
Early surgical exploration of atypical mid-shaft humeral fractures with radial-nerve palsy is essential, as unrecognized anatomical variants can lead to true nerve entrapment even outside the classical Holstein–Lewis zone.
Dr Jeff Walter Rajadurai OR, Department of Orthopaedics, Madha Medical College and Research Institute, Chennai, Tamil Nadu, India. E-mail: jeffy.walter@gmail.com
Abstract
Introduction: Radial nerve palsy is a recognised complication of humeral shaft fractures, often associated with distal-third spiral patterns described by Holstein and Lewis. However, authentic mechanical entrapment of the nerve at the mid-shaft level is rather rare. These events test the limits of normal anatomy and show how important it is to look into things right once when fracture geometry suggests possible nerve entrapment.
Case Reports: A 28-year-old right-handed female sustained a humeral fracture at the mid-shaft (AO 12-A3) following a collision with a two-wheeled vehicle. She showed early signs of radial nerve palsy, which meant that her wrist and finger extensors were weak, but her triceps were still working. Radiographs confirmed a transverse fracture/very short oblique configuration. An open reduction and internal fixation within 6 h of injury through the posterior revealed that the radial nerve was stuck between broken pieces of bone and was being compressed by sharp cortical edges. During fixation, the nerve was carefully released and secured. Further dissection proximally revealed an auxiliary branch originating from the radial cord, an anatomical variant. After surgery, rehabilitation included early range-of-motion exercises and wrist splinting. The patient achieved 50% recovery of wrist extension at 12 weeks and complete neurological recovery with full bony union by 24 weeks.
Discussion: This case elucidates that entrapment of the radial nerve can occur at the mid-shaft level when fracture morphology and varied nerve anatomy overlap. Cadaveric studies confirm the variations in radial nerve branching and its proximity to the humeral cortex. Early surgical exploration and decompression are crucial to avoid chronic palsy, particularly when the clinical presentation or fracture morphology is atypical.
Conclusion: Atypical mid-shaft humeral fractures with radial-nerve palsy require prompt surgical evaluation. It is vital to know about high-level radial-nerve branching variants because locating and releasing them early helps the patient fully recover and helps us learn more about the Holstein–Lewis mechanism outside its usual distal zone.
Keywords: Humeral fractures, radial nerve injuries, entrapment neuropathy, anatomical variation, surgical decompression.
Fractures of the humeral shaft are common injuries in orthopaedic practice, constituting almost three per cent of all adult fractures [1]. Radial-nerve palsy is one of their known consequences that stick out since it happens a lot and makes both patients and doctors nervous. The radial nerve runs through the spiral groove and stays close to the humeral cortex for most of its length. This makes it very easy to hurt by moving, pulling, or trapping [2,3,4]. Holstein and Lewis (1963) were the first to show the connection between humeral-shaft fractures and radial-nerve palsy. They did this by describing a typical distal-third spiral fracture that caused nerve entrapment at the lateral intermuscular septum [2]. Their description overwhelmingly influenced orthopaedic knowledge for decades together, thus highlighting the necessity for thorough attention during both diagnosis and fixation. However, further research has shown that radial nerve injury can occur at any level of the humeral shaft, not just in its distal third [4,5,6,7]. The majority of radial-nerve palsy cases are neuropraxic in nature and resolve spontaneously within weeks [4,6]. A few arise from mechanical entrapment of the nerve between fracture fragments, necessitating prompt surgical inspection and release [8,9]. It is essential to distinguish between these entities: Neuropraxia typically indicates a transitory conduction block, but genuine entrapment poses a danger of enduring malfunction or secondary axonotmesis if not alleviated [10,11]. Modern-day imaging and intraoperative observations have enhanced this comprehension. Hendrickx et al. [4] and Hegeman et al. [6] showed that most closed fractures with primary palsy can be safely managed expectantly, although a small number with transverse or spiral shapes may hide nerve entrapment. Böhringer et al. [9], in their recent research “Revision or Wait and See?”, emphasised that while observation is the standard practice, clinical suspicion should take preference over established norms when fracture geometry or intra-operative indicators suggest entrapment. This study presents a different perception by detailing a mid-shaft (AO 12-A3) transverse fracture with intra-operative radial nerve entrapment, serving as a proximal equivalent of the Holstein–Lewis mechanism. This instance showed that the nerve was promptly between the ends of the fracture, which is different from the conventional distal spiral pattern. The complete neural recovery after meticulous release and dynamic compression plating supports the idea that the Holstein–Lewis phenomenon goes beyond anatomical limits and is instead guided by the character of the fracture and the radial nerve’s natural weakness, making it a true Holstein–Lewis-like variant.
