
The Masquelet technique with a non-vascularised fibular strut graft effectively treats large tibial bone defects in children, providing structural support, reducing graft volume, enabling earlier weight-bearing, and allowing full fibular regeneration with careful periosteal preservation.
Dr. Shakil Ahmad, Department of Orthopedic Surgery, Sohar Hospital, Ministry of Health, Sohar, Oman. E-mail: dr.shakilortho@gmail.com
Abstract
Introduction: Compound tibial fractures with large segmental bone defects present a formidable reconstructive challenge, particularly in the skeletally immature population. While the Masquelet-induced membrane technique has emerged as a reliable method for managing critical-sized bone defects, its use with morselised cancellous bone alone limits early weight-bearing and mechanical stability. We describe a modification combining the Masquelet technique with a non-vascularised mid-shaft fibular strut graft to address these limitations.
Case Report: A 14-year-old boy sustained an open fracture of the right tibia and fibula (Gustilo-Anderson type IIIB) with an approximately 6 cm segmental tibial bone defect following a motor vehicle collision. Management involved a staged approach: initial wound debridement and external fixation, followed by open reduction and internal fixation with a dynamic compression plate and polymethylmethacrylate cement spacer impregnated with gentamicin. At 11 weeks, the cement spacer was removed, and the defect was reconstructed using a non-vascularised mid-shaft fibular strut graft placed intramedullarily within the induced membrane, augmented with a bi-cortical iliac crest bone graft. The patient achieved partial weight-bearing at 24 weeks, full weight-bearing at 33 weeks, and resumed normal activities by 39 weeks post-injury. Follow-up radiographs demonstrated satisfactory bone union with complete regeneration of the fibular donor site.
Conclusion: Combining the Masquelet technique with a non-vascularised fibular strut graft is a viable option for reconstructing large tibial bone defects in skeletally immature patients. This approach provides structural support, reduces cancellous graft requirements, enables earlier weight-bearing, and achieves complete donor site regeneration in the growing skeleton.
Keywords: Masquelet technique, induced membrane, fibular strut graft, non-vascularized, tibial bone defect, compound fracture, skeletally immature, Gustilo-Anderson IIIB.
Compound tibial fractures with large segmental bone defects remain one of the most challenging scenarios in orthopaedic trauma surgery [1,2]. These injuries are frequently encountered following high-energy mechanisms such as motor vehicle collisions and are often complicated by extensive soft-tissue damage, periosteal stripping, and contamination, all of which compromise the biological environment necessary for bone healing [3]. The management challenge is further amplified in skeletally immature patients, where preserving growth potential and minimising donor site morbidity are paramount considerations. Several reconstructive strategies have been described for managing critical-sized bone defects. Simple autologous cancellous bone grafts tend to undergo resorption when the defect exceeds 6 cm [4]. Free vascularised fibular grafts offer a biological solution but require microsurgical expertise that may not be readily available in all settings [5,6]. Allografts carry substantial risks of non-union (35%), graft fracture (16.4%), and infection (5.4%), as reported in large series [2,3]. The Ilizarov distraction osteogenesis technique, while effective, demands prolonged treatment duration and patient compliance, which can be particularly challenging in the paediatric population [7]. The Masquelet-induced membrane technique has gained increasing acceptance as a reliable two-stage approach for reconstructing large bone defects [4,8]. In the first stage, a polymethylmethacrylate (PMMA) cement spacer is placed after thorough debridement, which induces the formation of a biologically active pseudo-synovial membrane rich in vascular endothelial growth factor (VEGF), transforming growth factor-β1 (TGF-β1), and bone morphogenetic protein-2 (BMP-2) [9]. In the second stage, the cement spacer is removed, and the defect is filled with morselised autologous cancellous bone graft within this vascularised membrane envelope [8]. However, the gold standard use of a cancellous bone graft alone provides limited structural support, restricting weight-bearing until consolidation is achieved [10]. Recent reports have proposed combining the Masquelet technique with structural grafts to overcome this limitation [11,12]. We present the case of a skeletally immature patient with a Gustilo-Anderson Type IIIB open tibial fracture and a 6 cm segmental bone defect, successfully managed using the Masquelet technique combined with a non-vascularised mid-shaft fibular strut graft. This modification provided structural support, reduced cancellous graft requirements, and facilitated earlier weight-bearing and favourable functional recovery.
