
Painful proximal humerus enchondromas in older adults should always be carefully evaluated to exclude low-grade chondrosarcoma. Histopathological confirmation remains essential for definitive diagnosis.
Dr. U Thyagarajan, Department of Orthopaedic Surgery, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India. E-mail: thyaga_77@hotmail.com
Abstract
Introduction: Enchondromas are benign cartilaginous tumours commonly affecting the small bones of the hand; however, proximal humeral involvement presenting with persistent pain in older adults is uncommon and may mimic low-grade chondrosarcoma.
Case Report: A 53-year-old female presented with right shoulder pain and proximal humeral swelling. Radiographs, magnetic resonance imaging, and computed tomography imaging demonstrated a lobulated intramedullary cartilaginous lesion with cortical thinning and endosteal scalloping. The patient underwent curettage of the lesion, biopsy, and bone grafting using bone substitutes. Histopathological examination confirmed an enchondroma. Post-operative follow-up demonstrated satisfactory graft incorporation and symptomatic improvement.
Conclusion: This case highlights the importance of prompt radiological investigations, and histopathological examination is essential for accurate diagnosis and management with curettage and bone substitution, which showed good incorporation and outcome.
Keywords: Enchondroma, low-grade chondrosarcoma, curettage, graft incorporation.
Enchondromas are benign intramedullary cartilaginous neoplasms arising from residual growth plate cartilage [1]. Although commonly found in the small bones of the hands and feet, long bone involvement, such as the proximal humerus, is less common [1,2]. Symptomatic lesions in older adults may mimic low-grade chondrosarcoma clinically and radiologically, creating diagnostic difficulty [2,3,4,5]. This report presents a symptomatic proximal humerus enchondroma in a 53-year-old female managed successfully with curettage and bone grafting. Enchondromas are benign intramedullary cartilaginous neoplasms arising from residual growth plate cartilage. Although commonly found in the small bones of the hands and feet, long bone involvement, such as the proximal humerus, is less common. Symptomatic lesions in older adults may mimic low-grade chondrosarcoma clinically and radiologically, creating diagnostic difficulty. This report presents a symptomatic proximal humerus enchondroma in a 53-year-old female managed successfully with curettage and bone grafting.
A 53-year-old female presented with complaints of right shoulder pain for 1 year, aggravated over the preceding 15 days. Pain was insidious in onset, gradually progressive, dull aching in nature, aggravated by shoulder movements, and relieved by rest. Mild swelling over the right shoulder was present for 6 months. There was no history of trauma, fever, weight loss, pathological fracture, or constitutional symptoms. The patient was a known case of hypothyroidism on regular medication. The patient was initially treated conservatively with analgesics and physiotherapy, resulting in relief of symptoms.
Clinical examination:
On local examination, mild swelling and tenderness were noted over the proximal humerus and deltoid region. Terminally painful shoulder abduction and painful restriction of internal rotation were observed. Distal neurovascular status, including the distal pulse and sensations, was intact.
Imaging:
Plain radiographs of the shoulder, an anteroposterior view, were taken, which revealed a well-defined osteolytic lesion involving the proximal metaphysis of the right humerus (Fig. 1). Magnetic resonance imaging (MRI) of the shoulder joint demonstrated a hyperintense intramedullary cartilaginous lesion suggestive of an enchondroma with associated chronic tendinosis changes (Fig. 2). Computed tomography (CT) scan of the shoulder demonstrated endosteal scalloping and cortical thinning (Fig. 3).
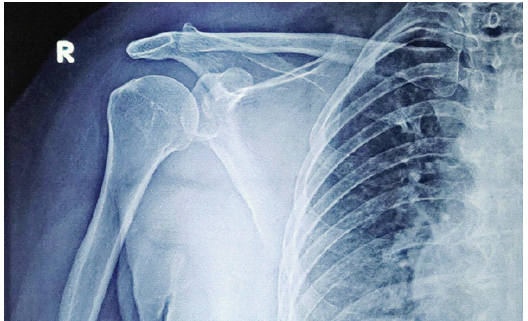
Figure 1: Pre-operative anteroposterior radiograph showing osteolytic lesion in proximal humerus.