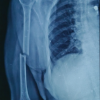
A 28-year-old female who was right-handed and functionally active arrived at the emergency room after a two-wheeler crash. She stated that she was in a lot of pain, her right arm was swollen, and she could not move it. The distal end did not have an open wound or a problem with the blood vessels. On inspection, she had abnormal mobility at the shaft centre. The patient could not extend her wrists and fingers, but her triceps strength was still relatively intact. This is a characteristic of radial nerve palsy. The sensation on the back of the hand was slightly diminished. Plain radiographs (antero-posterior and lateral views) revealed a transverse/short oblique fracture of the mid-shaft of the humerus, matching an AO 12-A3 pattern (Fig. 1).

Figure 1: Pre-operative X-ray.
A diagnosis of a closed mid-shaft fracture of the right humerus with primary radial nerve palsy was established based on clinical and radiological data. Because of the sudden onset and the radial nerve palsy, surgery was planned to stabilise the area through the posterior for aesthetic reasons. The surgery was performed within 6 hours of injury. During the operation, the radial nerve was seen to be running along the spiral groove. The team was startled to find that the nerve was wedged between the proximal and distal fracture fragments. The sharp edges of the cortical bone had crushed it, but its continuity was maintained. Fine micro-dissection was performed to carefully extricate the nerve from the entrapped site, and an infant feeding tube was employed to protect the nerve during the entire process. To see if the nerve’s anatomy had variation, further dissection was done in proximity to it. It was remarkable that there was a branch from the main cord of the radial nerve near the fracture. In the end, the nerve was retained in its entirety. After the nerve was entirely secured, the fracture was fixed and reduced with a 4.5 mm titanium dynamic compression plate that had four cortices of purchase on each side (Fig. 2).
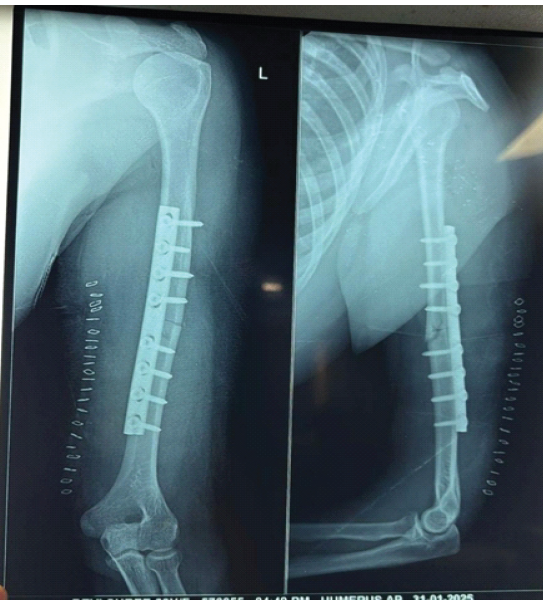
Figure 2: Immediate post-operative X-ray.
It was vital to retain the physiological humerus bow in place and not put too much pressure on the nerve when putting the plate in place. The radial nerve and its branches were spared harm during the entire surgery. The limb was put in a sling after the surgery, and the patient was given clear instructions on how to move the fingers and raise the limb. Periodic neurovascular function was examined. To prevent the shoulder and elbow from getting stiff, passive and active-assisted range-of-motion (ROM) exercises began the day following surgery. A wrist-extension splint was put on to support the wrist that had dropped, and an arm pouch was given to keep the elbow from sagging and minimise the swelling that builds up in the arm. Every 2 weeks, there were adequate clinical examinations. By the 4th week, the wrist extensors were evidently flickering and improved progressively. The patient’s wrist extension had improved by 50% after 12 weeks, and their shoulder and elbow joints had almost full ROM re-established. At 24 weeks, the patient demonstrated complete recovery of radial nerve motor function and had no neurological deficits. Radiographs at each step confirmed progressive osseous union (Fig. 3, 4, 5).