Patient information and presentation:
A 14-year-old boy, with a known history of glucose-6-phosphate dehydrogenase deficiency, presented to the accident and emergency department of Sohar Hospital on October 28, 2023, following a motor vehicle collision (rollover accident) in which he was a rear-seat passenger. On initial assessment, the patient was haemodynamically stable. Abdominal computed tomography revealed a right suprarenal gland haematoma (40 × 22 mm), which was managed conservatively following general surgical clearance. An orthopaedic examination revealed an open fracture of the right tibia and fibula, classified as Gustilo-Anderson Type IIIB. There were two open wounds on the right leg: A 15 cm wound over the medial (shin) aspect and an 8 cm wound on the anterolateral aspect with exposed muscle. There was no clinical evidence of vascular injury, and distal pulses were intact (Fig. 1).

Figure 1: Clinical photograph of the open fracture (Gustilo-Anderson Type IIIB) of the right leg at presentation in the emergency department, demonstrating the extent of soft-tissue injury.
Initial management (Day 0 – October 28, 2023) In the emergency department, the wounds were thoroughly irrigated with normal saline and dressed. An above-the-knee plaster slab was applied for temporary stabilisation. X-rays were done, which showed a highly comminuted fracture of the tibia and fibula (Fig. 2).

Figure 2: Anteroposterior and lateral radiographs of the right leg at presentation, showing comminuted fractures of the tibia and fibula with segmental bone loss.
The patient was taken to the operating theatre within hours of admission. Intraoperative assessment confirmed severe soft-tissue loss on the medial aspect, a segmental tibial bone defect of approximately 6 cm at the fracture site, and crush injury to the lateral compartment extensor muscles. Thorough wound debridement was performed, and a bridging external fixator was applied to the right tibia for provisional stabilisation.
Stage 1: Definitive fixation and cement spacer placement (Day 4 – November 01, 2023):
At the second operative procedure, wound swabs were obtained from both the medial and lateral wounds; infection was subsequently excluded. On inspection, the wounds were clean, and the exposed muscles were viable. The external fixator was removed, and definitive open reduction and internal fixation were performed. The fibula was stabilised using an 11-hole one-third semi-tubular plate, and the tibia was fixed with a 12-hole dynamic compression plate. The segmental tibial bone defect was filled with a PMMA bone cement spacer impregnated with gentamicin to induce membrane formation in accordance with the first stage of the Masquelet technique (Fig. 3). The wounds were again thoroughly irrigated with normal saline and closed primarily.
The patient was followed up in the outpatient clinic with serial wound assessments until complete soft-tissue healing was achieved.

Figure 3: Post-operative anteroposterior and lateral radiographs showing internal fixation with the cement spacer in situ.
Stage 2: Cement spacer removal and bone grafting (Week 11 – January 11, 2024):
At the second-stage procedure (approximately 11 weeks after the index injury), the cement spacer was carefully removed, preserving the induced membrane. The intramedullary canal was canalised, and the fracture ends were refreshed by shingling to promote a vascular response. A non-vascularised cortical strut graft was harvested from the ipsilateral mid-shaft fibula with meticulous periosteal preservation to facilitate donor site regeneration. The fibular strut graft was placed intramedullarily within the induced membrane cavity to provide structural support (Fig. 4).
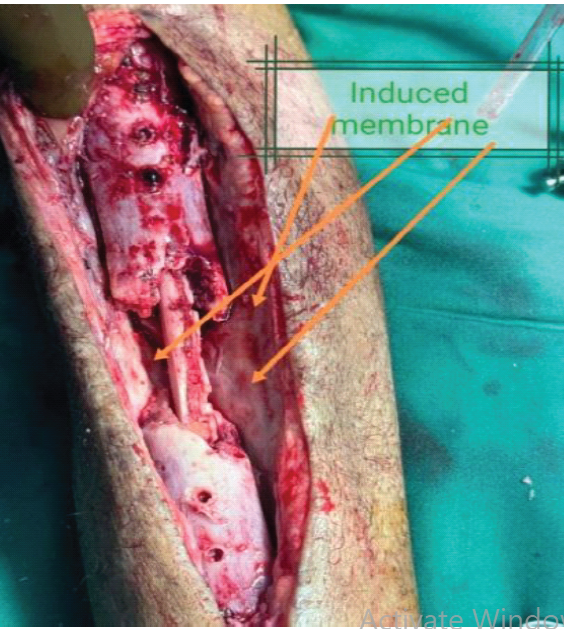
Figure 4: Intraoperative photograph demonstrating the intramedullary fibular strut graft within the induced membrane.
The remaining defect was augmented with a bi-cortical autologous bone graft harvested from the right iliac crest. No drill holes were made on the fibular graft surface, as incorporation proceeded satisfactorily without this additional step (Fig. 5).

