
Hybrid fixation strategies incorporating cervical facet fixation may provide a viable option for revision of proximal junctional failure by optimising fixation, facilitating sagittal alignment, and maximising surface area for arthrodesis in degenerative spines.
Dr. Micah W Smith, Department of Spine Surgery, SpineONE/Orthopaedics Northeast, Fort Wayne, IN, USA. E-mail: wabashspine@gmail.com
Abstract
Introduction: Proximal junctional kyphosis (PJK) and proximal junctional failure (PJF) are well-recognised complications following long thoracolumbar fusion constructs and frequently require complex revision surgery. Achieving stable fixation and solid arthrodesis at proximal levels is particularly challenging in the setting of advanced degeneration and altered anatomy. This case review describes a hybrid fixation strategy incorporating cervical facet fixation to address these challenges.
Case Report: A 76-year-old female presented 21 months after T4–pelvis fusion with progressive PJF, resulting in upper thoracic kyphotic deformity, focal spinal stenosis, and progressive myelopathic symptoms. Imaging demonstrated a fracture at T4, grade 2 T3–4 anterolisthesis, and significant kyphosis with compromise of the spinal canal. The patient underwent revision surgery consisting of C2–T4 posterior fusion with decompression and posterior column osteotomies. A hybrid construct was utilised, including cervical lateral mass fixation, thoracic pedicle fixation, and intervening zero-profile cervical facet fixation. Cervical facet fixation was employed to provide supplemental stabilisation while preserving posterior fusion surface area and accommodating degenerative anatomy without extensive osteophyte resection.
Conclusion: At 2-year follow-up, the patient demonstrated maintained sagittal alignment and radiographic evidence of solid arthrodesis without hardware failure or progression of deformity.
Keywords: Proximal junctional failure, proximal junctional kyphosis, revision spine surgery, cervical facet fixation, long-segment spinal fusion, sagittal alignment.
Proximal junctional kyphosis (PJK) and proximal junctional failure (PJF) are common complications following long thoracolumbar fusion constructs [1,2,3]. Depending on the severity and rigidity of the deformity requiring correction, treatment strategies may include proximal extension of the fusion, posterior column osteotomies such as Ponte osteotomy, or, in more severe cases, three-column osteotomies including pedicle subtraction osteotomy or vertebral column resection [4,5]. As the proximal segments of the spine degenerate, they often become increasingly stiff and osteophytic, creating fixation challenges for treating surgeons. These challenges include determining appropriate implant length and achieving uniform implant head heights to facilitate rod seating while minimizing the risk of pullout or loss of fixation [6,7]. In many patients, the size of traditional lateral mass implant heads may occupy a substantial portion of the lateral mass and overlie the facet joint, limiting available posterior surface area for bone graft placement and potentially compromising arthrodesis [8,9]. Traditional lateral mass fixation introduces implant head prominence and rod interface mechanics that increase construct profile and necessitate substantial posterior muscle dissection. In revision surgery, where prior scarring and altered anatomy already compromise tissue planes, such implant bulk may contribute to paraspinal irritation and an amplified inflammatory response [6,8]. Facet-based systems utilizing a zero-profile, intra-articular design provide stabilization without lateral mass occupation or high-profile rod interfaces at each level [8,9]. By reducing posterior implant footprint and soft-tissue disruption, this strategy supports preservation of paraspinal musculature and maintains the biological substrate necessary for robust posterior arthrodesis. Furthermore, attempts to address implant height mismatch through aggressive osteophyte resection may weaken cortical bone and further jeopardize fixation in an already compromised proximal segment [6,8]. These technical limitations are particularly relevant in revision surgery for PJF, where both biomechanical stability and preservation of the biological environment for fusion are critical. This case report presents a surgical solution utilizing a hybrid fixation construct consisting of cervical lateral mass fixation, thoracic pedicle fixation, and intervening cervical facet fixation to facilitate stable alignment and maximize posterior surface area for achieving solid arthrodesis in the setting of PJF [1,8,9].