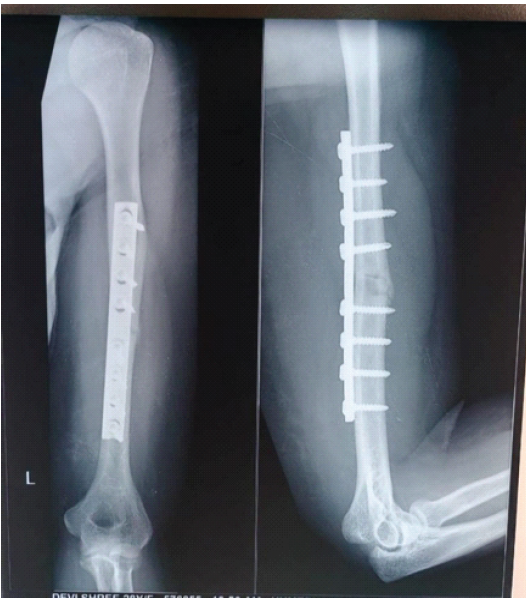
Figure 3: Three-month follow-up X-ray.

Figure 4: Six-month follow-up X-ray.
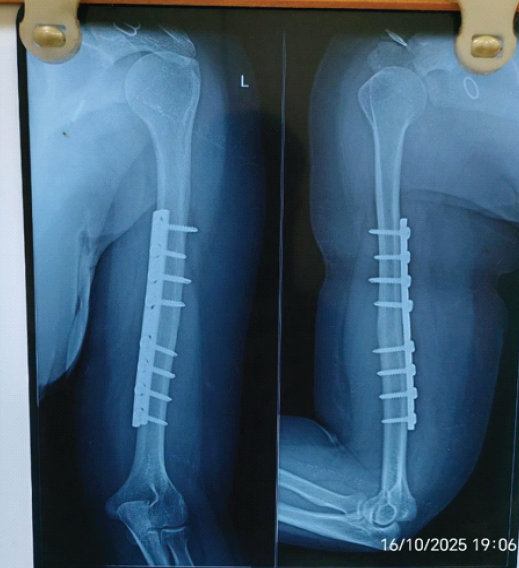
Figure 5: Eight-month follow-up X-ray.
The intra-operative images with the nerve secured and the plate fixed are shown in Figs 6, 7, and 8. There were no complications following surgery, with the implant, or loss of sensation during follow-up.
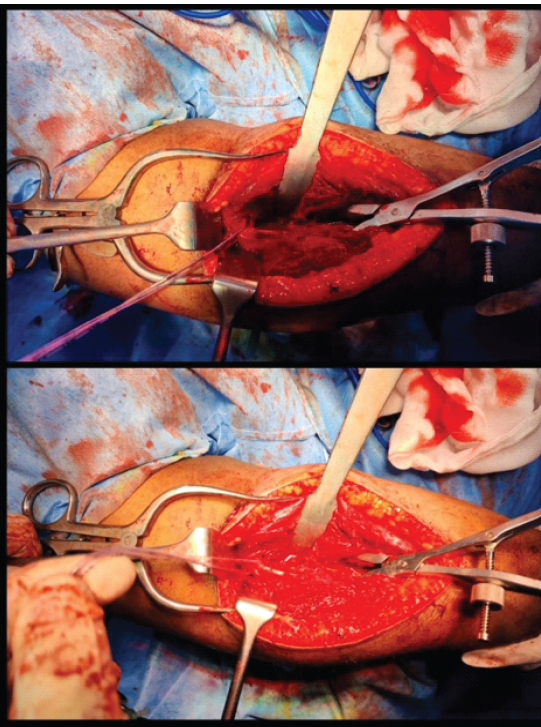
Figure 6: Intra-operative clicks showing the main radial cord and the auxiliary branch.