Figure 5: Post-operative anteroposterior radiographs of both legs following bone grafting.
Post-operative rehabilitation and follow-up:
The patient was initially permitted toe-touch weight-bearing and was followed up regularly in the outpatient clinic. The rehabilitation milestones were as follows: Partial weight-bearing was initiated at 24 weeks post-injury (April 21, 2024), and the patient progressed to full weight-bearing at 33 weeks (June 23, 2024). Follow-up radiographs demonstrated satisfactory and progressive bone union at the reconstruction site. Notably, the fibular donor site showed complete bone regeneration, consistent with the regenerative capacity of the skeletally immature skeleton when the periosteum is preserved (Fig. 6).
Patient regained normal unrestricted activity at 39 weeks (August 06, 2024) (Fig. 7).
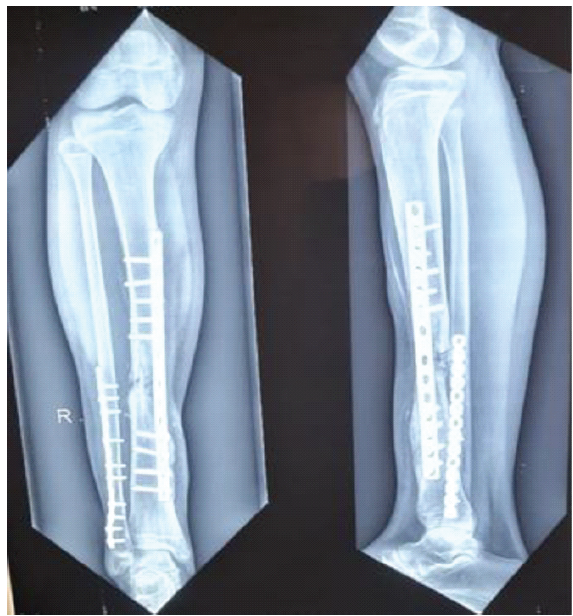
Figure 6: Follow-up anteroposterior and lateral radiographs demonstrating satisfactory bone union.

Figure 7: Clinical photograph of the patient after complete wound healing and resumption of normal activities.
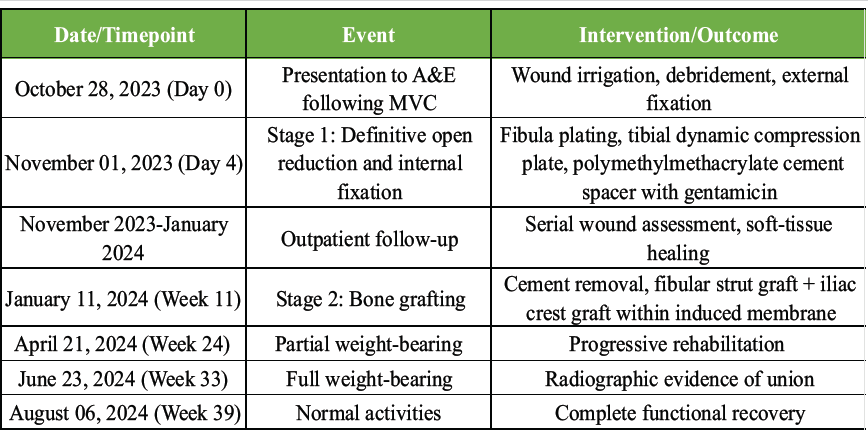
Table 1: Timeline
Timeline: (Table 1)
The management of compound tibial fractures with large segmental bone defects continues to challenge orthopedic surgeons, with no single technique universally accepted as the optimal treatment [1,4]. This case demonstrates that the Masquelet-induced membrane technique, when combined with a non-vascularized fibular strut graft, provides an effective and reproducible solution for reconstructing critical-sized tibial bone defects in the skeletally immature population. The conventional Masquelet technique relies on morselized cancellous bone graft (1–2 mm) to fill the defect within the induced membrane [4,8]. While this approach capitalizes on the rich biological environment of the membrane – which secretes VEGF, TGF-β1, and BMP-2 to promote osteogenesis and neovascularization – it provides limited structural support [4]. Consequently, patients must remain non-weight-bearing until radiographic evidence of consolidation, which may take several months [10]. In pediatric patients, prolonged immobilization carries additional risks of muscle atrophy, joint stiffness, and psychosocial impact. Several authors have proposed modifications to enhance the structural properties of the Masquelet technique. Gannamani et al. [12] recently reported a promising approach combining non-vascularized fibula and cancellous graft within the Masquelet technique for distal femoral defects, demonstrating favorable outcomes. El-Alfy et al. [11] described the use of free non-vascularized fibular grafts within the induced membrane for post-traumatic tibial defects, reporting successful union in their series. The modified Capanna technique, combining vascularized fibula with allograft, has shown excellent results for large defects but requires microsurgical expertise [6]. In the present case, the non-vascularized mid-shaft fibular strut graft was placed intramedullarily to serve as a structural scaffold within the induced membrane. This modification conferred several advantages. First, the cortical bone graft provided immediate mechanical support, enabling earlier partial weight-bearing at 24 weeks compared with the prolonged non-weight-bearing period typically associated with the standard Masquelet technique. Second, the fibular strut reduced the volume of