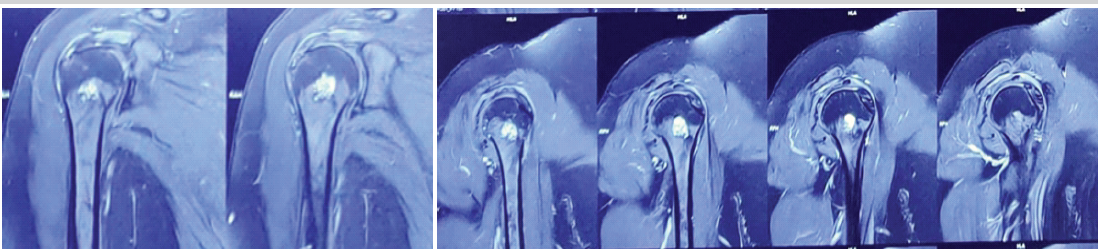
Figure 2: Magnetic resonance images showing an intramedullary cartilaginous lesion.
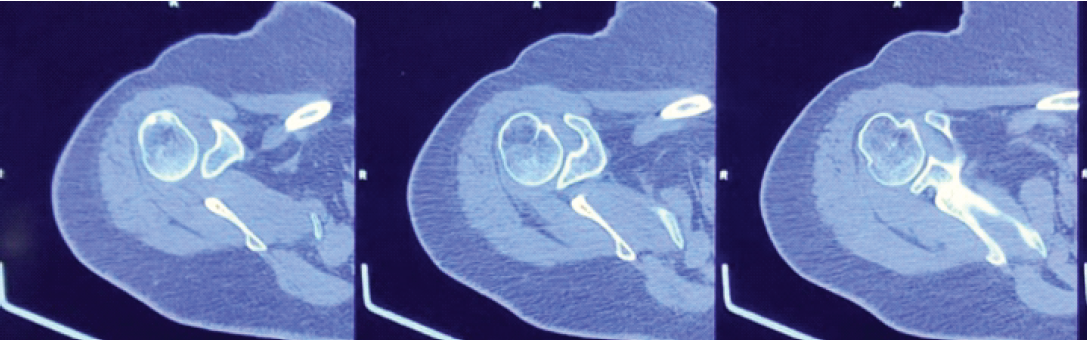
Figure 3: Computed tomography images showing endosteal scalloping and cortical thinning.
Management and hospital course:
The patient was admitted and advised on surgical management. Under strict aseptic precautions, the procedure was performed under general anaesthesia with the patient in a supine position. The skin was painted and draped. A skin incision was made over the lateral aspect of the proximal humerus. The bony lesion was identified under C-arm guidance, and a thorough curettage of the lesion was performed. Samples were sent for histopathological examination. The void in the proximal humerus was filled using beta-tricalcium phosphate granules and hydroxyapatite granules. The skin and soft tissues were closed in layers, and a sterile dressing was applied.
Postoperatively, the patient remained comfortable with satisfactory wound healing and no immediate complications. Pendulum exercises were initiated on post-operative day 2, followed by progressive shoulder mobilisation. Histopathological examination revealed lobules of hyaline cartilage with mild cellularity and mild nuclear atypia, consistent with enchondroma. Preoperatively, the patient’s Visual Analogue Scale (VAS) pain score was 4/10. At the 2-month follow-up, the VAS score improved to 1/10, indicating substantial pain relief. Pre-operative shoulder range of motion was within normal limits, although abduction was painful. At final follow-up, the patient demonstrated a full painless range of shoulder motion without functional restriction. Follow-up radiographs demonstrated satisfactory incorporation of the bone substitute without evidence of recurrence, pathological fracture, graft-related complications, or implant failure (Figs. 4, 5).
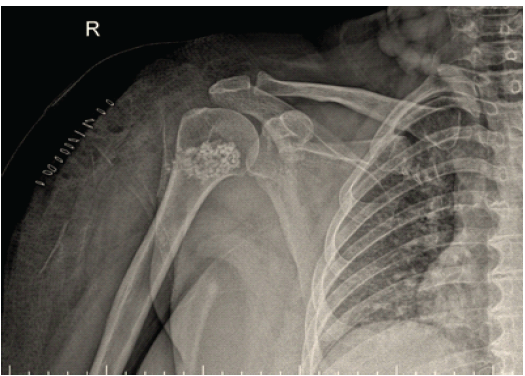
Figure 4: Immediate post-operative radiograph after curettage and bone grafting.