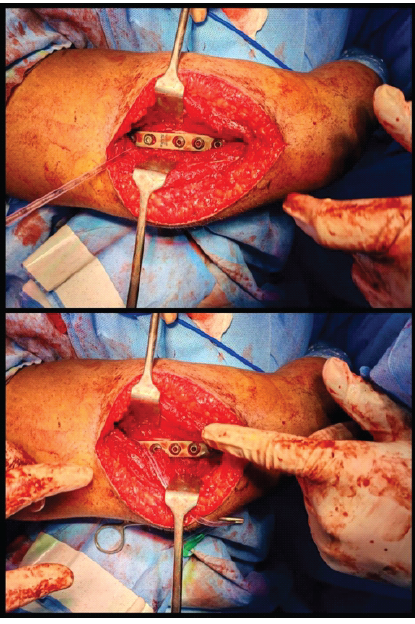
Figure 7: Intra-operative clicks showing the nerve and the branch being preserved using an infant feeding tube while the plate was fixed.

Figure 8: The incision was made posteriorly for cosmesis.
The patient was able to go back to work and complete her normal daily chores without any difficulty at the end of the 3rd month (Fig. 9). After 6 months, she started riding her bike.

Figure 9: Patient showing comparative functional gain.
There have been many reports of radial nerve palsy linked to humeral-shaft fractures, but the anatomy of the nerve and its variation has always perplexed the surgeons. Holstein and Lewis (1963) were the first to talk about the distal-third spiral fracture as a rare event that happens when the radial nerve becomes compressed at the lateral intermuscular septum, which causes motor impairments [2]. Subsequent literature substantiates that these injuries constitute the principal aetiology of radial nerve palsies associated with humeral fractures, frequently representing 8–12% of patients [3,5]. Nonetheless, a limited percentage of these occurrences transpire outside the typical distal zone, rendering mid-shaft entrapment a notable event [4,6,7,9]. This case contributes to a narrow collection of reported incidents by detailing a mid-shaft (AO 12-A3) transverse/very short oblique fracture, wherein the radial nerve was mechanically entrapped between the fracture fragments, as confirmed at the time of surgery. The torsional spiral structure of the Holstein–Lewis fracture was not seen in this pattern. Instead, it had a transverse break/a very short oblique with torsional shear. This caused the nerve to slip between the cortical ends and get compressed as the pieces recoiled. This can be correlated with the specific symptoms like weakness in the wrist and finger extensors while leaving the triceps alone. This suggests that the lesion is between the triceps branches and the radial bifurcation. This fracture and nerve compression pattern is not very common. Recent studies on humeral-shaft fractures with early radial-nerve palsy indicate that only 2–3% exhibit genuine nerve compression between fragments [4,6,7,9]. In the majority of instances, neuropraxia induced by traction or contusion resolves spontaneously within a few weeks [6,12]. Entrapment requires immediate surgical intervention, as prolonged compression can lead to axonotmesis and permanent impairment [8,10,11,13,14,15]. One significant aspect of this report was the intraoperative instinct to extend the dissection proximally beyond the spiral groove. This meticulous examination identified an additional branch originating directly from the radial chord, situated nearer to the body than the conventional bifurcation into superficial and deep branches. To our knowledge, this observation made during surgery has never been documented before in cases of acute fracture. Anatomical studies show that there are variations in radial nerve anatomy. Cadaveric studies by Sawyer et al. revealed significant individual variability in the motor branching pattern of the radial nerve in the forearm, including the early separation of muscular branches [16]. Otake et al. noted that the branching connection between the radial nerve and its target muscles differs in amount, origin, and level, with certain branches emerging more proximally than traditional descriptions indicate [17]. These results are consistent with those of Prasad and Isaac, who noted irregular branch origins to the triceps, indicating that proximal divisions are feasible and may facilitate the proximity of neuronal structures to the humeral cortex [18]. Additional evidence from Ramos e Silva et al. substantiated the presence of various development locations for motor branches in the elbow area, emphasising that the route of the radial nerve should not be regarded as uniform among individuals [19]. The superficial branch, formerly classified as sensory, has demonstrated unanticipated trajectories and emergence levels [20]. These investigations collectively establish a robust anatomical basis for the hypothesis that diverse high-level branching may increase the likelihood of nerve entrapment in atypical locations, as evidenced in this case report. Table 1 shows the significant distinctions between this case and other key studies that have been published. In this case, the idea of the Holstein–Lewis idea has changed from an anatomical region to mechanical compression. The report teaches us that the pattern of the fracture and the course of the nerve are also essential. The same phenomenon can happen when the fracture pattern and nerve course overlap, no matter how close or far apart they are. The swift neurological enhancement post-decompression in this instance corroborates the idea that mechanical issues require mechanical remedies.
