properly protected. The lesion was excised, and the underlying bone surface was smoothed (Fig. 4a and b).
Post-operative course:
Initially, the patient had some weakness in abduction and adduction of the fingers, likely related to post-operative pain. An immediate post-operative X-ray confirmed the complete removal of the lesion with no associated fractures. At follow-up visits, the patient reported symptomatic improvement, demonstrated full ROM at the MCP joint, and showed no sign of lesion recurrence.
Biopsy and pathology:
Histological examination showed the full spectrum of BPOP lesions in the form of a disorganized mixture of cartilage, benign bone, and bland spindle cells (Fig. 5a). The higher power view showed cartilaginous portions with characteristic basophilic stroma, focal endochondral ossification, and adjacent spindle cell areas with prominent vasculature (Fig. 5b and c). A high magnification view of the cartilaginous component displayed atypical chondrocytes with nuclear irregularities and binucleation. The characteristic basophilic matrix is present (Fig. 5d). Mitotic activity is low, and there are no areas of necrosis.
BPOP, also known as “Nora’s lesion,” is an uncommon but locally aggressive benign bone tumor that predominantly affects the small bones of the hands and feet. This case series reports three patients with BPOP limited to the small bones of the hands, with an emphasis on their clinical presentation, diagnosis complexity, surgical treatment, and functional outcomes. The detailed analysis of these cases contributes to the growing literature on this rare condition and highlights the need for accurate diagnosis and appropriate surgical management to minimize recurrence rates and improve outcomes. One of the primary diagnostic challenges in BPOP is its radiologic and histologic resemblance to more aggressive bone lesions, such as osteosarcoma and periosteal chondrosarcoma. This similarity often leads to misdiagnosis, as reported in previous literature, where BPOP was initially mistaken for malignant tumors because of its aggressive radiologic appearance [7,8]. In our case series, radiographs, MRI, and CT scans revealed periosteal-based lesions with varying degrees of cortical erosion, prompting initial suspicions of osteosarcoma, especially in the first case. This is consistent with the literature, where atypical radiologic features can mimic malignant processes [9]. MRI proved most helpful in determining the extent of the lesion and defining the soft tissue involvement. Soft tissue extension, cortical erosion, and periosteal reaction indicated the need for histopathological confirmation. Histologically, BPOP is distinguished from other lesions by a combination of irregular bone, cartilage, and fibrous tissue with “blue bone” mineralization [10]. Despite these histopathological characteristics, the diagnosis can still be difficult due to overlapping features with other bone lesions. In the first presented case, histological examination confirmed BPOP after an initial misdiagnosis of osteosarcoma, emphasizing the importance of biopsy in validating the diagnosis. A recent case report described an atypical intramedullary presentation of BPOP, which required modifications to the standard treatment approach due to its unique location and associated complications [11]. Although surgical excision remains the mainstay of treatment for BPOP because no effective adjuvant therapy currently exists [7,12], that case deviated from the conventional periosteal-based lesion presentation and required a more nuanced surgical approach. The lesion led to cortical thinning and a pathological fracture, which required bone grafting to restore structural integrity after excision—an uncommon necessity in most BPOP cases. An autograft from the distal radius was used to fill the residual intraosseous cavity, promoting healing and reducing the risk of post-operative instability. This approach differs from standard management, where periosteal-based lesions typically do not require grafting [11]. In addition, a wide local excision was performed with careful attention to adjacent tendon protection, where tendons such as the EDM have been involved in BPOP excisions, as in our third case. The use of wide-awake local anesthesia with no tourniquet technique provided precise surgical control while minimizing patient discomfort and intraoperative bleeding. Early physical therapy leads to excellent functional outcomes, including a full ROM and strength in the affected digit. Given the high recurrence rate associated with BPOP, these cases highlight the importance of tailoring treatment strategies based on lesion characteristics, ensuring complete excision while optimizing bone healing. However, one of the most significant challenges in