A 76-year-old female presented 21 months following a prior T4–pelvis posterior spinal fusion (Fig. 1) with development of PJF characterized by progressive fracture of the T4 vertebral body. The patient initially experienced pain and progressive deformity, followed by worsening deformity of the upper thoracic region and the onset of progressive myelopathic symptoms. On neurologic examination, she demonstrated residual decreased sensation in the left lower extremity, which was chronic and unchanged from her pre-operative baseline before the index surgery. Radiographic evaluation revealed a grade 2 anterolisthesis at T3–4 with 43 degrees of kyphosis across T3–4 (Fig. 2), along with erosion of the T4 pedicle screws into the T3–4 disc space (Fig. 3). The resulting kyphotic deformity produced focal spinal canal stenosis at this level (Fig. 4a and b). Given the progressive deformity, radiographic instability, and neurologic symptoms, the patient was indicated for revision surgery consisting of C2–T4 posterior fusion with T2–4 decompression and T1–4 posterior column (Ponte) osteotomies. The patient had a prior history of PJF at T12 following an earlier spinal procedure; therefore, given the magnitude of correction required, C2 was selected as the upper instrumented vertebra. Intraoperatively, navigation was utilized for the placement of pedicle fixation at T1 through T3. Freehand techniques were employed for placement of cervical fixation at C2, C4, and C5. Intervening cervical facet fixation was placed across the C2–7 facet joints (Fig. 5a and b). Cervical facet fixation with a zero-profile posterior cervical facet fixation system (SurGenTec, ION-C™) provided supplemental stabilization while avoiding occupation of the lateral mass surface area, typically required by traditional lateral mass fixation, thereby preserving posterior surface area for arthrodesis. Facet-based fixation was placed under direct visualization, allowing rapid and reproducible deployment without the need for extensive lateral mass preparation, rod contouring adjustments, or set screw engagement at each level. Compared with traditional lateral mass screw placement, which requires trajectory preparation, screw insertion, rod alignment, and cap screw application, the facet implant can be deployed in a fraction of the operative time while preserving posterior soft-tissue integrity [8,9]. In revision constructs where operative duration and tissue handling are critical variables, minimizing implant complexity may offer additional procedural efficiency [6]. In the setting of advanced degenerative changes with extensive osteophyte formation, variability in implant head heights can complicate rod seating and reduction. Rather than performing aggressive osteophyte resection, which may remove cortical bone and weaken fixation in an already tenuous environment, cervical facet fixation was utilized to accommodate alignment while preserving bone integrity. The rod was contoured appropriately, and with controlled cervical alignment through fixation at C2, C4, and C5, physiologic sagittal alignment was achieved.
As spine surgery continues to increase in prevalence, complications related to adjacent segment pathology are expected to rise. This is particularly critical following long posterior fusion constructs, where PJK/PJF remain common and clinically consequential problems despite ongoing efforts aimed at prevention and risk mitigation [1,2,10]. Revision surgery in this setting presents a unique combination of biomechanical and biological challenges, particularly at the cervicothoracic junction. This case presentation describes a technique utilising posterior cervical facet-based fixation to bridge multiple levels between cervical lateral mass fixation and thoracic pedicle fixation. This strategy facilitated controlled and gentle contouring of the cervical spine without increasing the risk of implant pullout in regions where fixation purchase is often suboptimal [8,9]. Such considerations are especially relevant in revision settings, where bone quality is frequently compromised, and excessive reduction forces may predispose constructs to early failure. In patients requiring revision for PJK/PJF, the cervical spine is often significantly degenerative. Large osteophytes commonly overlie the lateral masses and facet joints, altering posterior anatomy and complicating traditional fixation strategies. The placement of lateral mass fixation without removal of these osteophytes frequently results in variable implant head heights, making rod seating and reduction difficult without applying excessive force, which may increase the risk of fixation failure [8,9]. Conversely, removal of osteophytes to normalise implant alignment may weaken cortical bone and further compromise fixation strength in an already tenuous environment [6]. Traditional lateral mass fixation is inherently high profile, with posterior screw heads and rod interfaces occupying the lateral mass and contributing to implant prominence [8,9]. In contrast, the ION-C™ system functions as a zero-profile intra-articular implant positioned within the facet joint itself, thereby avoiding posterior implant bulk while preserving lateral mass surface area for graft placement [8]. Beyond profile considerations, facet-based fixation engages the joint directly, allowing fusion to occur both within the facet and across the prepared posterior elements. This intra-articular and extra-articular fusion environment may enhance biologic integration while maintaining segmental stability [8,9]. A frequent concern when reducing lateral mass screw density in long-segment cervicothoracic constructs is whether sufficient mechanical strength exists to resist forward cantilever forces during the fusion phase [1,6,7]. In this case, sagittal alignment was maintained without lateral mass screws at every intervening level, suggesting that intra-articular stabilisation provided a meaningful biomechanical contribution during fusion maturation. The durable 2-year radiographic outcome supports the premise that strategic facet-based fixation can supplement construct strength without reliance on maximal screw density [8,9]. These competing technical considerations present a familiar dilemma for the treating surgeon: achieving adequate alignment and stability while preserving both fixation strength and the biological substrate required for fusion, factors that directly influence revision decision-making in cases of PJF [6,5]. Facet-based posterior fixation offers a means of supplementing stability without occupying the lateral mass