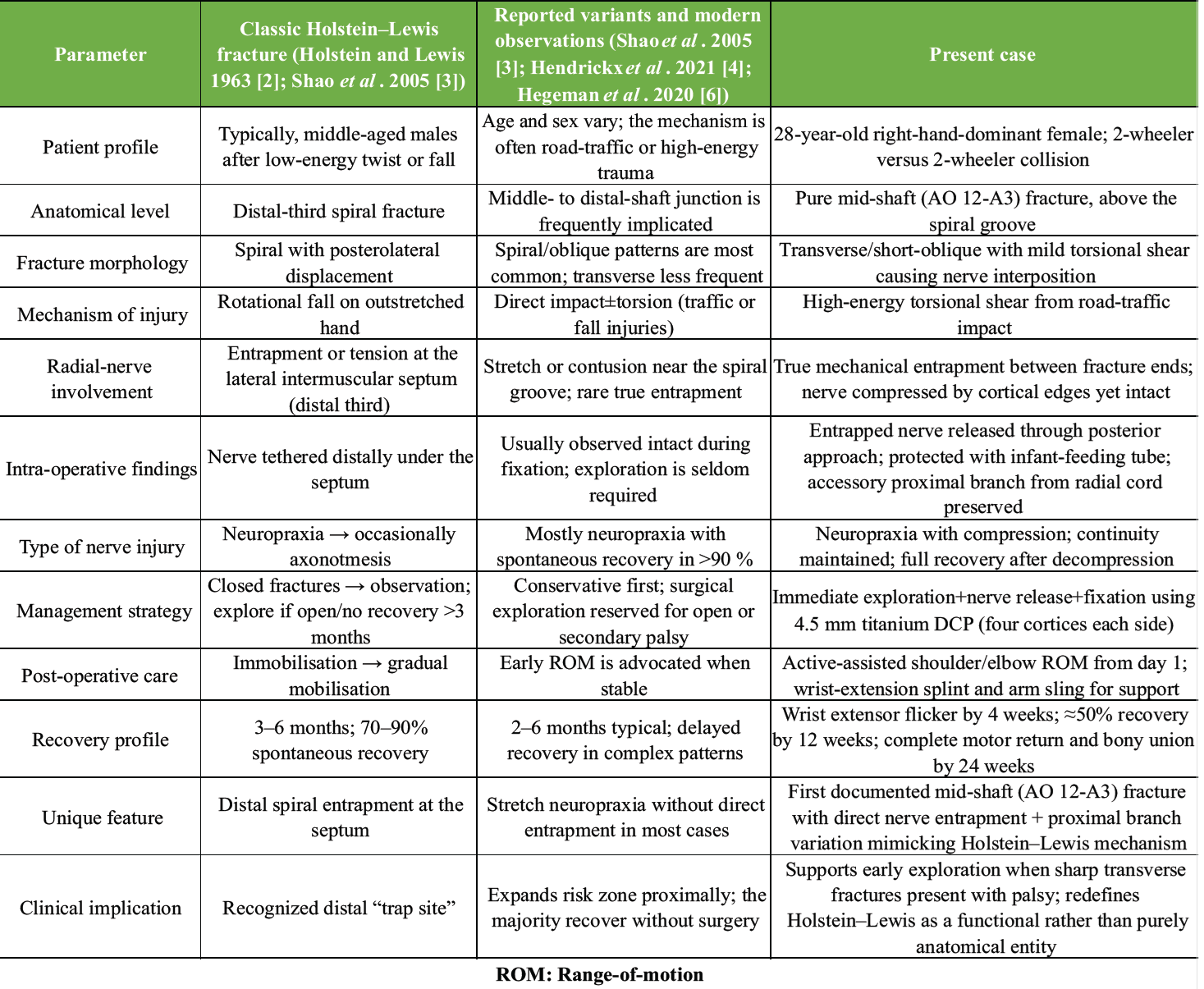
Table 1: Differences between the present case and other key reported literature
Limitations:
This report represents a single-case observation; therefore, the results cannot be generalised to all mid-shaft humeral fractures linked to radial nerve palsy. As with any case study, causal relationships or incidence patterns cannot be established. This article does not assert the superiority of early surgical surgery, as it lacks comparisons with conservatively handled cases or delayed exploratory options. The intra-operative identification of an additional radial nerve branch indicates an uncommon anatomical variation that may not be seen in typical clinical settings. Pre-operative sophisticated imaging modalities, like magnetic resonance imaging or high-resolution ultrasound, were not utilised to identify nerve entrapment. The decision for early exploration was mostly determined by clinical presentation and fracture morphology. The assessment of neurological recovery was conducted clinically, lacking conventional grading systems or electrophysiological evaluations, which may limit objective measurement of recovery. The patient came on time and underwent surgical intervention within 6 h, which may not reflect outcomes in instances of delayed presentation. This research reflects the experience of a singular surgical team at one institution, necessitating additional follow-up to assess the long-term sustainability of neurological recovery. Ultimately, the inherent publishing bias associated with infrequent positive outcomes must be acknowledged.
This case study strengthens the traditional knowledge of the Holstein–Lewis injury by showing that radial-nerve entrapment can happen at the mid-shaft when the pattern of fracture and differences in anatomy meet. The surgical discovery of a proximal auxiliary branch from the radial cord, supported by known anatomical literature, highlights that the to-be-careful area for nerve injury is beyond conventional zones. Early examination and meticulous dissection were crucial in transforming a potential permanent palsy into complete healing. This report finally illustrates that successful trauma surgery depends on fundamentals beyond just the restoration technique. It also depends on how skilled the surgeon is at suspecting unusual patterns where anatomy and mechanics interact, thus expecting intra-operative surprises.