managing BPOP is its high recurrence rate, reported to range between 20% and 55%, particularly within the first 2 years following excision [7,8]. The recurrence of BPOP is thought to be due to incomplete resection, highlighting the importance of wide surgical margins. In our series, no recurrences were observed during the 2-year follow-up period, possibly owing to the meticulous surgical technique employed. These results align with the findings of Helliwell et al., who also advocated for aggressive resection to prevent recurrence [9]. Radiologic follow-up is essential to monitor for signs of recurrence, as clinical symptoms may not always be apparent in the early stages. In our cases, regular imaging during the follow-up visits showed no evidence of recurrence, and the patients remained asymptomatic. Interestingly, studies have suggested that genetic factors may play a role in the recurrence of BPOP. Kao et al. identified recurrent chromosomal abnormalities in BPOP, including fusions involving COL1A1 and COL1A2, which are associated with the tumor’s proliferative nature [10]. These findings suggest that genetic studies may become an important tool in predicting recurrence risk and guiding the management of patients with BPOP. The cases presented in this series contribute to the growing body of literature on BPOP by providing detailed reports of its clinical presentation, imaging characteristics, and post-operative outcomes. This information is valuable for orthopedic surgeons and radiologists who may encounter this rare condition, as accurate diagnosis and management are essential to prevent recurrence and ensure optimal functional results. Moreover, this series supports the need for continued research into the pathogenesis of BPOP, particularly in understanding its genetic underpinnings. The identification of specific genetic markers, such as COL1A1/2 mutations, may pave the way for more targeted therapies and improve diagnostic accuracy [10]. Based on the findings of this case series and the reviewed literature, several recommendations for the management of BPOP can be proposed. First, accurate diagnosis is crucial and should involve a combination of imaging, biopsy, and histopathological examination to distinguish BPOP from more aggressive bone lesions. Second, wide local excision is essential to minimize the risk of recurrence. In cases where the lesion involves tendons or other critical structures, careful surgical planning is necessary to preserve function. Finally, long-term follow-up with regular imaging is recommended to monitor for recurrence, particularly in the first 2 years postoperatively. Future research should focus on the genetic aspects of BPOP, as this may provide insights into its pathogenesis and tendency for recurrence. Studies exploring advanced imaging techniques, such as functional MRI or positron emission tomography scans, could also improve diagnostic accuracy and help distinguish BPOP from other bone lesions earlier in the disease process.
BPOP is a rare, benign, but locally aggressive tumor that poses significant diagnostic and management challenges due to its resemblance to malignant bone lesions. The cases presented in this series highlight the importance of accurate diagnosis through a combination of imaging and histopathological examination. Surgical excision with wide margins remains the treatment of choice, while early initiation of physical therapy is crucial for optimal functional recovery. Long-term follow-up with regular imaging is essential to detect recurrences, which can occur in up to half of the cases. Genetic studies may offer future insights into the pathogenesis of BPOP and provide more targeted approaches to treatment. This case series contributes to the growing body of literature on BPOP and underscores the need for continued research into its genetic basis and recurrence patterns.
Orthopedic oncologists should consider BPOP (Nora’s lesion) for periosteal hand masses that resemble surface osteosarcoma/chondrosarcoma, therefore obtaining CT/MRI and confirming with histopathology before definitive resection is a must. Surgical excision including the involved periosteum is the mainstay treatment, aiming for wide margins when feasible to lower recurrence. Due to high recurrence rates, long‑term post-operative follow-up should be scheduled, as well as informing patients preoperatively about the possibility of re-excision.
Abramovici L, Steiner GC. Bizarre parosteal osteochondromatous proliferation (Nora’s lesion): A retrospective study of 12 cases, 2 arising in long bones. Hum Pathol 2002;33:1205-10.
Endo M, Hasegawa T, Tashiro T, Yamaguchi U, Morimoto Y, Nakatani F, et al. Bizarre parosteal osteochondromatous proliferation with a t (1; 17) translocation. Virchows Arch 2005;447:99-102.