or requiring aggressive bone removal, thereby preserving the posterior fusion surface area critical for arthrodesis. An additional advantage of this technique is that it is performed in an open surgical setting, allowing direct visualisation of posterior cervical anatomy. This facilitates efficient and reproducible placement of facet-based fixation while avoiding consumption of the lateral mass with traditional implants. By preserving posterior elements and lateral mass surface area, this approach maximises the available bed for bone grafting, an important consideration in revision surgery, where failure to achieve fusion is common [8,9]. At 2-year follow-up, the patient demonstrated preservation of sagittal alignment and radiographic evidence of solid arthrodesis. This outcome is particularly noteworthy given the patient’s advanced age, prior PJFs, long-segment fusion, and markedly degenerative cervical anatomy, factors that historically place patients at substantial risk for nonunion and construct failure following revision surgery [1,6,7]. In a clinical setting where failure to fuse would be expected to be common, the achievement of solid arthrodesis highlights the importance of construct strategies that preserve posterior fusion surface area while enabling stable, controlled fixation. In this case, these principles were realised through the use of the ION-C™ posterior cervical facet fixation system, which provided neutral-position facet fixation without distraction, resisted implant migration, and integrated seamlessly into a hybrid construct spanning the cervicothoracic junction. By addressing both the mechanical demands of alignment correction and the biological requirements for fusion, this approach may represent a valuable adjunct in carefully selected patients undergoing revision surgery for PJF.
Key biomechanical highlights:
Neutral-position facet stabilisation:
Posterior facet-based fixation enables segmental stabilisation while maintaining the facet joint in a neutral, non-distracted position. By limiting joint expansion and avoiding distraction-dependent mechanics, this approach reduces stress transfer to adjacent fixation points and mitigates pullout risk during sagittal alignment correction, particularly in degenerative or revision bone where fixation margins are narrow [1,6,8].
Modulation of insertional and reduction forces:
Fixation strategies that allow gradual, controlled placement minimise peak insertional forces and stress concentrations at the bone–implant interface. Engagement mechanisms that resist migration further enhance construct stability under physiologic loading, an important consideration in long-segment revision constructs where cumulative stresses are amplified [7,8,9].
Posterior column load sharing:
Stabilisation achieved through the posterior column alters the force profile of the construct by reducing reliance on cantilever forces during rod seating and contouring. This promotes more uniform load distribution across fixation points and decreases the risk of mechanical failure in compromised bone [6,8].
Preservation and preparation of the posterior fusion interface:
Avoidance of lateral mass occupation preserves posterior fusion surface area while permitting targeted preparation of the facet joints and adjacent posterior elements. This maximises graft–host contact and supports a mechanically stable environment favourable for arthrodesis in revision settings where fusion beds are often limited [6,8].
Mechanically supported osseointegration:
Stable fixation within physiologic micromotion thresholds supports bone formation at the graft–implant interface. Implant architectures that permit graft incorporation and load transfer across the fusion interface facilitate osseointegration and contribute to long-term construct durability [8,9].
Clinical correlation in this case:
The maintained sagittal alignment and solid arthrodesis observed at 2-year follow-up are consistent with these biomechanical principles. In this construct, the ION-C™ posterior cervical facet fixation system served as an implementation of these concepts, providing neutral-position facet stabilisation, resistance to implant migration, controlled placement, and compatibility with graft integration within a hybrid cervicothoracic fixation strategy.
Zero-profile stabilisation and reduced soft tissue burden:
Intra-articular facet fixation avoids posterior implant prominence associated with lateral mass screw heads and rod interfaces. A reduced construct profile may decrease paraspinal irritation and inflammatory burden, particularly in revision surgery where scar formation is already significant [6,8].
Reduced fixation density without loss of alignment control:
Strategic facet-based fixation may reduce reliance on high-density lateral mass screw placement while maintaining sagittal balance under physiologic loading. In long-segment revision constructs where pullout and proximal failure are concerns [1,7], the preservation of alignment in this case supports the mechanical contribution of intra-articular stabilisation [8,9].
PJF following long posterior fusion constructs presents substantial biomechanical and biological challenges, particularly in the setting of advanced degeneration and prior revision surgery. This case illustrates that a hybrid fixation strategy incorporating posterior cervical facet-based stabilisation can facilitate controlled sagittal alignment while preserving posterior fusion surface area—an important determinant of fusion mass development and long-term construct durability in high-risk revision environments. In the context of extensive degenerative anatomy, prior junctional failure, and elevated risk for nonunion, incorporation of intra-articular facet stabilisation provided supplemental posterior support without requiring lateral mass fixation at every intervening level. In a revision construct subjected to significant anterior cantilever forces and compromised bone quality [1,6,7], maintenance of sagittal alignment at 2-year follow-up supports the potential biomechanical contribution of facet-based fixation within a hybrid cervicothoracic strategy. Access to posterior facet-based fixation techniques may expand surgical options for addressing complex PJF while preserving the posterior fusion substrate critical for arthrodesis [8,9]. Well-designed prospective comparative studies are warranted to further define the biomechanical and clinical durability of intra-articular facet stabilisation relative to conventional posterior fixation constructs in complex and revision cervical surgery.