Mid-shaft humeral fractures, though rarely associated with radial-nerve entrapment, demand a high index of suspicion and careful proximal exploration, as early recognition and release of variant nerve anatomy can prevent permanent neurological deficit and ensure complete functional recovery.
References
- 1. Ekholm R, Adami J, Tidermark J, Hansson K, Törnkvist H, Ponzer S. Fractures of the shaft of the humerus. An epidemiological study of 401 fractures. J Bone Joint Surg Br 2006;88:1469-73. [Google Scholar] [PubMed]
- 2. Holstein A, Lewis GM. Fractures of the humerus with radial-nerve paralysis. J Bone Joint Surg Am 1963;45:1382-8. [Google Scholar] [PubMed]
- 3. Shao YC, Harwood P, Grotz MRW, Limb D, Giannoudis PV. Radial nerve palsy associated with fractures of the shaft of the humerus: A systematic review. J Bone Joint Surg Br 2005;87:1647-52. [Google Scholar] [PubMed]
- 4. Hendrickx L AM, Van Der Velde D, Van Den Bekerom MP, Van Den Wildenberg FJ, Van Noort A. Radial nerve palsy associated with closed humeral shaft fractures: A systematic review. Eur J Orthop Surg Traumatol 2020;30:279-89. [Google Scholar] [PubMed]
- 5. Li Y, Ning G, Wu Q, Wu Q, Li Y, Feng S. Review of literature of radial nerve injuries associated with humeral fractures-an integrated management strategy. PLoS One 2013;8:e78576. [Google Scholar] [PubMed]
- 6. Hegeman EM, Roolker W, Van Der Beek D, Van Noort A, Hogervorst M. Incidence and management of radial nerve palsies in closed humeral shaft fractures: Analysis of 450 patients. Injury 2020;51 Suppl 2:S53-61. [Google Scholar] [PubMed]
- 7. Chang G, Spencer HT. Radial nerve palsy after humeral shaft fractures. Hand Clin 2018;34:291-301. [Google Scholar] [PubMed]
- 8. Samardžić M, Grujicić D, Milinković ZB. Radial nerve lesions associated with fractures of the humeral shaft. Injury 1990;21:220-2. [Google Scholar] [PubMed]
- 9. Böhringer A, Bäcker R, Geyer M. Primary radial nerve lesions in humerus shaft fractures-revision or wait and see? J Orthop Case Rep 2024;14:53-8. [Google Scholar] [PubMed]
- 10. Seddon HJ. Three types of nerve injury. Brain 1943;66:237-88. [Google Scholar] [PubMed]
- 11. Sunderland S. A classification of peripheral nerve injuries producing loss of function. Brain 1951;74:491-516. [Google Scholar] [PubMed]
- 12. Shi S, Ou X, Du X. Enhanced nerve function recovery in radial nerve palsy patients with humerus shaft fracture: A randomized study of low-frequency pulse electrical stimulation combined with exercise therapy. Front Neurol 2024;15:1370316. [Google Scholar] [PubMed]