cancellous bone graft required, thereby decreasing iliac crest donor site morbidity. Third, the technique does not require microsurgical skills, making it feasible in centers without vascular surgery capabilities. An important finding in this case was the complete regeneration of the fibular donor site, which is attributable to the meticulous preservation of the periosteal sleeve during graft harvest. This regenerative capacity is particularly robust in skeletally immature patients [12,13]. Furthermore, we observed satisfactory graft incorporation without the need for multiple drill holes on the fibular graft surface, which contrasts with some previously described techniques and simplifies the procedure. The Gustilo-Anderson Type IIIB classification of this injury underscores its severity, with extensive soft-tissue loss and periosteal stripping [9]. The staged approach allowed for adequate soft-tissue healing before definitive bone reconstruction, which is critical for reducing infection risk and optimizing the biological environment for graft incorporation [14,15]. The use of gentamicin-impregnated cement in the first stage served the dual purpose of inducing membrane formation and providing local antibiotic prophylaxis against infection [1]. The patient’s age (14 years) merits specific discussion. The Masquelet technique has been less extensively studied in the pediatric population compared with adults [12]. Gouron et al. [12] reported a series of 14 children treated with the induced membrane technique, demonstrating its efficacy and safety in the growing skeleton. The present case adds to this evidence and highlights the particular advantage of fibular donor site regeneration in skeletally immature patients. Several limitations of this report should be acknowledged. As a single case report, the generalizability of our findings is limited. Formal functional outcome assessment using validated instruments, such as the Lower Extremity Functional Scale [16], would strengthen future reports. Long-term follow-up is warranted to assess for potential complications, including graft resorption, refracture, or growth disturbance. In addition, the contribution of the induced membrane versus the fibular strut graft to the observed outcome cannot be independently quantified.
This case demonstrates that the Masquelet-induced membrane technique, when combined with a non-vascularised mid-shaft fibular strut graft, is a viable and effective strategy for reconstructing large segmental tibial bone defects in skeletally immature patients. The approach provides structural support for earlier weight-bearing, reduces cancellous bone graft requirements, does not require microsurgical expertise, and achieves complete fibular donor site regeneration in the growing skeleton. This modification merits further evaluation through larger case series and comparative studies to establish its role in the orthopaedic armamentarium for managing complex tibial bone loss.
Compound tibial fractures with large segmental bone loss in skeletally immature patients can be successfully managed by combining the Masquelet-induced membrane technique with a non-vascularized mid-shaft fibular strut graft. This approach offers a technically accessible alternative to microsurgical reconstruction, enables earlier weight-bearing, and capitalizes on the regenerative potential of the pediatric skeleton at the fibular donor site.