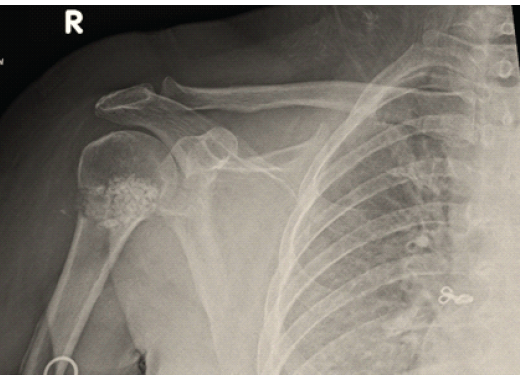
Figure 5: Follow-up radiograph taken at 2 month post-operative showing satisfactory graft incorporation.
Enchondromas are typically benign, asymptomatic cartilaginous tumours; however, painful lesions in long bones require careful assessment to rule out low-grade chondrosarcoma [1,2]. Symptoms such as pain, cortical thinning, and endosteal scalloping are concerning features that often require biopsy [2,4,5]. MRI and CT imaging are crucial in distinguishing benign from malignant cartilaginous lesions [2,4,6,7]. Histopathological examination remains the definitive standard for diagnosis [1,7,8,9]. Surgical treatment, including curettage and bone grafting, remains effective for symptomatic lesions [1,8]. This case highlights the importance of integrating clinical, radiological, and histopathological findings in diagnosing a symptomatic enchondroma of the proximal humerus. Contemporary literature supports intralesional curettage with bone graft substitutes as a reliable treatment option with low recurrence rates and satisfactory functional outcomes in appropriately selected patients [10]. Painful enchondromas of the proximal humerus present a diagnostic challenge because clinical and radiological features may overlap with those of low-grade chondrosarcoma. Features such as persistent pain, cortical thinning, and endosteal scalloping need careful evaluation with advanced imaging and histopathological confirmation. Recent literature supports MRI and CT as valuable modalities for assessing cortical integrity, endosteal scalloping, and soft-tissue extension. Histopathology remains the diagnostic gold standard, although immunohistochemical and molecular studies may further assist in difficult cases. Intralesional curettage remains the preferred treatment for symptomatic benign cartilaginous lesions. In the present case, beta-tricalcium phosphate and hydroxyapatite granules were selected because they eliminate donor-site morbidity associated with autograft harvest, provide structural support, and demonstrate favourable osteoconductive properties. Published series have reported low recurrence rates and satisfactory functional outcomes following curettage and bone substitute augmentation. The favourable early clinical and radiological outcome observed in our patient is consistent with these reports. Nevertheless, long-term follow-up is necessary to evaluate recurrence, graft remodelling, and sustained functional recovery. Curettage followed by defect filling with bone substitutes such as beta-tricalcium phosphates and hydroxyapatite granules remains a safe and effective treatment for symptomatic enchondromas. In this case, surgical management resulted in satisfactory pain relief, improved function, and radiological evidence of graft incorporation without recurrence during follow-up. The procedure avoided complications like pathological fracture and provided a definitive histopathological diagnosis. Longer follow-up and larger studies are needed to further assess the long-term outcomes of graft substitutes and bone void fillers in managing enchondromas of long bones.
Limitations:
This report describes a single patient, and therefore, the findings cannot be generalised to the wider population. The inherent nature of a case report precludes comparison with alternative treatment strategies such as observation, autologous bone grafting, allograft reconstruction, or cement augmentation. Furthermore, the relatively short follow-up period of 2 months is insufficient to evaluate long-term outcomes, including recurrence, graft incorporation, functional durability, or malignant transformation. Objective functional assessment was limited, as validated outcome measures such as the DASH, ASES, or Constant-Murley scores were not utilised. Pain assessment was documented using the VAS, which improved from 4/10 preoperatively to 1/10 postoperatively. Pre-operative shoulder motion was preserved with painful abduction, while post-operative assessment demonstrated a full, painless range of motion. Although histopathological examination confirmed enchondroma, immunohistochemical and molecular studies were not available at our institution. Similarly, an independent second-opinion pathology review was not available. Therefore, differentiation from low-grade chondrosarcoma relied on the combined clinical, radiological, and histopathological findings. Long-term follow-up data were unavailable at the time of manuscript preparation. Potential complications, including graft failure, infection, pathological fracture, persistent pain, recurrence, and long-term graft remodelling, could not be systematically evaluated. Finally, selection bias is unavoidable because only a successfully treated case is presented.