Strategic incorporation of zero-profile cervical facet fixation within hybrid cervicothoracic constructs may preserve posterior fusion surface area while providing biomechanical stability in revision proximal junctional failure.
References
- 1. Hyun SJ, Lee BH, Park JH, Kim KJ, Jahng TA, Kim HJ. Proximal junctional kyphosis and proximal junctional failure following adult spinal deformity surgery. Korean J Spine 2017;14:126-32. [Google Scholar] [PubMed]
- 2. Lau D, Clark AJ, Scheer JK, Daubs MD, Coe JD, Paonessa KJ, et al. Proximal junctional kyphosis and failure after spinal deformity surgery: Systematic review of incidence, risk factors, and outcomes. Spine (Phila., Pa. 1976) 2014;39:2093-102. [Google Scholar] [PubMed]
- 3. Glattes RC, Bridwell KH, Lenke LG, Kim YJ, Rinella A, Edwards C 2nd. Proximal junctional kyphosis in adult spinal deformity following long instrumented posterior spinal fusion: Incidence, outcomes, and risk factor analysis. Spine (Phila., Pa. 1976) 2005;30:1643-9. [Google Scholar] [PubMed]
- 4. Hart RA, McCarthy I, Ames CP, Shaffrey CI, Hamilton DK, Hostin R. Proximal junctional kyphosis and proximal junctional failure. Neurosurg Clin N Am 2013;24:213-8. [Google Scholar] [PubMed]
- 5. Hart R, McCarthy I, O’Brien M, Bess S, Line B, Adjei OB, et al. Identification of decision criteria for revision surgery among patients with proximal junctional failure after surgical treatment of spinal deformity. Spine (Phila., Pa. 1976) 2013;38:E1223-7. [Google Scholar] [PubMed]
- 6. Echt M, Ranson W, Steinberger J, Yassari R, Cho SK. A systematic review of treatment strategies for the prevention of junctional complications after long-segment fusions in the osteoporotic spine. Global Spine J 2021;11:792-801. [Google Scholar] [PubMed]
- 7. Yagi M, Yamanouchi K, Fujita N, Funao H, Ebata S. Proximal junctional failure in adult spinal deformity surgery: An in-depth review. Neurospine 2023;20:876-89. [Google Scholar] [PubMed]
- 8. Laratta JL, Gupta K, Smith WD. Tissue-sparing posterior cervical fusion with inter-facet cages: A systematic review of the literature. Global Spine J 2020;10:230-6. [Google Scholar] [PubMed]
- 9. Kasliwal MK, Manning BT, Russo V. Posterior cervical fusion using cervical interspace spacers: clinical and radiographic outcomes. J Craniovertebr Junction Spine 2016;7:48-54. [Google Scholar] [PubMed]
- 10. Lanodiyu ZA, Sakti YM, Rahyussalim AJ, Nagata K. Key considerations for the prevention of proximal junctional kyphosis following adult spinal deformity surgery: A literature review. Spine Surg Relat Res 2025;10:19-28. [Google Scholar] [PubMed]

Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Cauda Equina Syndrome Following Posterior Interbody Cage Migration after TLIF: A Rare Case Report
June 1, 2026 Cauda Equina Syndrome Following Posterior Interbody Cage Migration after TLIF: A Rare Case Report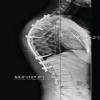 January 1, 2026 Proximal Junctional Kyphosis Following Spinal Thoracic Deformity Correction in a Patient with Kabuki Syndrome: A Case Report
January 1, 2026 Proximal Junctional Kyphosis Following Spinal Thoracic Deformity Correction in a Patient with Kabuki Syndrome: A Case Report February 10, 2021 Unexpected Complications after Corrective Spinal Fusion Surgery for Adult Spinal Deformity with Severe Hip Contracture
February 10, 2021 Unexpected Complications after Corrective Spinal Fusion Surgery for Adult Spinal Deformity with Severe Hip Contracture April 14, 2013 A Case of Simultaneous Bilateral Anterior Shoulder Dislocation
April 14, 2013 A Case of Simultaneous Bilateral Anterior Shoulder Dislocation