- 13. Meinberg EG, Agel J, Roberts CS, Karam MD, Kellam JF. Fracture and dislocation classification compendium-2018. J Orthop Trauma 2018;32 Suppl 1:S1-170. [Google Scholar] [PubMed]
- 14. Chhabra A, Lee SK, Flammang AJ, Belzberg AJ. Peripheral nerve injury grading simplified on MR neurography. AJR Am J Roentgenol 2014;203:553-63. [Google Scholar] [PubMed]
- 15. Weisberg ZS, Wolf JM. Radial nerve palsy in the setting of humeral shaft fracture. J Hand Surg Am 2024;49:690-7. [Google Scholar] [PubMed]
- 16. Sawyer JR, Davis BR, Pugh NA. The branching and innervation pattern of the radial nerve in the forearm. Anat Sci Int 2020;95:517-25. [Google Scholar] [PubMed]
- 17. Otake Y, Kimura K, Matsui H. Relationship between the branching patterns of the radial nerve and its target muscles in the forearm: A cadaveric study. PLoS One 2021;16:e0258129. [Google Scholar] [PubMed]
- 18. Prasad M, Isaac B. Variations in the branching pattern of the radial nerve branches to triceps brachii muscle. J Clin Diagn Res 2019;13:AC01-5. [Google Scholar] [PubMed]
- 19. Ramos e Silva M, Souza MJ, Prado GF. An anatomical study of motor branches of the radial nerve in the elbow region. Rev Bras Ortop 2014;49:587-92. [Google Scholar] [PubMed]
- 20. Haugen TW, Cannady SB, Chalian AA, Shanti RM. Anatomical variations of the superficial radial nerve encountered during radial forearm free flap elevation. ORL J Otorhinolaryngol Relat Spec 2019;81:155-8. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2025 Atypical Transverse Midshaft Humerus Fracture in an Octogenarian: Surgical Nuances and Functional Outcome Following Locked Intramedullary Nailing
November 1, 2025 Atypical Transverse Midshaft Humerus Fracture in an Octogenarian: Surgical Nuances and Functional Outcome Following Locked Intramedullary Nailing December 10, 2021 Recurrent Giant Cell Tumor of Distal Radius with Pulmonary Metastasis: A Case Report
December 10, 2021 Recurrent Giant Cell Tumor of Distal Radius with Pulmonary Metastasis: A Case Report February 10, 2021 Reviewers Acknowledgement & Photo-gallery February 2021
February 10, 2021 Reviewers Acknowledgement & Photo-gallery February 2021 December 1, 2025 Biomechanical Reinforcement of a Bucket-handle Lateral Meniscus Tear Using Circumferential Fiber Augmentation: A Case Report
December 1, 2025 Biomechanical Reinforcement of a Bucket-handle Lateral Meniscus Tear Using Circumferential Fiber Augmentation: A Case Report