Rybak LD, Abramovici L, Kenan S, Posner MA, Bonar F, Steiner GC. Cortico-medullary continuity in bizarre parosteal osteochondromatous proliferation mimicking osteochondroma on imaging. Skeletal Radiol 2007;36:829-34.
De Smet L, Lambert I, Sciot R. Bizarre parosteal osteochondromatous proliferation of the hand: Report of two cases. Chir Main 2001;20:247-50.
Nilsson M, Domanski HA, Mertens F, Mandahl N. Molecular cytogenetic characterization of recurrent translocation breakpoints in bizarre parosteal osteochondromatous proliferation (Nora’s lesion). Hum Pathol 2004;35:1063-9.
Michelsen H, Abramovici L, Steiner G, Posner MA. Bizarre parosteal osteochondromatous proliferation (Nora’s lesion) in the hand. J Hand Surg 2004;29:520-5.
Samargandi R. Unusual site of a bizarre parosteal osteochondromatous proliferation (Nora’s Lesion) involving the scapula: First case report and review of the literature. Cureus 2023;15:e38980.
Bajwa SN, Reddy R, Wagh YS, Agarwal M, Katariya A. Bizarre parosteal osteochondromatous proliferation-a case series of typical and atypical presentations. J Orthop Case Rep 2019;10:45-50.
Helliwell TR, O’connor MA, Ritchie DA, Feldberg L, Stilwell JH, Jane MJ. Bizarre parosteal osteochondromatous proliferation with cortical invasion. Skeletal Radiol 2001;30:282-5.
Kao YC, Yoshida A, Hsieh TH, Nord KH, Saba KH, Ichikawa H, et al. Identification of COL1A1/2 mutations and fusions with noncoding RNA genes in bizarre parosteal osteochondromatous proliferation (Nora lesion). Mod Pathol 2023;36:100011.
Zhang F, Wang Y, Wang Y, Wang X, Zhang D, Zhao X, et al. Disruption of Jmjd3/p16Ink4aSignaling Pathway Causes Bizarre Parosteal Osteochondromatous Proliferation (BPOP)-like Lesion in Mice. J Bone Miner Res 2021;36:1931-41.
Edoardo I, Elisa F, Damiano RA, Silvia F, Rodolfo C, Lorenzo A. Bizarre parosteal osteochondromatous proliferation (Nora lesion): A narrative review. Acta Med Litu 2022;29:176-93.[/referenecs_numbered]



Related Articles in Journal of Orthopaedic Case Reports
 February 10, 2024 Bizarre Parosteal Osteochondromatous Proliferation (Nora’s Lesion) Of the Second Proximal Phalanx Encasing the Flexor Tendon of the Foot: A Case Report
February 10, 2024 Bizarre Parosteal Osteochondromatous Proliferation (Nora’s Lesion) Of the Second Proximal Phalanx Encasing the Flexor Tendon of the Foot: A Case Report July 1, 2026 Post-Traumatic Turret Exostosis of the Proximal Phalanx of the Middle Finger: A Rare Case Report and Review of Literature
July 1, 2026 Post-Traumatic Turret Exostosis of the Proximal Phalanx of the Middle Finger: A Rare Case Report and Review of Literature June 1, 2026 Sequential Development and Staged Management of Distal Femoral Osteochondroma with Progressive Bilateral Genu Valgum: A Case Report
June 1, 2026 Sequential Development and Staged Management of Distal Femoral Osteochondroma with Progressive Bilateral Genu Valgum: A Case Report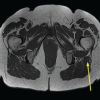 April 1, 2026 Incidental Intramedullary Lipoma of the Proximal Femur Detected Following Trauma: A Case Report
April 1, 2026 Incidental Intramedullary Lipoma of the Proximal Femur Detected Following Trauma: A Case Report