References
- 1. Kasha S, Rathore SS, Kumar H. Antibiotic cement spacer and induced membrane bone grafting in open fractures with bone loss: A case series. Indian J Orthop 2019;53:237-45. [Google Scholar] [PubMed]
- 2. Matejovsky Z Jr., Matejovsky Z, Kofranek I. Massive allografts in tumour surgery. Int Orthop 2006;30:478-83. Delloye C, Van Cauter M, Dufrane D, Francq BG, Docquier PL, Cornu O. Local complications of massive bone allografts: An appraisal of their prevalence in 128 patients. Acta Orthop Belg 2014;80:196-204.[TPS1.1] [Google Scholar] [PubMed]
- 3. Masquelet AC, Begue T. The concept of induced membrane for reconstruction of long bone defects. Orthop Clin North Am 2010;41:27-37. Gustilo RB, Gruninger RP, Davis T. Classification of type III (severe) open fractures relative to treatment and results. Orthopedics 1987;10:1781-8.[TPS2.1] [Google Scholar] [PubMed]
- 4. Pacelli LL, Gillard J, McLoughlin SW, Buehler MJ. A biomechanical analysis of donor-site ankle instability following free fibular graft harvest. J Bone Joint Surg Am 2003;85:597-603. [Google Scholar] [PubMed]
- 5. Wang P, Wu Y, Rui Y, Wang J, Liu J, Ma Y. Masquelet technique for reconstructing bone defects in open lower limb fracture: Analysis of the relationship between bone defect and bone graft. Injury 2021;52:988-95. [Google Scholar] [PubMed]
- 6. Ronga M, Ferraro S, Fagetti A, Cherubino M, Valdatta L, Cherubino P. Masquelet technique for the treatment of a severe acute tibial bone loss. Injury 2014;45 Suppl 6:S111-5. [Google Scholar] [PubMed]
- 7. El-Alfy B, Abulsaad M, Abdelnaby WL. The use of free nonvascularized fibular graft in the induced membrane technique to manage post-traumatic bone defects. Eur J Orthop Surg Traumatol 2018;28:1191-7. [Google Scholar] [PubMed]
- 8. Binkley JM, Stratford PW, Lott SA, Riddle DL. The lower extremity functional scale (LEFS): Scale development, measurement properties, and clinical application. North American orthopaedic rehabilitation research network. Phys Ther 1999;79:371-83. [Google Scholar] [PubMed]
- 9. Motsitsi N. Masquelet’s technique for management of long bone defects: From experiment to clinical application. East Cent Afr J Surg 2012;17:43-47. [Google Scholar] [PubMed]
- 10. Hatashita S, Kawakami R, Ejiri S, Sasaki N, Toshiki N, Ito M, et al. ‘Acute Masquelet technique’ for reconstructing bone defects of an open lower limb fracture. Eur J Trauma Emerg Surg 2021;47:1153-62. [Google Scholar] [PubMed]
- 11. Lenze U, Kasal S, Hefti F, Krieg AH. Non-vascularised fibula grafts for reconstruction of segmental and hemicortical bone defects following meta- /diaphyseal tumour resection at the extremities. BMC Musculoskelet Disord 2017;18:289. [Google Scholar] [PubMed]
- 12. Gannamani S, Rachakonda KR, Tellakula Y, Takkalapally H, Maryada VR, Gurava Reddy AV. Combining non-vascularized fibula and cancellous graft in the Masquelet technique: A promising approach to distal femur compound fracture management with large defects. Injury 2024;55:111233. [Google Scholar] [PubMed]
- 13. Gouron R, Deroussen F, Plancq MC, Collet LM. Bone defect reconstruction in children using the induced membrane technique: A series of 14 cases. Orthop Traumatol Surg Res 2013;99:837-43. [Google Scholar] [PubMed]
- 14. Yadav AK, Pawar E, Prasanna Kumar GS, Mane A, Harssor A, Shet V, et al. Functional outcome of non-vascularized fibula in gap non union. Int J Res Orthop 2019;6:205-8. [Google Scholar] [PubMed]
- 15. Karger C, Kishi T, Schneider L, Fitoussi F, Masquelet AC, French Society of Orthopaedic [Google Scholar] [PubMed]
- 16. (SoFCOT). Treatment of posttraumatic bone defects by the induced membrane technique. Orthop Traumatol Surg Res 2012;98:97-102. [Google Scholar] [PubMed]
- 17. Jayaramaraju D, Venkataramani H, Rajasekaran RB, Agraharam D, Sabapathy SR, Rajasekaran S. Modified Capanna’s technique (vascularized free fibula combined with allograft) as a single-stage procedure in post-traumatic long-segment defects of the lower end of the femur: Outcome analysis of a series of 19 patients with an average gap of 14 cm. Indian J Plast Surg 2019;52:296-303. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Aneurysmal Bone Cyst of the Proximal Humerus Managed with En Bloc Resection, Fibular Strut Grafting, and PHILOS Fixation: A Case Report
July 1, 2026 Aneurysmal Bone Cyst of the Proximal Humerus Managed with En Bloc Resection, Fibular Strut Grafting, and PHILOS Fixation: A Case Report July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis
July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis June 1, 2026 Revision Reconstruction of a Humeral Simple Bone Cyst Using Fibular Strut Graft, Iliac Crest Bone Graft, and Posterior Plating in a Young Adult: A Case Report
June 1, 2026 Revision Reconstruction of a Humeral Simple Bone Cyst Using Fibular Strut Graft, Iliac Crest Bone Graft, and Posterior Plating in a Young Adult: A Case Report May 1, 2026 Suprapatellar Tibial Nailing in Skeletally Immature Patients: A Case Series
May 1, 2026 Suprapatellar Tibial Nailing in Skeletally Immature Patients: A Case Series