Symptomatic enchondroma of the proximal humerus in older adults can mimic low-grade chondrosarcoma clinically and radiologically. Multimodal imaging and histopathological confirmation are essential for accurate diagnosis. Curettage with bone grafting provides satisfactory clinical and radiological outcomes.
Intralesional curettage followed by bone substitute grafting is an effective treatment option for symptomatic proximal humerus enchondromas, resulting in pain relief and satisfactory radiological healing.
References
- 1. Biondi NL, Tiwari V, Varacallo M. Enchondroma. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024. [Google Scholar] [PubMed]
- 2. Gassert FG, Breden S, Neumann J, Gassert FT, Bollwein C, Knebel C, et al. Differentiating enchondromas and atypical cartilaginous tumours in long bones with computed tomography and magnetic resonance imaging. Diagnostics (Basel) 2022;12:2186. [Google Scholar] [PubMed]
- 3. Wells ME, Childs BR, Eckhoff MD, Rajani R, Potter BK, Polfer EM. A radiological scoring system for differentiation between enchondroma and chondrosarcoma. JAAOS Glob Res Rev 2021;5:e21.00226. [Google Scholar] [PubMed]
- 4. Da Silva GV, Vargas F, Neto P, Serra F, Nelas J, Souto C, et al. Imaging differences between enchondroma and atypical cartilaginous tumour: Insights from a reference centre. J Orthop Rep 2025;5:100673. [Google Scholar] [PubMed]
- 5. Yildirim M, Yildirim H. CT radiomics-based machine learning model for differentiating between enchondroma and low-grade chondrosarcoma. Medicine (Baltimore) 2024;103:e39311. [Google Scholar] [PubMed]
- 6. Engel H, Herget GW, Füllgraf H, Sutter R, Benndorf M, Bamberg F, et al. Chondrogenic bone tumours: The importance of imaging characteristics. Rofo 2021;193:262-75. [Google Scholar] [PubMed]
- 7. Kim D, Jeong JY, Han MH, Jeong W, Chae J, Park I, et al. Periostin is a novel histological biomarker for the diagnosis of chondroid tumours. Transl Cancer Res 2021;10:434-44. [Google Scholar] [PubMed]
- 8. Lanoue G, Wasyliw E, Adams J, Gonzalez F, Wasyliw C. The resolution of a biopsy-proven enchondroma in the proximal humerus over a 14-year interval. Cureus 2025;17:e93194. [Google Scholar] [PubMed]
- 9. Skeletal Lesions Interobserver Correlation among Expert Diagnosticians (SLICED) Study Group. Classification of cartilaginous tumours in long bones: Reproducibility and diagnostic challenges. Virchows Arch 2022;481:687-96. [Google Scholar] [PubMed]
- 10. Parlier-Cuau C, Bousson V, Ogilvie CM, Lackman RD, Laredo JD. Management of enchondromas and atypical cartilaginous tumours of long bones: Current concepts and outcomes. EFORT Open Rev 2023;8:248-58. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Diagnostic Dilemma in a Distal Femoral Intramedullary Lesion: Enchondroma Mimicking Low-Grade Chondrosarcoma with Discordant Biopsy Findings: A Case Report
July 1, 2026 Diagnostic Dilemma in a Distal Femoral Intramedullary Lesion: Enchondroma Mimicking Low-Grade Chondrosarcoma with Discordant Biopsy Findings: A Case Report November 1, 2025 Enchondroma of Hands: A Surgical Dilemma and Our Experience
November 1, 2025 Enchondroma of Hands: A Surgical Dilemma and Our Experience October 10, 2022 Proximal Phalanx Enchondroma with Pathological Fracture Treated with Curettage and Bone Substitute Placement – A Case Report
October 10, 2022 Proximal Phalanx Enchondroma with Pathological Fracture Treated with Curettage and Bone Substitute Placement – A Case Report September 10, 2022 Allograft Impaction and Supplementary Plating for the Management of Epi-Metaphyseal Enchondroma: A Rare Case Report
September 10, 2022 Allograft Impaction and Supplementary Plating for the Management of Epi-Metaphyseal Enchondroma: A Rare Case Report